
Comparison of estimates of central systolic blood pressure and peripheral augmentation index obtained from the Omron HEM-9000AI and SphygmoCor systems
- DOI
- 10.1016/j.artres.2009.02.001How to use a DOI?
- Keywords
- Applanation tonometry; Central systolic pressure; Augmentation index
- Abstract
Central blood pressure is increasingly considered to be more predictive of cardiovascular events than peripheral pressure. Central systolic pressure (cSBP) can be estimated from the late systolic shoulder (pSBP2) of the radial pulse waveform. The Omron HEM-9000AI utilizes this technique to non-invasively measure cSBP through semi-automated applanation tonometry. The aim of this study was to compare the Omron HEM-9000AI with an existing device, the SphygmoCor, and to test its reproducibility.
33 subjects were tested using both the Omron and the SphygmoCor devices, which identify pSBP2 in the radial waveform, and estimate cSBP and peripheral augmentation index (pAIx) using their inbuilt software. 10 subjects were retested after a period of 24 h to determine reproducibility.
There was a strong correlation (r = 0.94; P < 0.001), and no difference between mean values of pSBP2 (0.8 ± 4.8 mmHg; P = 0.4) measured by the two devices. However estimates of cSBP were significantly higher in the Omron than the SphygmoCor (12.2 ± 4.6 mmHg; P < 0.001), despite significant correlation (r = 0.95; P < 0.001). pAIx measurements were correlated (r = 0.85; P < 0.001) with no significant difference between absolute values (mean difference = 1 ± 9.2%; P = 0.6). Results from both devices were reproducible, with significant correlation and insignificant mean differences for values of cSBP and pAIx.
pSBP2 values were highly correlated, but a direct analysis with invasive measurements is necessary to determine which estimate of cSBP is most accurate. Excluding this discrepancy, the Omron system is potentially useful for measuring pSBP2 and pAIx in large scale trials.
- Copyright
- © 2009 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
Central aortic blood pressure has recently received significant interest as a more accurate predictor of outcome than brachial artery blood pressure.1,2 Peripheral blood pressure is higher than central blood pressure due to pressure amplification from the aorta to the brachial artery.3,4 However there is considerable variation in central blood pressures even between individuals with similar brachial blood pressure.5 Moreover, pharmacological intervention produces a larger decrease in central pressure than peripheral pressure,6–8 and the administration of noradrenaline can induce opposite effects on central and peripheral pressure.9 Although central blood pressure cannot be reliably inferred from a cuff measurement of brachial systolic and diastolic blood pressure, a number of techniques exist to assess the aortic pressure. Aortic pressure can be measured directly by cardiac catheterisation. However, this method is invasive and, therefore, not appropriate for large scale trials. A commercially available device (SphygmoCor) records the radial pulse waveform using applanation tonometry, and then applies a transfer function to obtain the central aortic pressure waveform and a number of other indices, including central systolic blood pressure (cSBP). This estimated cSBP correlates strongly with data from direct invasive measurement of central blood pressure.4,10
Central systolic blood pressure can also be estimated from the late systolic shoulder of the radial pulse waveform (pSBP2), without the use of a transfer function. Close correlation between pSBP2 and cSBP has been demonstrated,6,7,11 with similar absolute values.6,11 A new device, the Omron HEM-9000AI utilizes this technique to estimate central systolic blood pressure with one important difference. pSBP2 is identified in the radial pressure waveform but a commercial algorithm is then applied to estimate the cSBP.7 The aim of this study was to compare the values of central systolic pressure and peripheral augmentation index calculated by the Omron and the SphygmoCor systems. The reproducibility for both devices was also investigated.
Methods
Subjects
In all, 33 healthy subjects (mean age 36 ± 12years, range 20–61 years), who were free from cardiovascular disease and medication were recruited from the Clinical Pharmacology Unit and an existing database of healthy volunteers. Local Research Ethics Committee approval was obtained and informed consent given by all subjects.
Devices
The two devices compared were the SphygmoCor (AtCor Medical, Sydney, Australia) and the Omron HEM-9000AI (Omron Healthcare Co., Ltd., Kyoto, Japan). The late systolic shoulder (pSBP2; Fig. 1) represents the influence of the reflected wave, and is provided by both systems’ software. The Omron system then estimates central systolic blood pressure (cSBPom) from the pSBP2 value, using linear regression. The SphygmoCor estimates central systolic pressure (cSBPsphyg) from the aortic pressure wave, which is derived from the radial pressure wave using a generalised transfer function. Both devices use inbuilt software to derive peripheral augmentation index (pAIx) from the radial pulse waveform, and the same equation is used by both.
