
The addition of whole-body vibration to a lifestyle modification on arterial stiffness in overweight and obese women
- DOI
- 10.1016/j.artres.2012.01.006How to use a DOI?
- Keywords
- Arterial stiffness; Obesity; Pentraxin 3; Whole-body vibration
- Abstract
Background: Increased arterial stiffness is an independent risk factor for cardiovascular disease. Arterial stiffness increases in obese individuals as compared to normal weight. While weight loss by calorie-restriction alone decreases arterial stiffness in obesity, it decreases muscle mass. Resistance training is recommended treatment for this frailty, but it can also increase arterial stiffness. Whole-body vibration (WBV) has recently been indicated as an alternative for resistance training. The present study aimed to examine whether lifestyle modifications combined with WBV decrease arterial stiffness in overweight and obese women.
Methods: Twelve overweight and obese women (age: 30–48 years) completed a 12-week lifestyle-modification program (1200kcal/day diet, brisk walking for 30 min, 3 days/week) and WBV (30–35 Hz, 30 min, 3 days/week).
Results: Before and after this program, we measured body weight and indices of arterial stiffness, i.e., carotid-femoral pulse wave velocity (cfPWV) and brachial-ankle PWV (baPWV). Body weight, cfPWV, and baPWV of the overweight and obese women significantly decreased after this intervention. The concentration of plasma pentraxin 3, which has a cardioprotective effect, significantly increased after the program.
Conclusion: We recommend the addition of WBV to classical lifestyle modifications to decrease arterial stiffness, which would reduce the risk of cardiovascular disease and muscle weakness in obese individuals.
- Copyright
- © 2012 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
Obesity is known to be an independent risk factor for cardiovascular disease.1–3 Increased arterial stiffness is also known as an independent risk factor for cardiovascular morbidity and mortality.4,5 It has already been reported that arterial stiffness in obese individuals is higher than that in individuals with a normal weight.6,7 Previously, we have reported that dietary modification can induce remarkable weight loss and lowering of arterial stiffness in obese subjects.8 However, diet modification alone decreases not only adipose tissue but also muscle mass and muscle strength.9 Inclusion of exercise training in lifestyle modification is important for preventing a decrease in fat-free mass, increasing relative visceral fat-mass loss, improving dietary compliance, and maintaining long-term weight control.10 We have previously reported that habitual aerobic exercise can decrease arterial stiffness in obese subjects.11 Moreover, habitual aerobic exercise has a cardioprotective effect, as indicated by the increased in plasma pentraxin 3 (PTX3) concentration.12 Compared to dietary modification, habituation of aerobic exercise alone is often insufficient to induce marked weight loss.9 However, it is well known that a combination of diet modification and aerobic exercise is more effective than diet modification alone to induce weight loss, resulting from increased energy expenditure, in obese individuals.13
Aging is also associated with loss of muscle mass and strength, even in subjects of a normal weight, because of a decrease in physical activity level.14,15 Not only aging but also obesity decrease in muscle mass, and the loss of muscle mass may be associated with deleterious health outcomes, e.g., muscle weakness and insulin resistance.15 Obesity and sarcopenia in older adults may potentiate each other and maximize their effects on physical disability, morbidity, and mortality.14 It is therefore important to prevent a decrease in muscle mass and to decrease adipose tissue for weight loss in middle-aged obese individuals. Although resistance training itself does not induce fat-mass loss, it prevents the loss of muscle mass and increases the resting metabolic rate.9 Moreover, resistance training increases muscle mass and may improve glucose and insulin responses to a glucose load in healthy subjects and patients with diabetes.16 Previous studies have recommended weight loss through dietary modification, aerobic exercise training, and muscle strength training in obese individuals.9 Some studies, however, have indicated that resistance training increases arterial stiffness.17,18 To resolve these contradictory points, novel resistance-training methods that cause neither loss of muscle strength nor increased arterial stiffness are needed for weight loss in obese subjects.
