
A comparison of SphygmoCor and Vicorder devices for measuring aortic pulse wave velocity in pregnancy
- DOI
- 10.1016/j.artres.2012.01.003How to use a DOI?
- Keywords
- Pulse wave velocity; Aortic stiffness; Pregnancy; SphygmoCor; Vicorder
- Abstract
Background: Aortic pulse wave velocity (aPWV) has been found to be increased in preeclampsia when compared to normal pregnancy. Preeclampsia is associated with increased risk of later cardiovascular disease and, as such, study of the aortic stiffness in pregnancy, and its hypertensive disorders, is important to the understanding the underlying vascular changes. We compared two different techniques to measure aPWV in the mid-trimester of pregnancy.
Methods: 58 women were recruited from the obstetric ultrasound clinic, mean (±SD) age 33 (±6) years and gestation 27 (±1) weeks. Aortic PWV was measured using SphygmoCor and Vicorder devices.
Results: We found that both devices provided similar aPWV values with no significant difference between devices: mean difference (±SD), 0.1 (±0.9)m/s, p = 0.4. We found good correlation between devices (r = 0.6, p < 0.001). Good intra-observer variability was observed for both SphygmoCor and Vicorder devices, coefficients of variation 5.69% and 2.67%, respectively.
Conclusions: The SphygmoCor and Vicorder devices produce similar readings for aPWV in the second trimester of pregnancy, with good intra-observer variability. Due to its simpler technique the Vicorder device may be more suited to the clinical setting, particularly in advanced pregnancy or obesity.
- Copyright
- © 2012 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
Women who have had a pregnancy complicated by preeclampsia are at increased risk of cardiovascular disease in later life.1 A number of mechanisms may be responsible for this such as shared risk factors2,3 or a direct effect of preeclampsia itself on the cardiovascular system. Interestingly a number of surrogate markers of cardiovascular disease such as endothelial dysfunction and increased arterial stiffness have been reported in women with previous preeclampsia.4,5 In light of this there has been increasing interest in assessing arterial and aortic stiffness in pregnancy, particularly prior to the onset of preeclampsia or other associated pregnancy complications such as intra-uterine growth retardation. Aortic stiffness is an independent risk factor of cardiovascular disease in several populations.6
Aortic pulse wave velocity (aPWV) is the “gold-standard”7 measure of aortic stiffness and can be assessed non-invasively. In practical terms, aPWV is assessed as the distance from carotid pulse to the femoral pulse divided by the time taken to travel that distance. Several devices are available to measure aPWV. Although the SphygmoCor system (AtCor Medical, West Ryde, NSW, Australia) is widely used, it requires an experienced operator and is intrusive in that it requires exposure and palpation of the femoral artery and attachment of ECG leads to the chest. The Vicorder device (Skidmore Medical Ltd, Bristol, UK) requires little operator training and does not require exposure of the groin or chest. These features of the Vicorder make it an attractive option in pregnancy and for research in clinical settings. Both devices are non-invasive and have good correlation and repeatability in an older, non-pregnant population.8,9 The aim of this study was to examine whether aPWV measured using these devices is correlated and repeatable in a younger population in pregnancy – a state of profound cardiovascular adaptation.
Methodology
58 women in the second trimester of pregnancy were recruited from an obstetric ultrasound clinic at Cambridge University Hospitals NHS Trust in the UK between June and December 2010. Women returned on a separate occasion for assessment of cardiovascular parameters. Ethics approval for the study was granted by the local research ethics committee.
Women rested supine for 10 min in a 30° left lateral position to avoid aorto-caval compression by the gravid uterus in a quiet temperature controlled room before measurements were taken. Blood pressure was recorded using a Omron M7 automated sphygmomanometer, which has been validated in pregnancy.10 Sequential recordings using ECG-gated applanation tonometry of the carotid and femoral artery pressure waveforms as previously described8,9 was used to determine the aPWV with the SphygmoCor device. A total of 10 s of high-quality waveforms were captured for each reading, and the intersecting tangents algorithm was applied to determine the foot-to-foot transit time using the integrated software and the R wave as a reference frame. Path length was calculated as the distance from the femoral measurement site to the supra-sternal notch minus the distance from the carotid site to the supra-sternal notch. The notch-femoral distance was measured using callipers to avoid measuring over the gravid uterus which would falsely inflate the path length.