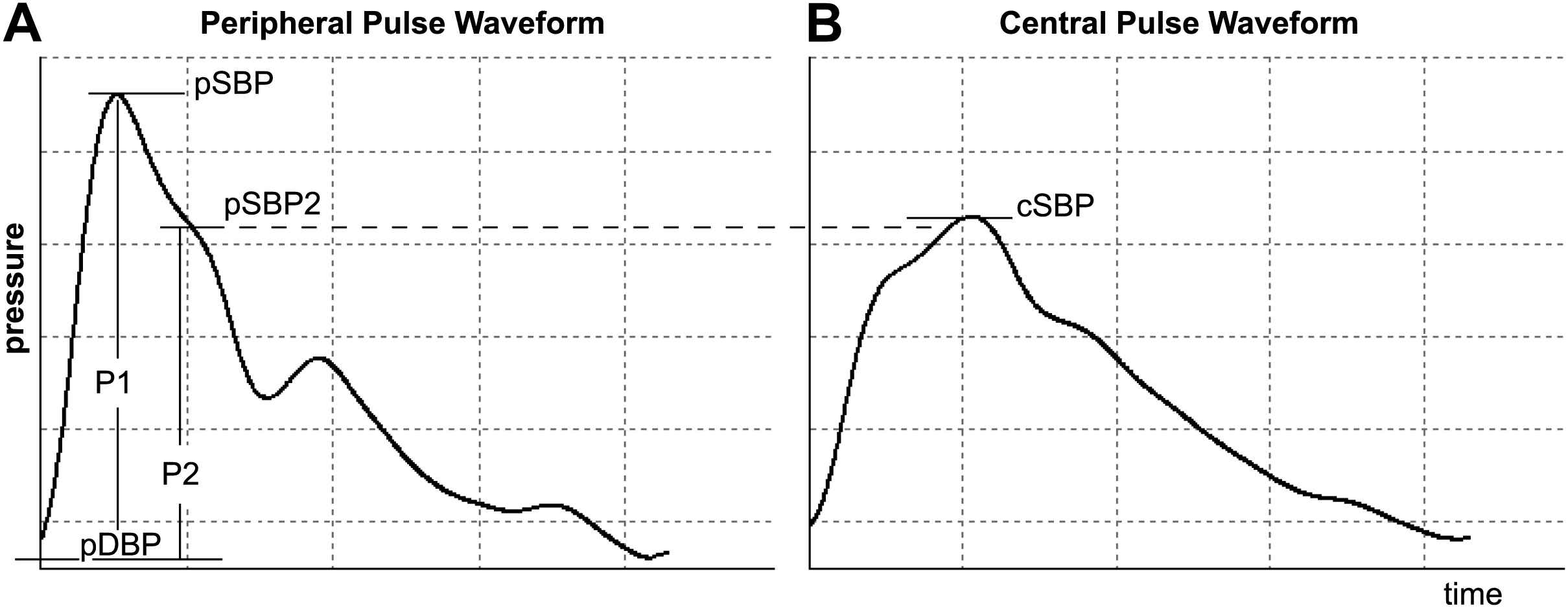
Relationship between peripheral pulse waveform and central pulse waveform. A, showing peripheral (radial) pulse waveform with peripheral systolic pressure (pSBP), peripheral late systolic shoulder (pSBP2) and definitions of P1 and P2 as used to calculate peripheral augmentation index (pAIx). B, showing central (aortic) waveform with central systolic blood pressure (cSBP), corresponding in amplitude to pSBP2.
Protocol
Applanation tonometry of the radial artery at the left wrist was performed in all subjects using both the Omron and the SphygmoCor systems. Subjects were rested for at least 5 min prior to measurement. The order of measurement was randomised, and measurements were performed immediately after each other. Brachial blood pressure was measured in the right arm using the Omron’s inbuilt oscillometric device according to BHS guidelines, and the average blood pressure measurements were used to scale both the Omron and the SphygmoCor readings. Measurements were repeated to achieve two blood pressure readings within 5 mmHg for the Omron system, and to achieve two high quality pulse wave readings with the SphygmoCor system. An average of two readings from each device was used in the subsequent analysis. All readings were made by one trained operator (CJR).
In one subject pSBP2 could not be identified from the radial pulse wave by the SphygmoCor and, therefore, pAIx could not be calculated. This reading was excluded from further analysis of pAIx, but included in comparisons of cSBP, which was successfully calculated.
Reproducibility
To assess reproducibility rather than repeatability, the readings in 10 subjects (mean age 34 ± 10 years; range 20–51 years) were repeated in the same order, 24 h later to minimize diurnal variation.