Recently, whole-body vibration (WBV) has been developed as a novel means of muscular strength training. The effects of 12-week WBV training appear similar to those of resistance training in young women and in middle-aged and elderly individuals.19,20 However, in contrast to the effect of resistance training on arterial stiffness as described above, Otsuki et al. have reported that transient WBV decreases arterial stiffness.21 Therefore, WBV training, as instead of resistance training, may become useful tool to cause neither loss of muscle strength nor increased arterial stiffness in obese subjects who are needed for weight loss. Especially, a combination of WBV training and a classical lifestyle-modification weight loss program aerobic exercise might be effective. However, whether the addition of WBV training to dietary restriction and aerobic exercise decreases arterial stiffness in obese individuals remains unknown entirely. Taken together, the present study was undertaken to examine whether incorporation of WBV training in a classical lifestyle-modification weight loss program decreases arterial stiffness in premenopausal overweight and obese women. Furthermore, we measured concentrations of plasma PTX3 before and after the intervention.
Methods
Subjects
Twelve premenopausal sedentary overweight and obese women participated in the study (age: 42±2 years; body mass index [BMI]: 32±1kg/m2). Candidates who were current smokers, who were taking any medications or who had regular exercise habit were excluded. No subjects had apparent cardiovascular disease, as assessed by medical history and physical examination. This study was reviewed and approved by the Institutional Review Board at the University of Tsukuba. All potential risks and procedures of the study were explained to the subjects who provided written informed consent to participate in the study.
Experimental design
All participants were studied before and after a 12-week lifestyle-modification weight-reduction program (dietary modification, aerobic exercise training, and WBV). Dietary intake was assessed by 3-day weighed dietary records, and dietary recall interviews by a skilled dietician for each subject at the baseline and at the beginning of week 10 of the intervention. All measurements were performed after abstinence from caffeine and an overnight fast. The subjects were studied in supine resting conditions in a quiet, temperature-controlled room (24–26°C). All measurements were performed after a resting period of at least 20 min.
Dietary modification
The chosen protocol has been reported as a low-calorie diet intervention with effects on body composition, body-fat distribution, and coronary heart disease risk factors.8,22 Based on the diet protocol, all participants were instructed to take meals consisting, on average, of 300 kcal of protein, 600 kcal of carbohydrate, and 300 kcal of fat per day (total: 1200 kcal/day). The subjects maintained daily food diaries during the 12-week intervention period and learned about proper daily nutrition (well-balanced protein, carbohydrate, fat, amino acids, vitamins, and minerals) through weekly lectures and counseling by skilled dieticians.
Aerobic exercise training
The subjects underwent aerobic exercise training in the form of brisk walking for sessions of 30 min each (3 days/week); the subjects were supervised by two or three physical trainers. Each training session began with 15–30 min of warm-up activities such as stretching and ended with 15–30 min of cool-down activities. The subjects measured their heart rates (HRs) with portable heart-rate monitors (s-610i, Polar Electro OY, Oulu, Finland) while walking, and recorded the duration (min) and intensity (HRs) during each exercise session. The walking intensity was started with 45% of the maximum HR. The intensity was gradually increased, and finally targeted to 70–75% of the maximum HR, which represents moderate intensity.
WBV training
A total-body WBV training program comprised unloaded static and dynamic exercises on the vibration platform (Power Plate®, Badhoevendorp, The Netherlands). Frequency and amplitude of the vertical sinusoidal vibrations produced from vibration platform were at 30–35 Hz and 2.0 mm. The lower-body exercises included high squat and deep squat and wide-stance squat and lunge. The duration of the WBV training was 3 days/week for 30 min; each interval of vibration lasted 30 s. The break period between vibration intervals was fixed at 30 s throughout the intervention. Training volume and training intensity were low at the beginning, but progressed slowly according to the overload principle. Briefly, in the first month, the training consisted of unloaded static exercise with a light frequency (30 Hz) of vibration. In the second month, the training intensity was increased by increasing the frequency of the vibration to 35 Hz. In the last month, the training intensity was increased by changing from static to dynamic exercises.