A volume displacement method was then used to determine the aPWV using the Vicorder device. A 100 mm wide blood pressure cuff was placed around the upper thigh to measure the femoral pulse and a 30 mm partial cuff around the neck at the level of the carotid artery. The cuffs were each inflated to 60 mmHg, and high-quality waveforms were recorded simultaneously for 3 s as previously described.8 The foot-to-foot transit time was determined using an in-built cross-correlation algorithm centred around the peak of the second derivative of pressure. Path length was defined as the distance from the supra-sternal notch to the top of the thigh cuff. As discussed previously, callipers were used to measure this distance.
Blood pressure readings were taken following placement of ECG electrodes and leads and measurement of the notch-femoral and notch-carotid distances. Readings using the SphygmoCor system were then taken at the carotid and femoral pulse sites. After successful readings, the ECG leads were removed and the Vicorder thigh cuff attached to the participant. The path distance for the Vicorder device was measured and the neck cuff attached. Vicorder readings were performed and were recorded within 5 min of the SphygmoCor readings. The left femoral and carotid sites were used for all measurements and all readings were performed in duplicate. These duplicate readings were used for assessing the repeatability of aPWV measurement of each device. Both techniques were well tolerated.
Statistics
Agreement between SphygmoCor and Vicorder values was analyzed by Bland–Altman plots11 with mean difference ± SD values reported. Absolute values were compared with Student’s paired t-tests. Linear regression by the method of ordinary least squares was used to define the correlation between SphygmoCor and Vicorder values. Goodness of fit is expressed by Pearson’s correlation coefficient (r). Statistical analysis was performed using MedCalc v11.6 (Mariakerke, Belgium).
Results
Basic demographic, pregnancy and haemodynamic data are summarised in Table 1
| Parameter | Mean ± SD | Range |
|---|---|---|
| Age (years) | 33 ± 6 | 19–42 |
| Gestation (weeks) | 27 ± 1 | 24–30 |
| Height (cm) | 165 ± 7 | 150–187 |
| Weight (kg) | 68 ± 8 | 44–106 |
| Body Mass Index (kg/m2) | 24 ± 6 | 17–37 |