Data analysis
Pulse pressure (PP) amplification was calculated as the ratio between peripheral and central PP. Data were analysed using the method of Bland and Altman,12 to demonstrate the difference in values between the two devices. Pearson’s correlation coefficient (r) was used to determine correlation and paired Student’s t-tests used to assess significance of the difference between absolute values. Data are presented as means ± SD, and a P value <0.05 was considered significant.
Results
Measurement of central systolic blood pressure and peripheral augmentation index
Subject characteristics and seated brachial blood pressure values are shown in Table 1.
| Characteristic | Value |
|---|---|
| Age (years) (range) | 36 ± 12 (41) |
| Gender, male/female | 10/23 |
| Height (m) | 1.68 ± 0.09 |
| Weight (kg) | 67 ± 12 |
| BMI (kg/m2) | 23. 8 ± 3.3 |
| Systolic BP (mmHg) | 119 ± 13 |
| Diastolic BP (mmHg) | 71 ± 9 |
| Mean BP (mmHg) | 87 ± 10 |
| Pulse Pressure (mmHg) | 48 ± 8 |
| Heart Rate (bpm) | 65 ± 12 |
Data are means ± SD.
Subject characteristics.
The values of the late radial systolic shoulder (pSBP2) calculated by both devices (pSBP2sphyg and pSBP2om) showed strong correlation (r = 0.94; P < 0.001; Table 2; Fig. 2), with no significant difference between absolute values (mean difference 0.8 ± 4.8 mmHg; P = 0.4).
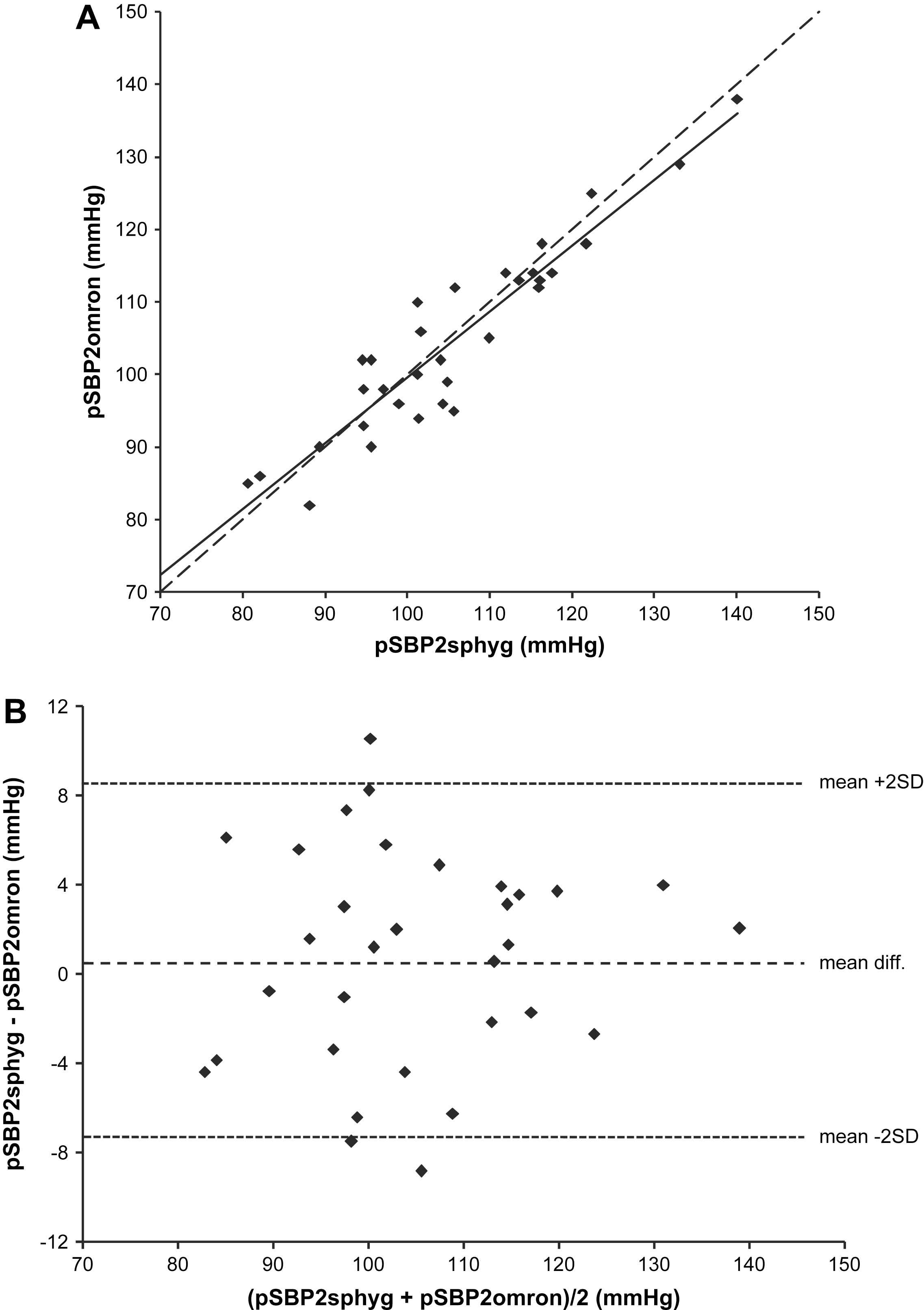
Correlation between peripheral late systolic shoulder amplitude calculated by the SyphgmoCor and the Omron. A, correlation between peripheral late systolic shoulder estimated by the SphygmoCor (pSBP2sphyg) and the Omron (pSBP2omron). Regression equation: Y = 0.907x + 8.952. Dashed line indicates line of identity. B, Bland–Altman plot showing agreement between pSBP2sphyg and pSBP2omron.