Pulse wave velocity and blood pressure
Carotid-femoral pulse wave velocity (cfPWV), brachial-ankle PWV (baPWV) and blood pressure measurements were performed in the supine position after 20 min rest using an automatic waveform analyzer (form PWV/ABI, Colin Medical Technology, Komaki, Japan). cfPWV was measured using applanation tonometry, as previously described.8 Briefly, carotid and femoral arterial pulse waves were obtained in triplicate by using arterial applanation tonometry, incorporating an array of 15 transducers. The distance traveled by the pulse waves was assessed in triplicate with a random zero-length measurement over the surface of the body with a non-elastic tape measure. Pulse wave transit time was determined from the time delay between the proximal and distal “foot” waveforms. The foot of the wave was identified as the commencement of the sharp systolic upstroke, which was automatically detected. cfPWV was calculated as the distance divided by the transit time. Brachial-ankle PWV (baPWV) was obtained in triplicate by using modified oscillometric pressure-sensor method.23 Briefly, bilateral brachial and post-tibial arterial pressure waveforms were stored for 10 s by extremities cuffs connected to an oscillometric pressure sensor wrapped on both arms and ankles inflating at a low pressure, during the measurement of cfPWV.
Plasma pentraxin 3 concentration
Plasma pentraxin 3 (PTX3) was measured as previously described.12 Briefly, each blood sample was placed in a chilled tube containing ethylenediaminetetraacetic acid (2mg/mL) and was then centrifuged at 2000g for 15min at 4°C. The plasma was stored at −80°C until assay. Plasma concentrations of plasma PTX3 were determined using a commercial enzyme-linked immunosorbent assay (ELISA) kit (Quantikine DPTX 30, R&D Systems Inc., Minneapolis, USA). The PTX3 assay was carried out according to the manufacturer’s instructions.
Blood biochemical analysis
The serum concentrations of total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides, and the plasma concentrations of glucose were determined using standard enzymatic techniques.
Peak oxygen uptake
Peak oxygen uptake (
Body composition by DEXA
DEXA (DPX-L, Lunar, WI, USA) was used to evaluate segmental body composition (i.e., upper limbs, trunk, lower limbs, and whole body), which consisted of fat mass (FM) and fat-free mass (FFM). Transverse scans were used to measure FM and FFM, and pixels of soft tissue were used to calculate the ratio of mass attenuation coefficients at 40–50keV (low energy) and 80–100keV (high energy), using software version 1.3Z.
Statistical analysis
Data are expressed as mean±SE. To evaluate differences in values before and after the program in overweight and obese women, Student’s t-test for paired values was used. Relationships between BMI and plasma PTX3 concentrations were analyzed using Pearson’s correlation. P<0.05 was accepted as significant.
Results
The characteristics of premenopausal overweight and obese women before and after 12 weeks of the lifestyle-modification program are summarized in Table 1. Body weight, BMI, waist circumference, and the percentage of fat body mass markedly decreased after the intervention. On the other hand, the percentage of lean body mass and peak oxygen uptake significantly increased after the program. Serum concentrations of total cholesterol, LDL cholesterol, and triglycerides also significantly decreased. Additionally, systolic blood pressure, diastolic blood pressure, mean arterial pressure, and heart rate were significantly lowered after the intervention (Table 2). Importantly, the cfPWV and baPWV also significantly decreased after these lifestyle modifications (Fig. 1). The addition of WBV training to a lifestyle-modification program in overweight and obese women thus decreased arterial stiffness. Furthermore, the plasma PTX3 concentration, which is recognized as an index of cardioprotection, significantly increased after the lifestyle modifications (Fig. 2). The relationship between plasma PTX3 concentrations and BMI was linear (R=−0.59, P<0.05) (Fig. 3). However, there was no relationship between plasma PTX3 concentrations and total fat mass (R=−0.41, P=0.20).