| Systolic blood pressure (mmHg) | 107 ± 12 | 85–139 |
| Diastolic blood pressure (mmHg) | 68 ± 8 | 49–91 |
| Mean blood pressure (mmHg) | 81 ± 10 | 61–110 |
| Pulse pressure (mmHg) | 88 ± 7 | 20–60 |
| Heart rate (beats min−1) | 82 ± 9 | 58–105 |
| Nulliparous/Multiparous | 31/27 |
Participant demographic, pregnancy and haemodynamics details.
Comparison of Vicorder and SphygmoCor aPWV
The mean aPWV recorded by the Vicorder device was 5.4 ± 1.0 (Range 3.1–8.4 m/s) and using the SphygmoCor device was 5.5 ± 0.7 m/s (range 4.1–7.6 m/s). The mean difference between devices was 0.1 ± 0.9 m/s, p = 0.4 (Fig. 1a). Overall there was reasonable correlation between the Vicorder and SphygmoCor devices, r = 0.6, p < 0.001 (Fig. 1b).
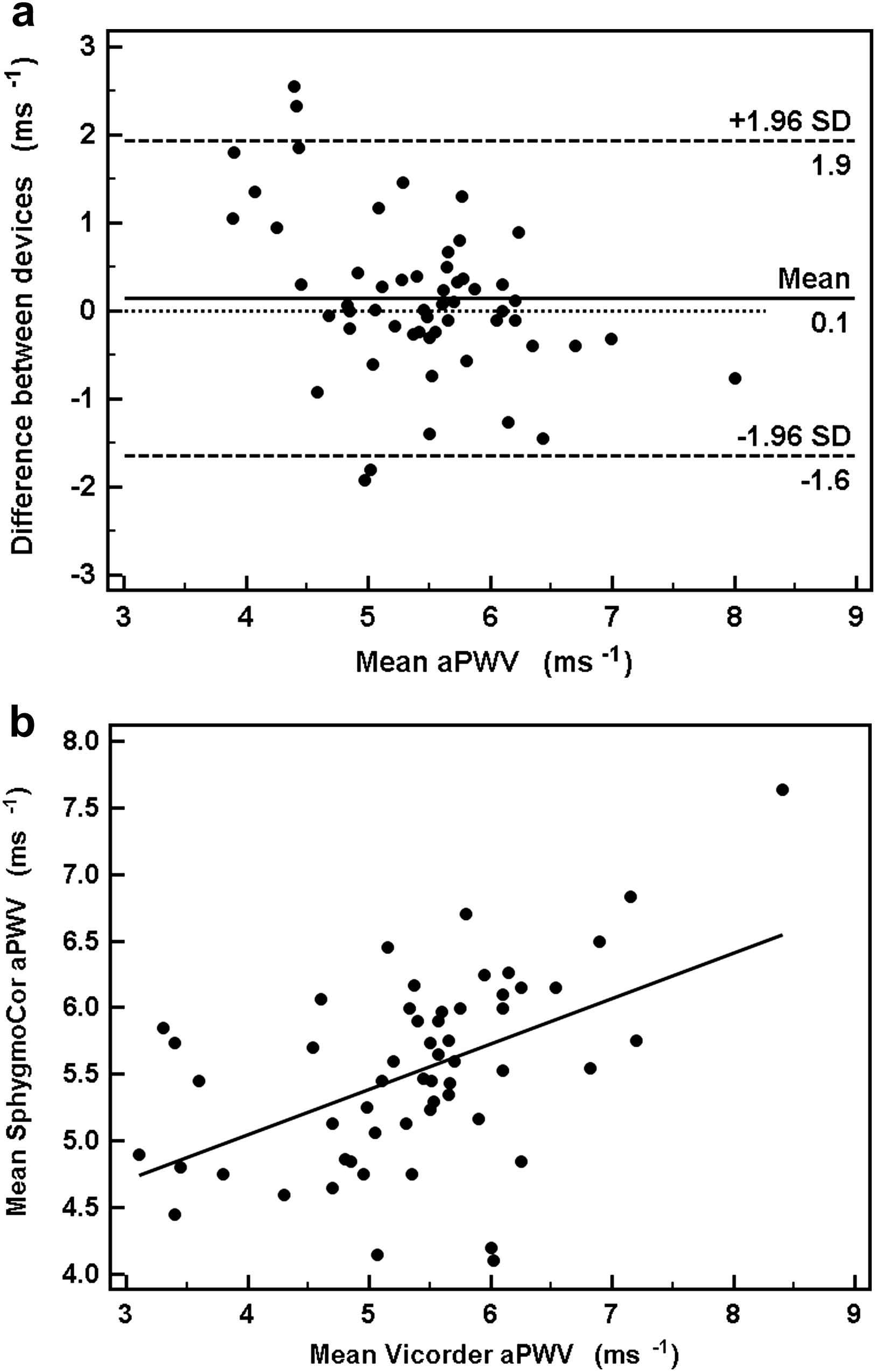
Relationship between SphygmoCor and Vicorder devices. Bland–Altman plot (a) demonstrates a mean (±SD) inter-device difference of 0.1 (±0.9)m/s, p = 0.4. (b) Correlation between the SphygmoCor and Vicorder aPWV readings, r = 0.6, p < 0.001.
Intra-observer variability
The mean differences for aPWV were (mean ± SD) 0.02 ± 0.45 m/s, for the SphygmoCor device and 0.03 ± 0.19 m/s for the Vicorder device. The coefficients of variation were 5.69% and 2.67% respectively. The Bland–Altman plots for the intra-observer variability show no tendency for the reproducibility of the measurement to vary with the underlying mean value (Fig. 2).
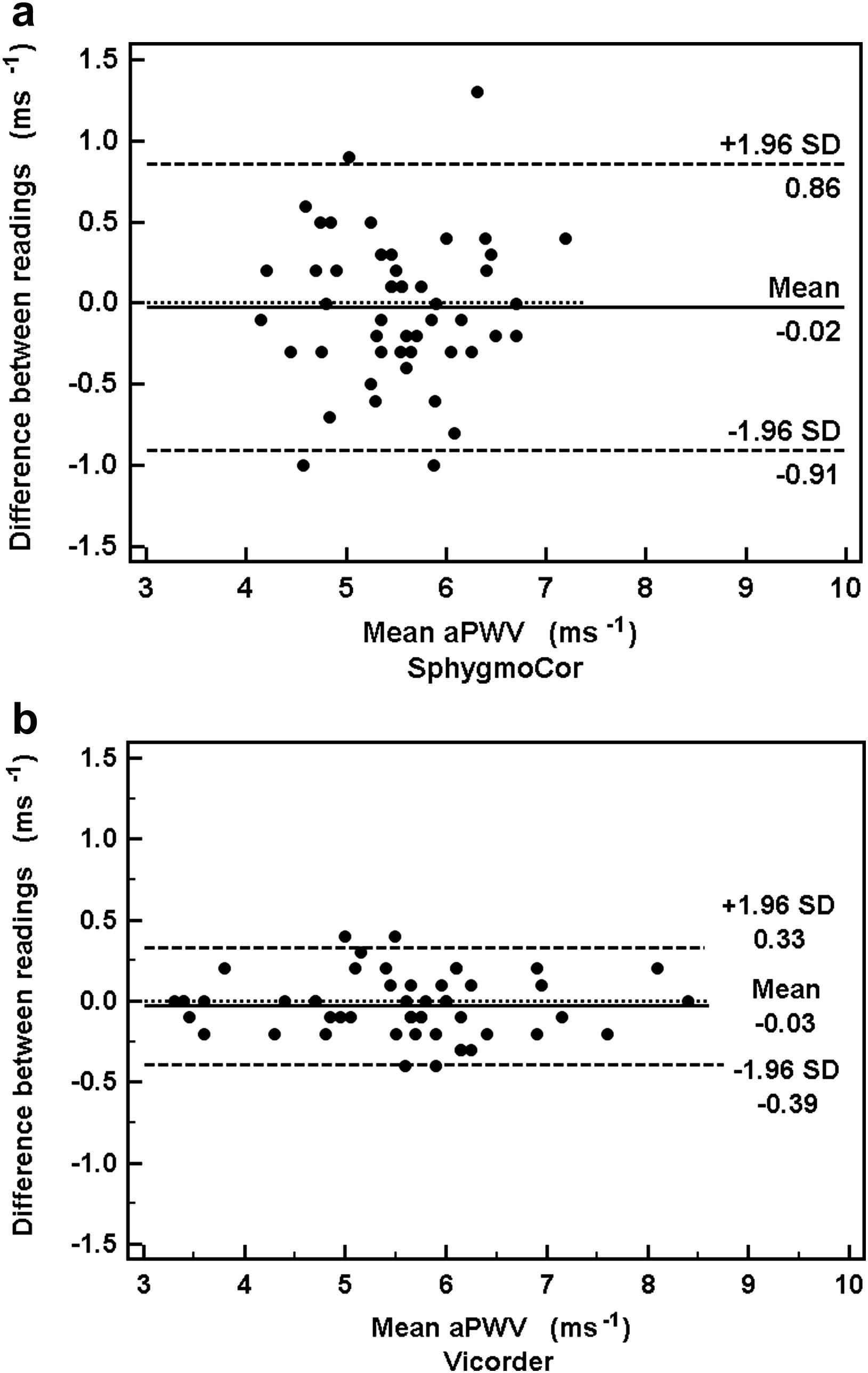
Intra-observer differences between duplicate readings using the SphygmoCor and Vicorder devices. Bland–Altman plot demonstrates a mean (±SD) intra-observer difference for (a) the SphygmoCor device of 0.02 (±0.45)m/s and (b) the Vicorder device 0.03 (±0.19)m/s.
Discussion
This study shows that in pregnant women aortic PWV measurements obtained using the Vicorder device, using an oscillometric technique, have a very good agreement with measurements obtained using the widely used SphygmoCor system, that uses an ECG-gated tonometric technique. The ARTERY society has set out accuracy criteria for comparison of devices.12 To attain an accuracy criteria of “excellent”, mean difference should be ≤0.5 m/s and SD ≤ 0.8 m/s whilst a mean difference of <1 m/s and SD ≤ 1.5 m/s is deemed acceptable. As such, our study shows excellent inter-device mean difference for measurement of aPWV by