| SphygmoCor | Omron | Difference | P | Pearson’s r | P | |
|---|---|---|---|---|---|---|
| pSBP2 (mmHg) | 105.5 ± 13.5 | 104.6 ± 13.1 | 0.8 ± 4.8 | 0.36 | 0.94 | <0.001 |
| cSBP (mmHg) | 106.4 ± 11.5 | 118.5 ± 14 | −12.2 ± 4.6 | <0.001 | 0.95 | <0.001 |
| PP amplification | 1.37 ± 0.16 | 1.03 ± 0.17 | 0.34 ± 0.11 | <0.001 | 0.78 | <0.001 |
| pAIx (%) | 72.0 ± 17.4 | 71.0 ± 15.4 | 1.0 ± 9.2 | 0.59 | 0.85 | <0.001 |
| cSBPsphyg − pSBP2om difference | 1.8 ± 4.3 | 0.02 | 0.95 | <0.001 | ||
| cSBPsphyg − pSBP2sphyg difference | 1.0 ± 4.9 | 0.28 | 0.94 | <0.001 | ||
| cSBPom − pSBP2om difference | 13.9 ± 0.8 | <0.001 | 1.00 | <0.001 | ||
Data are means ± SD.
Values obtained from the two devices.
There was a close correlation between cSBPsphyg and cSBPom (r = 0.95; P < 0.001; Fig. 3). However, absolute values of cSBP measured by the two devices differed significantly (mean difference 12.2 ± 4.6 mmHg, P < 0.001), as did PP amplification (mean difference 0.34 ± 0.11, P < 0.001). A comparison between cSBPsphyg and pSBP2om values showed a smaller mean difference of 1.8 ± 4.3 mmHg (P = 0.02; Fig. 4), which remained significant. In addition, cSBPsphyg and pSBP2sphyg values were similar (mean difference 1.0 ± 4.9 mmHg, P = 0.28). However, the mean difference between cSBPom and pSBP2om was 13.9 ± 0.8 mmHg (P < 0.001) and the average cSBP measured by the Omron was 119 mmHg, which was equal to the average brachial systolic blood pressure (Table 1). Indeed, in 14 out of the 33 individuals studied, cSPB estimated using the Omron device exceeded the brachial SBP value.