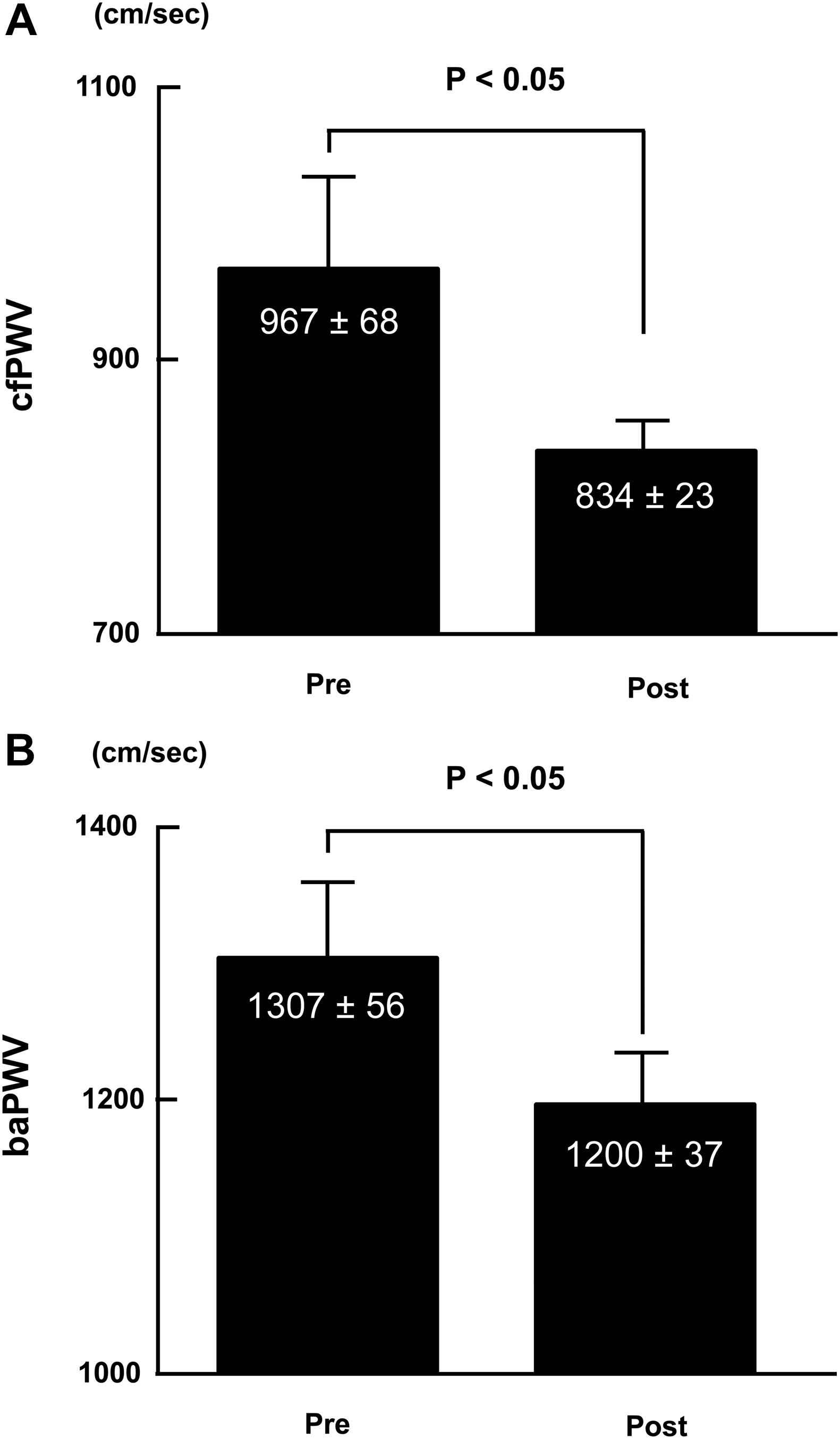
Arterial stiffness before and after a 12-week lifestyle-modification program incorporating whole-body vibration (WBV). (A) Carotid-femoral pulse wave velocity (PWV). (B) Brachial-ankle PWV. Data are expressed as mean±SE.