Vicorder and SphygmoCor in this particular population, although the SD falls within the “acceptable” range. Good intra-observer variability for both the devices has been demonstrated in the general population8 and a younger population of adolescents and children.13 Our results extend this finding to the pregnant population and demonstrate coefficients of variation that compare favourably with other studies for both devices.8,13,14 The Vicorder device shows better within operator repeatability.
Previous studies in non-pregnant populations have reported good correlation between the SphygmoCor and Vicorder devices.8,13,15 In the present study we find that this good correlation and acceptable limits of agreement holds true in pregnant women and that the parameters of agreement are similar to other studies.
The range of aPWV values we observed a similar to those previously measured in a normotensive pregnant population.16,17 It has been previously noted,8,15 there does appear to be a tendency for the Vicorder device to record lower values than the SphygmoCor device at higher aPWV ranges.8,15 In the present study, we did not clearly observe this phenomenon. A likely explanation is that the values observed in pregnancy are considerably lower than in a general population, therefore outside of the range at which this occurs.
There has also been considerable discussion regarding the correct measurement of the carotid-femoral length for all devices and, in respect to the Vicorder device, where the exact point of measurement of the femoral pulse is. In this study all measurements for Vicorder were made from the supra-sternal notch to the top of the femoral cuff, as per the manufacturer’s recommendation at the time of study, using callipers. Whilst there may be small differences between using the top of the thigh cuff or the mid-point of the thigh cuff, the use of either has been shown to have good agreement with the SphygmoCor in both adults and children.8,15 Through necessity, to avoid extension of the path length by measuring over the gravid uterus, the supra-sternal notch to femoral measurements in pregnancy must be taken using callipers. This method should provide similar accuracy of path length measurement to measurements made in the standard way in a non-pregnant, non-obese subject.