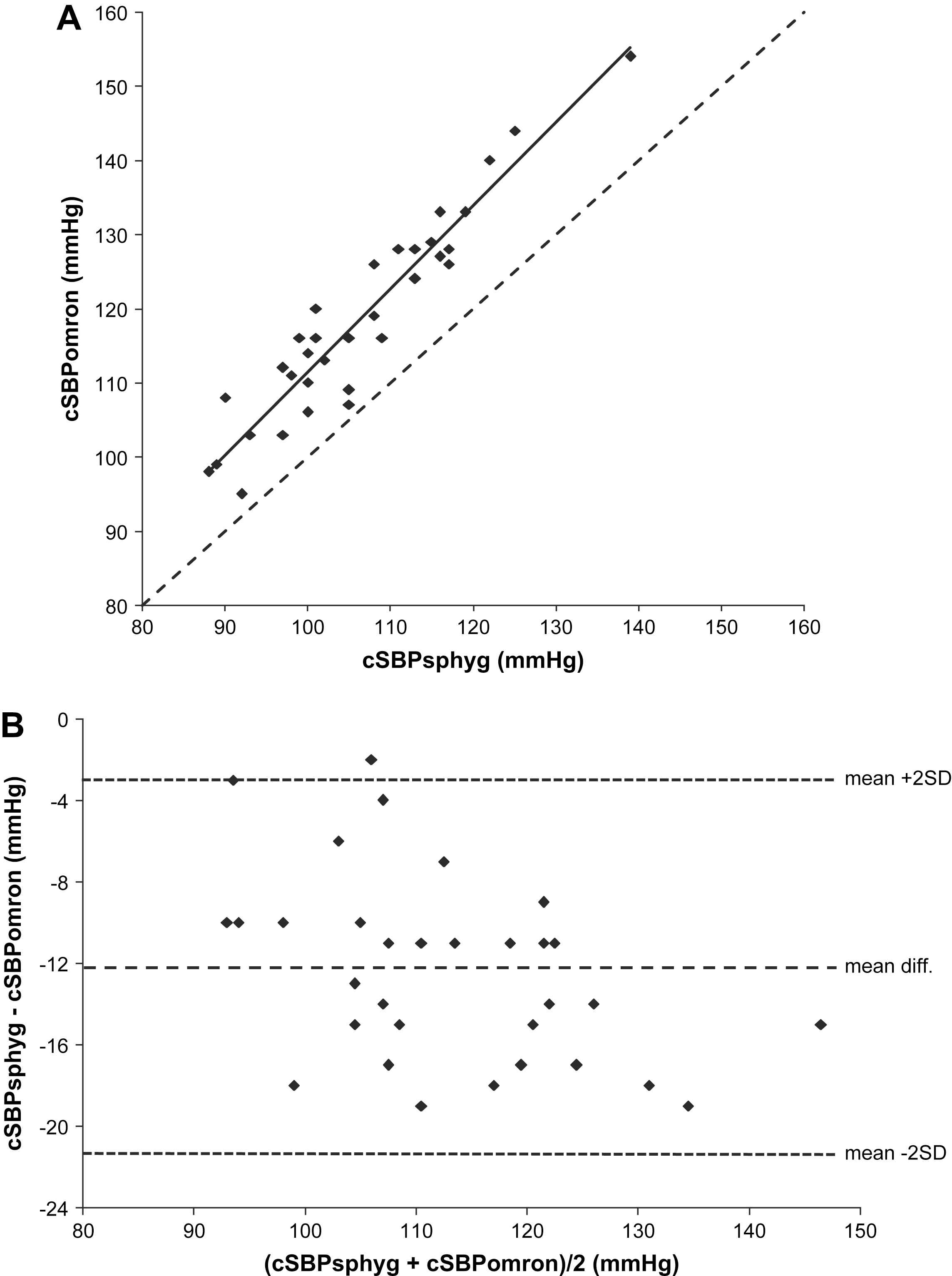
Correlation between central systolic blood pressure estimated by the SphygmoCor and the Omron. A, correlation between central systolic pressure estimated by the SphygmoCor (cSBPsphyg) and the Omron (cSBPomron). Regression equation: Y = 1.123x − 0.935. Dashed line indicates line of identity. B, Bland–Altman plot showing agreement between cSBPsphyg and cSBPomron.
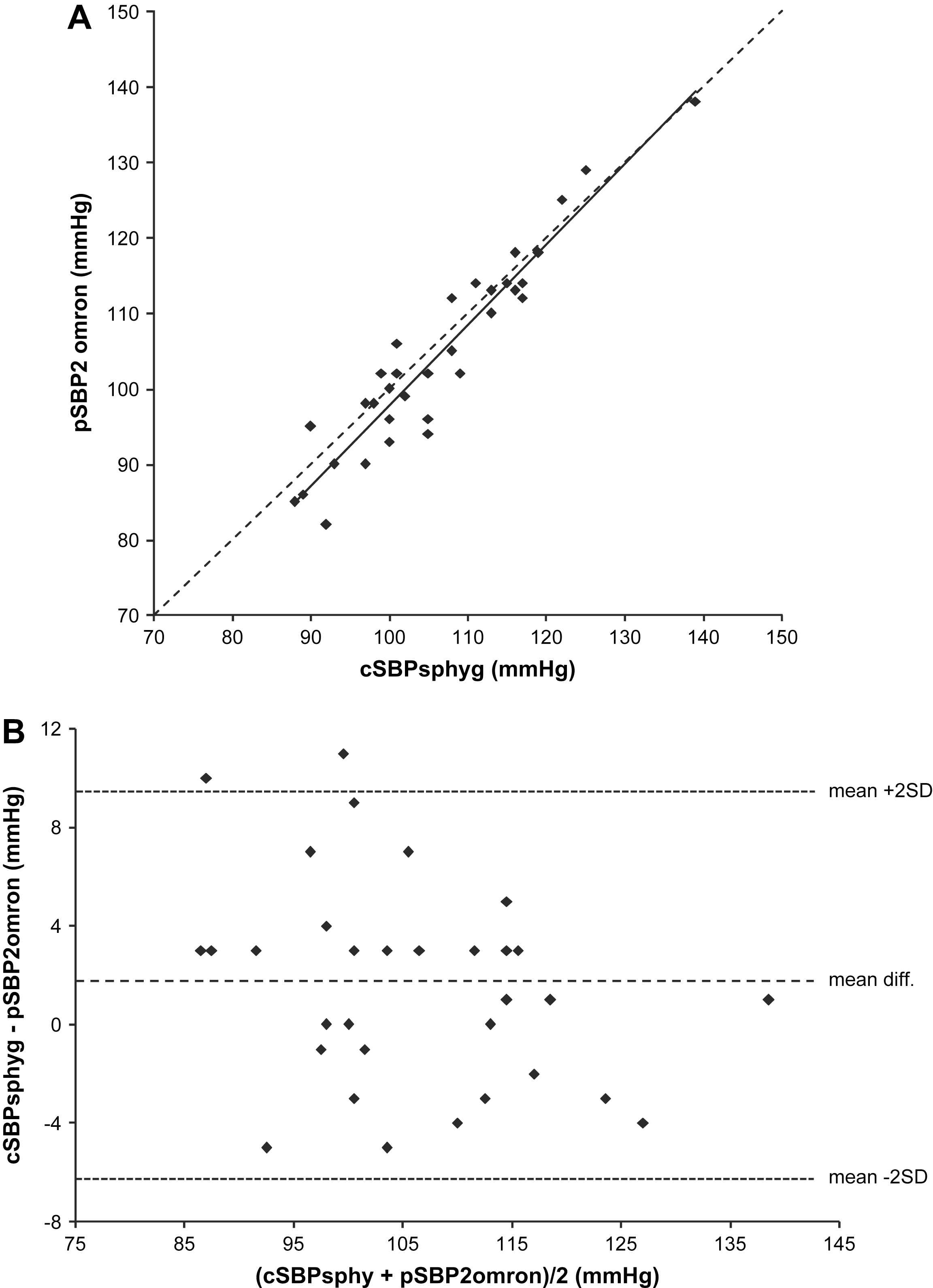
Correlation between central systolic blood pressure calculated by the SphygmoCor and the peripheral late systolic shoulder identified by the Omron. A, correlation between pSBP2omron and cSBPsphyg. Regression equation: Y = 1.065x − 8.731. Dashed line indicates line of identity. B, Bland–Altman plot showing agreement between pSBP2omron and cSBPsphyg.
Peripheral augmentation index measured by both devices showed close correlation (r = 0.85; P < 0.001; Fig. 5) and a mean difference of 0.1 ± 9.2%, which was not significant (P = 0.6).
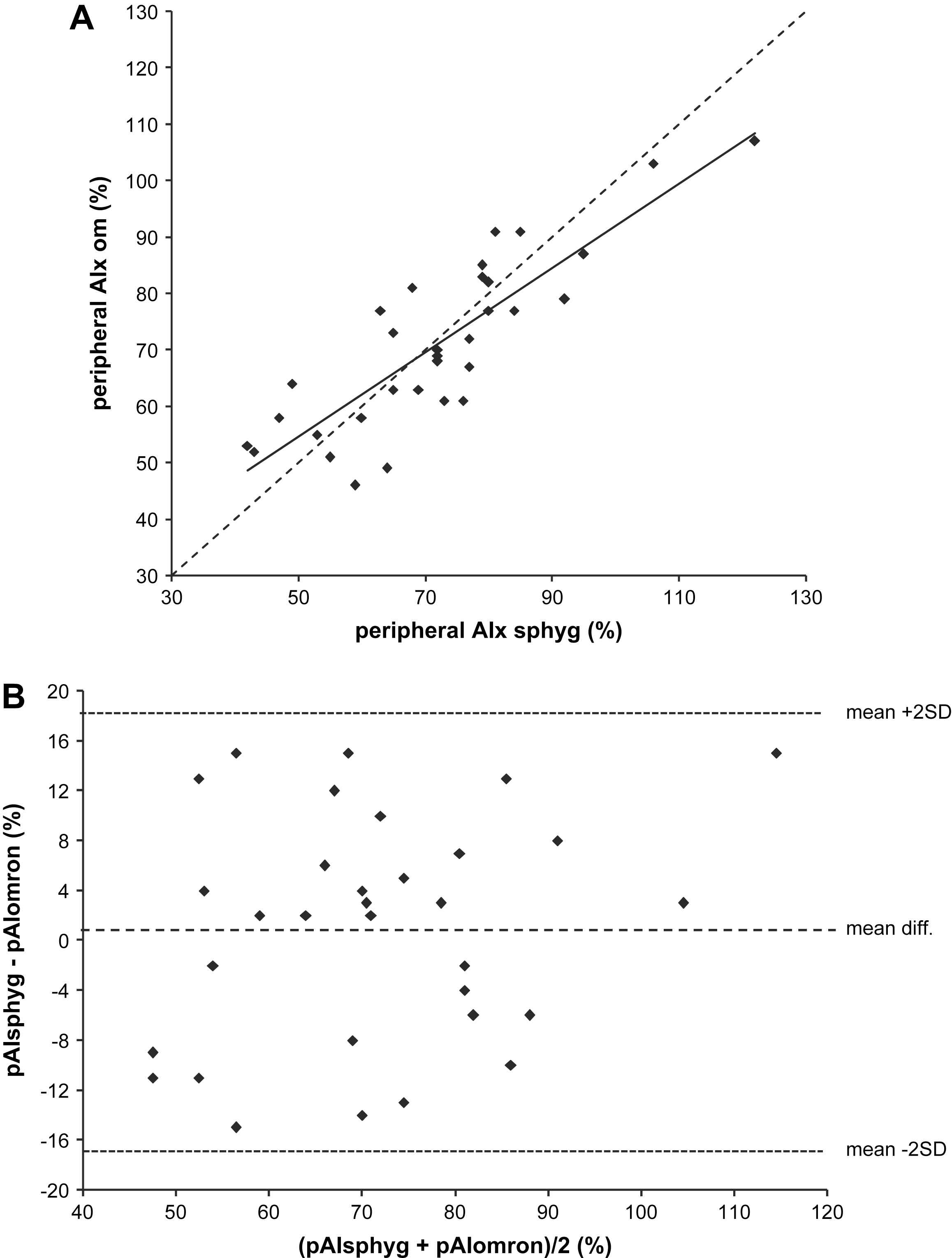
Correlation between peripheral augmentation index calculated by the SphygmoCor and the Omron. A, correlation between peripheral augmentation index calculated by the SphygmoCor (pAIxsphyg) and the Omron (pAIxomron). Regression equation: Y = 0.748x + 17.16. Dashed line indicates line of identity. B, Bland–Altman plot showing agreement between pAIxomron and pAIxsphyg.