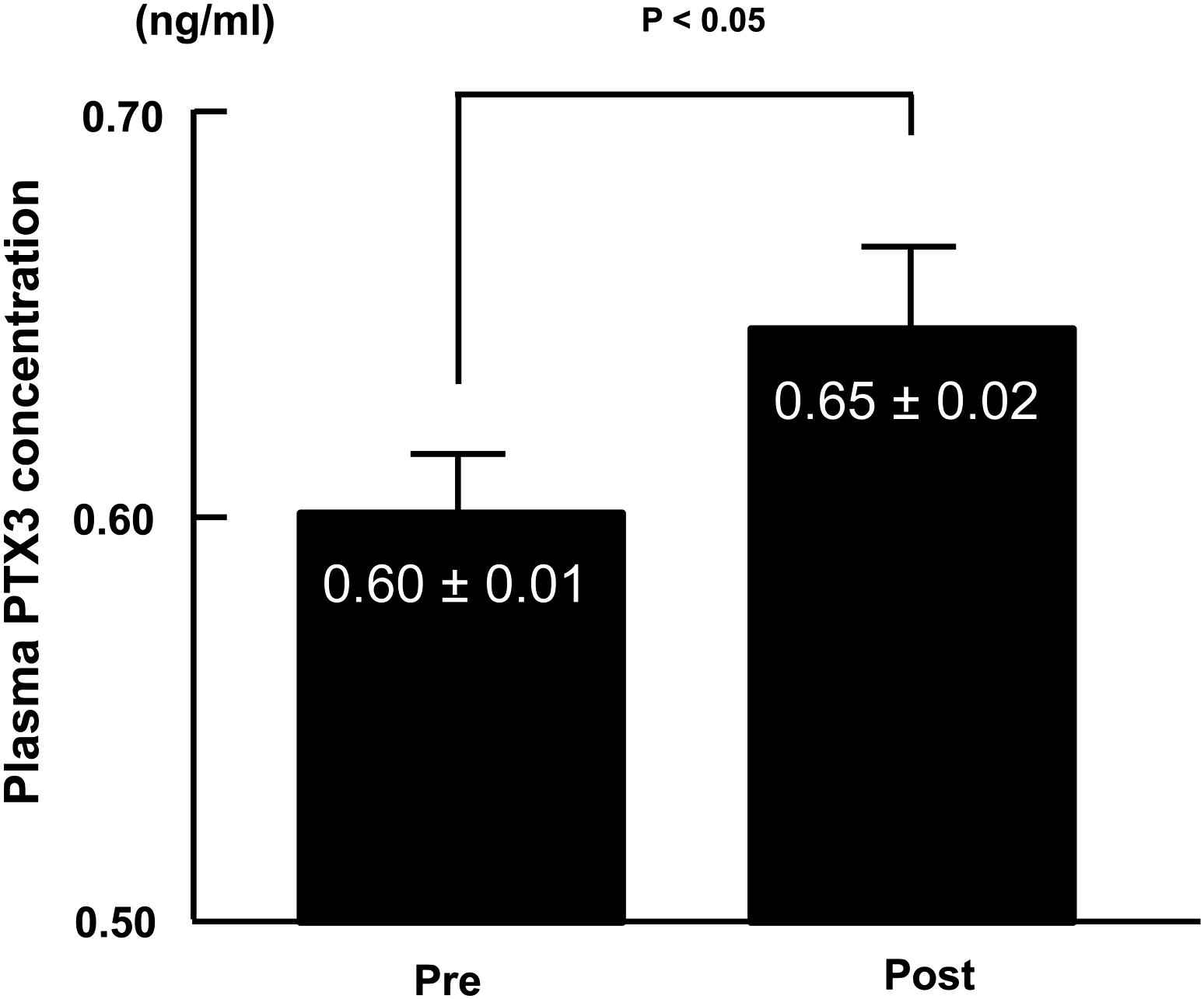
Plasma pentraxin 3 (PTX3) concentration before and after a 12-week lifestyle-modification program incorporating WBV. Data are expressed as mean±SE.