The present study was performed as a sub-study of aortic stiffness in pregnancy and all reading performed by the same operator (TE). For this reason the devices were used in a fixed order and the operator not blinded to the result of the first set of readings. As such measurement bias cannot be completely excluded. However both the SphygmoCor and Vicorder software generate measurements in an operator independent manner.
The pulse wave velocity measurements of the SphygmoCor device have not been formally validated against invasive techniques, though SphygmoCor has been shown to have good correlation with invasive cfPWV measurement.18 Similarly, whilst the Vicorder device has not been validated invasively, it has good correlation (r = 0.59) with cine-phase contrast MRI, though readings using Vicorder were slightly lower (0.7 m/s) than when calculated using the MRI technique.19 Indeed, most of the commercially available devices have not been validated against invasive techniques and, whilst this information would be of great value, for ethical reasons, this validation is extremely unlikely to occur in a pregnant population. As such the most widely used device, SphygmoCor, has become the default standard. SphygmoCor pulse wave velocity measurements have been shown to be comparable to Arteriograph (TensioMed, Hungary) measurements, which uses an oscillometric technique.20–22 However, this finding of close agreement between Arteriograph and SphygmoCor is not universal23 and we note the ongoing discussions regarding the Arteriograph technique.24 Similarly, comparison of the Complior device (Artech Medical, Pantin, France), which uses a piezo-electric method, to SphygmoCor has shown good correlation.25 Bland–Altman analysis revealed a tendency to higher values in the Complior readings, a finding repeated in another study21 and probably attributable to the differences in algorithm to detect transit time. (We are not aware of any direct comparisons of other methods, e.g. PulsePen, with SphygmoCor or Vicorder). The close agreement that we demonstrate between SphygmoCor and Vicorder compares favourably to similar comparisons of aPWV measurement. This provides a degree of reassurance that the values measured by the Vicorder in pregnancy are representative of the aPWV. Another source of error is possible when the diastolic blood pressure (DBP) of the subject is below 60 mmHg (the cuff inflation pressure of the Vicorder device) as this may lead to deterioration in the waveforms obtained. There were ten women with DBP below 60 mmHg in our study, of which only two had DBP <55 mmHg.
aPWV is an independent predictor of cardiovascular risk6 and preeclampsia is known to be associated with long term increased risk of cardiovascular disease.1 Increased aPWV is seen in both active preeclampsia26 and those at high risk of developing the disease.17 Further research is required to establish whether the increase in aortic stiffness is evident prior to conception in these women or whether it is a phenomenon that develops during a preeclamptic pregnancy and, to some extent, persists post-partum. In order to do this, larger longitudinal clinical studies from pre-pregnancy to post-partum are required. This would require large numbers of women and reliable, time-efficient measurement techniques.
In summary, the findings of this study indicate that both the Vicorder and SphygmoCor produce similar results in pregnancy and that the previously observed good repeatability is maintained in this specific population. Either device can be used successfully in pregnancy and both are well tolerated. However, for research that is taking place in the clinical environment such as the antenatal clinic or labour ward, the Vicorder may be the more practical device, given that it requires less skill, less patient exposure and less time to perform the measurements.
Author contribution
TRE performed the study; TRE, CMM, IBW were involved in the analysis and interpretation of the study; TRE wrote the first draft of the manuscript; All authors contributed to the writing of the manuscript.
Funding
TRE is funded by the Evelyn Trust. CCL is recipient of an Evelyn Trust research grant. IBW and CMM are both British Heart Foundation Fellows. AMM is supported by Cambridge Fetal Care. CMM and IBW are supported by the Cambridge Biomedical Research Centre (NIHR). IBW has received unrestricted educational support (all <£10,000 pa) from AtCor, Vicorder and IEM in the past 5 years.
References
Cite this article
TY - JOUR AU - T.R. Everett AU - A. Mahendru AU - C.M. McEniery AU - C.C. Lees AU - I.B. Wilkinson PY - 2012 DA - 2012/01/21 TI - A comparison of SphygmoCor and Vicorder devices for measuring aortic pulse wave velocity in pregnancy JO - Artery Research SP - 92 EP - 96 VL - 6 IS - 2 SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2012.01.003 DO - 10.1016/j.artres.2012.01.003 ID - Everett2012 ER -