Reproducibility
Repeated measurements of cSBP and pAIx after 24 h showed significant correlation and agreement with the original values from both the SphygmoCor and the Omron devices (Table 3). Correlation between measurements of cSBP was higher with the SphygmoCor system (mean difference = 3.0 ± 5.4 mmHg; P = 0.11; r = 0.83; P < 0.01) than the Omron (mean difference = 6.2 ± 9.1 mmHg; P = 0.06; r = 0.76; P < 0.05). Peripheral AIx readings with the SphygmoCor showed a mean difference of −1.3 ± 8.6% (P = 0.6) and a correlation of r = 0.88 (P < 0.001) whereas the Omron readings had a larger mean difference but a slightly smaller standard deviation (3.7 ± 7.4%; P = 0.15), and a similar correlation (r = 0.90, P < 0.001).
| 1st reading | 2nd reading | Difference | P | Pearson Correlation | P | |
|---|---|---|---|---|---|---|
| cSBPsphyg (mmHg) | 105.4 ± 9.0 | 102.4 ± 9.2 | 3.0 ± 5.4 | 0.11 | 0.83 | <0.01 |
| cSBPom (mmHg) | 117.8 ± 10.0 | 111.6 ± 14.0 | 6.2 ± 9.1 | 0.06 | 0.76 | <0.05 |
| pAIxsphyg (%) | 68.4 ± 15.1 | 69.7 ± 18.1 | −1.3 ± 8.6 | 0.64 | 0.88 | <0.001 |
| pAIxom (%) | 70.8 ± 14.2 | 67.1 ± 17.1 | 3.7 ± 7.4 | 0.15 | 0.90 | <0.001 |
Data are means ± SD.
Reproducibility.
Discussion
As several papers have recently reported, aortic systolic blood pressure holds important predictive value for calculating future cardiovascular events, independently of brachial pressure.2 McEniery et al.5 demonstrated that for a given level of brachial systolic pressure, aortic systolic pressure was higher in those individuals with cardiovascular risk factors or disease compared with healthy subjects. If measurement of central pressure is to become routine, it is important to be able to perform measurements quickly and non-invasively in large populations. The Omron HEM-9000AI is semi-automated, and performs applanation tonometry through an array of sensors applied to the radial pulse in the wrist. This measures the radial pulse waveform and calculates cSBP and pAIx. The device is potentially suitable for estimating cSBP in large populations as it is quick and easy to use, and relatively operator independent. However, the findings of the current study suggest that the late systolic shoulder of the radial pressure wave (pSBP2) may provide a better estimate of aortic systolic pressure than the estimated cSBP value provided by the Omron device.