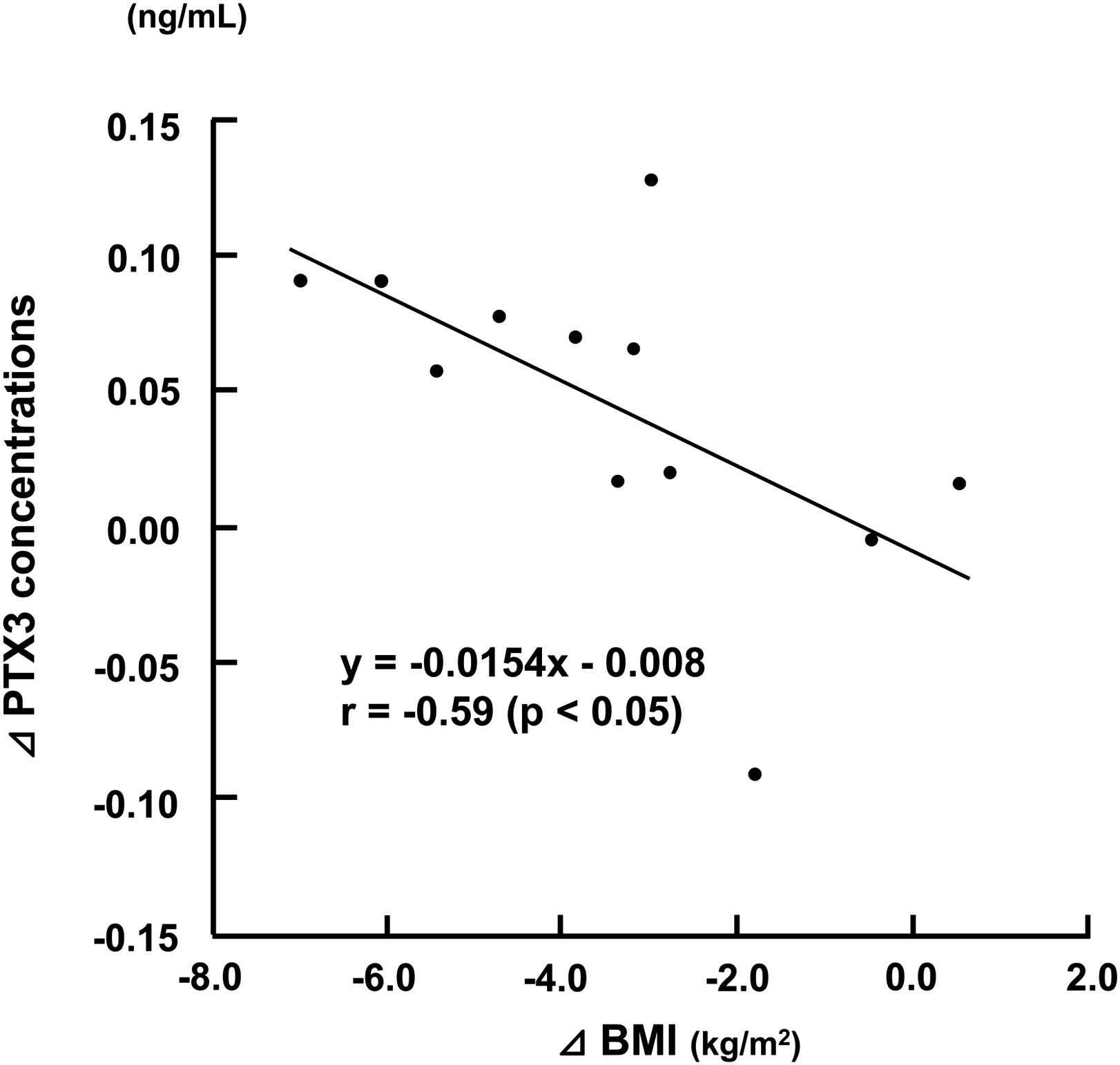
Relationship between changes in plasma PTX3 concentrations and body mass index. Data are expressed as mean±SE.
| PRE | POST | |
|---|---|---|
| Body weight, kg | 80.5±4.1 | 71.8±3.3** |
| BMI, kg/m2 | 32.1±1.3 | 28.7±1.0** |
| Waist circumference, cm | 103.8±2.6 | 92.8±2.2** |
| Percentage of fat body mass, % | 36.8±2.0 | 33.7±1.4* |
| Percentage of lean body mass, % | 61.0±2.7 | 63.2±2.4* |
| Total cholesterol, mg/dl | 222±9 | 200±8** |
| HDL cholesterol, mg/dl | 55±4 | 55±4 |
| LDL cholesterol, mg/dl | 141±6 | 124±6** |
| Triglyceride, mg/dl | 131±12 | 102±14* |
| Fasting blood glucose, mg/dl | 93±2 | 93±2 |
| Peak oxygen uptake, ml/min/kg | 22.2±1.7 | 28.1±1.1** |
Data are expressed as means±SE.
P<0.05,
P<0.01 vs. before the intervention.
Characteristics of premenopausal overweight and obese women before and after 12-week lifestyle modification.
| PRE | POST | |
|---|---|---|
| Systolic blood pressure, mmHg | 134±5 | 123±4** |
| Mean blood pressure, mmHg | 101±4 | 92±3** |
| Diastolic blood pressure, mmHg | 82±3 | 76±2* |
| Pulse pressure, mmHg | 51±2 | 47±3 |
| Heart rate, bpm | 74±4 | 64±2* |
Data are expressed as means±SE.
P<0.05,
P<0.01 vs. before the intervention.
Hemodynamic of premenopausal overweight and obese women before and after 12-week lifestyle modification.
Discussion
In the present study, we examined whether the addition of WBV training to a 12-week lifestyle-modification program decreased arterial stiffness in premenopausal overweight and obese women. After the program was completed, the cfPWV, an index of central arterial stiffness, and the baPWV, a total-body index of arterial stiffness, significantly decreased in premenopausal overweight and obese women. Weight reduction in these women, by a lifestyle-modification program that includes WBV training, thus decreased arterial stiffness. We have also shown that the addition of WBV training to classical lifestyle modifications significantly increases the plasma PTX3 concentration, an anti-inflammatory and cardioprotective index, in overweight and obese women. We therefore infer that the mechanism underlying the decrease in arterial stiffness by the 12-week lifestyle-modification program incorporating WBV, is associated with an enhancement of anti-inflammatory and cardioprotective effects.
Obesity is strongly associated with cardiovascular diseases.1–3 On the other hand, elevated arterial stiffness has been implicated in the pathophysiology of cardiovascular diseases and identified as an independent risk factor.4,5 Several studies have shown that obese subjects have higher degrees of arterial stiffness.6,7 Previously, we have reported that both dietary modification and aerobic exercise training can independently decrease arterial stiffness with significant weight loss in obese individuals.8,10 It is well known that the combination of diet modification and aerobic exercise training is more effective than either modality alone.13 In the present study, we showed that the addition of WBV training to a 12-week lifestyle-modification program decreased arterial stiffness in premenopausal overweight and obese women. These findings suggest that a combination of dietary modification, habitual aerobic exercise, and WBV decreases arterial stiffness, which may have beneficial effects on the prevention of cardiovascular diseases in overweight and obese women.
Aging is associated with loss of muscle mass and strength because of decrease in physical activity levels.14,15 Obesity may further promote a loss of muscle mass with aging and lead to muscle weakness and/or insulin resistance.15 Elderly obese individuals are therefore more susceptible to physical disability.14 It is thus important to prevent a loss of muscle mass during weight loss in middle-aged obese individuals. Resistance training does not induce a fat-mass loss, but it can prevent loss of muscle mass and can also increase the resting metabolic rate.9 It has been demonstrated that the combination of dietary restriction with aerobic exercise training is insufficient to stop decreasing lean body mass.24 On the other hand, it has been shown that resistance training increases arterial stiffness.17,18 For weight loss in obese individuals, neither loss of muscle mass nor an increase in arterial stiffness is a necessary consequence. Recently, WBV training has been shown to be a novel method for muscular strength training. From young women to the elderly, WBV training produces a similar positive effect to resistance training on muscle strength.19,20 Comparing to a resistance training without the vibration, WBV training induced muscle activation, and which is effective to increase muscular mass and strength.19,20 It has already been reported that acute WBV exercise decreases arterial stiffness.21 However, the long-term effects of WBV on arterial stiffness have not been elucidated. In the present study, we showed that the addition of WBV training to a 12-week lifestyle-modification program lowers arterial stiffness, as assessed by PWV, in premenopausal overweight and obese women. At the present study, moreover, the percentage of lean body mass increased, which may also be the effect of WBV training. In previous study, it has been shown that WBV training induces hypertrophy in type I and II muscle fibers in rats.25 The present result could not demonstrate as the effect of WBV training, because we used WBV training combined with a 12-week lifestyle-modification program. However, we have already known that the combination of dietary restriction with aerobic exercise training is insufficient to stop decreasing lean body mass.24 Therefore, habitual WBV training may contribute to increase the percentage of lean body mass in overweight and obese women. Taken together, WBV training can be a novel strength-training methodology, which does not decrease muscular mass or increase arterial stiffness. We propose that WBV training be added to the classical lifestyle-modification programs for overweight and obese individuals, for avoiding decreases in muscle strength and concomitant increases in arterial stiffness.
The mechanisms underlying the decrease in arterial stiffness after lifestyle modification with WBV training are unclear. Elevation of plasma PTX3 concentration is thought to be the result of cardioprotective and atheroprotective effects.12,26 PTX3 adjusts both proinflammatory and anti-inflammatory factors, to limit excess activation of inflammation, which may result in the prevention of cardiovascular diseases.27 We found that plasma PTX3 concentrations increased in premenopausal overweight and obese women after the lifestyle-modification program incorporating WBV. We previously reported that plasma PTX3 concentrations are higher in endurance-trained men are higher than in sedentary controls in a cross-sectional study.12 The results of the present study, however, suggest that an increase in PTX3 concentration results not only from exercise training but also from weight loss in overweight and obese women. We found that the relationship between plasma PTX3 concentrations and BMI is linear, indicating that PTX3 is a surrogate index of the cardioprotective effects of weight loss in obese individuals. It is known that PTX3 is synthesized by several types of cells upon cytokine stimulation; the predominant types of cells are vascular endothelial cells, smooth muscle cells, and monocytes.27 Alberti et al.28 reported that adipose tissue is also synthesizes PTX3 and observed that PTX3 levels in visceral fat are positively correlated with BMI. In a cross-sectional study, Sutton-Tyrrell et al.29 reported that arterial stiffness is greater in obese individuals with the accumulation of abdominal visceral fat. The accumulation of visceral fat is a risk factor for cardiovascular morbidity and mortality. The cellular mechanisms linking obesity and arterial stiffness are complex and have not been fully elucidated. Our present study suggests that increasing PTX3 concentration is a key factor for lowering obesity-linked cardiovascular disease mortality.
The present study has several limitations. First, female estrogen hormone may strongly affect vascular constrictive adjustment. It has been reported that some methods of arterial stiffness evaluation can be affected by the menstrual cycle.30 However, PWV is one of the means of measuring arterial stiffness, independently of the effects of menstrual cycle.31 Our present study therefore appropriately evaluated the effects of this lifestyle-modification program on arterial stiffness. Second, the lifestyle-modification program in the present study comprised dietary modifications, habitual aerobic exercise, and WBV training. Therefore, we could not confirm the effects of WBV training alone. Third, we did not measure any index of muscle strength. Fourth, the present study investigated the effects of WBV training combined with a 12-week lifestyle-modification program in overweight and obese women. The present results may not generalize to other populations. Further studies will need to address these issues.
In conclusion, the present study revealed that after the 12-week lifestyle-modification program that included WBV, arterial stiffness decreased without reduction in the percentage of lean body mass in premenopausal overweight and obese women. However, the plasma PTX3 concentrations of these women increased. We thus propose addition of WBV training to the classical lifestyle modifications (dietary modification and aerobic exercise training) as the preferred weight-loss regimen for overweight and obese individuals. Additionally, the increase in plasma PTX3 concentrations may be associated with weight reduction in overweight and obese women. These results suggest that PTX3 participates in the mechanism underlying a decrease in arterial stiffness that is accompanied by weight reduction in overweight and obese individuals via this novel lifestyle-modification program with WBV.
Acknowledgements
This work was supported by Grants-in-Aid for Scientific Research 21300234 and 21650179 and Grant-in-Aid for JSPS Fellows 21692 from Japan Society for the Promotion of Science.
References
Cite this article
TY - JOUR AU - Asako Miyaki AU - Seiji Maeda AU - Youngju Choi AU - Nobuhiko Akazawa AU - Yoko Tanabe AU - Rina So AU - Kiyoji Tanaka AU - Ryuichi Ajisaka PY - 2012 DA - 2012/02/15 TI - The addition of whole-body vibration to a lifestyle modification on arterial stiffness in overweight and obese women JO - Artery Research SP - 85 EP - 91 VL - 6 IS - 2 SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2012.01.006 DO - 10.1016/j.artres.2012.01.006 ID - Miyaki2012 ER -