Use of pSBP2 as a direct estimate of aortic systolic pressure has been validated against invasive measurements.6,7,11 The mean difference between pSBP2 and aortic systolic pressure was 1.8 ± 4 mmHg in the study by Munir et al.,6 and 1 ± 2 mmHg in the study by Pauca et al.11 However, using the Omron device, Takazawa et al.7 observed that although pSBP2 and aortic systolic pressure were highly correlated, the mean difference between them was 11.7 ± 7.1 mmHg. The Omron system extrapolates the pSBP2 to provide an estimate of cSBP, using linear regression. When comparing the values of the late systolic shoulder of the radial pulse wave identified by both devices (pSBP2sphyg and pSBP2om), the mean difference between devices was not significant. However the standard deviation of 5 mmHg means that individual data pairs may lie as much as 10 mmHg apart. This may be due to inaccuracies in detecting the late systolic inflection on the radial pulse wave in some subjects, which represents a potential limitation of this approach.
Estimates of cSBP calculated by the Omron and the SphygmoCor devices were highly correlated. However, absolute values calculated by the Omron were on average 12.2 mmHg higher than the SphygmoCor. Moreover, the Omron system’s estimates of cSBP were on average 13.9 mmHg higher than the corresponding pSBP2om value, a result of the conversion factor used to estimate cSBP from pSBP2. When comparing the original pSBP2om values with the cSBP calculated by SphygmoCor, the mean difference was only 1.8 mmHg. As we did not make invasive measurements of aortic pressure, it is impossible to know whether cSBPom or cSBPsphyg is closer to the true aortic SBP. However, the SphygmoCor’s system of estimating cSBP has been validated against invasive measurements,4,10 and it is therefore likely to be reliable. Moreover, using the Omron device, the mean difference between brachial SBP and cSBP was only 0.8 ± 8 mmHg, and central-to-peripheral PP amplification was negligible. Clearly this is not correct as peripheral pressure amplification increases brachial pressure values above those in the aorta, as has been confirmed by invasive data.3,4 Indeed, in nearly half of the subjects in the current study, the cSBP calculated by the Omron device was actually higher than the value of brachial blood pressure, which is non-physiological.
These data suggest that in estimating cSBP, the Omron’s inbuilt conversion factor over-compensates for differences between pSBP2 and actual aortic SBP. As pSBP2om is significantly closer to cSBPsphyg than the estimation of cSBPom, use of the conversion factor to obtain cSBPom seems unnecessary. Moreover, the cSBP value provided by the Omron device appears to be inaccurate, given the non-physiological values of PP amplification. Further comparison with direct invasive measurements of aortic pressure may yield a more appropriate algorithm to convert pSBP2om to cSBPom. Nevertheless, we suggest that to estimate central pressure accurately using the Omron device, investigators should use pSBP2 rather than the estimated value of cSBP.
Peripheral augmentation index is calculated by the same formula in both devices. As would be expected from the good correlation between pSBP2 values, there was strong agreement between the values of pAIx calculated by each device. The Omron therefore provides a reliable measure of peripheral augmentation index. The reproducibility for pAIx was higher than for cSBP with both devices. This is likely to be due to the natural variations in brachial blood pressure, whereas pAIx is a fiducial parameter and, unlike cSBP, is independent of scaling issues. The reproducibility with the Omron device was lower than that of the SphygmoCor system for cSBP, and pAIx readings in the Omron had a larger mean difference. This may be due to the SphygmoCor providing quality control data which allow the operator to select the best possible reading, thus minimising artefacts and improving quality. Despite this, both devices showed significant correlation and insignificant mean difference between the two readings, proving them both to provide reproducible results.
In summary, pSBP2 and estimated cSBP provided by the Omron system correlate strongly with values obtained from the SphygmoCor system. In addition, absolute values of pSBP2 obtained with each device were similar. However, absolute values of cSBP differed significantly between the devices. It is unclear from the current study whether values of pSBP2 or estimated cSBP are closer to the true value of aortic pressure, and further investigations comparing estimates of cSBP by the Omron HEM-9000AI to direct measurements of aortic pressure by cardiac catheterisation are recommended. Nevertheless, the results suggest that the Omron HEM-9000AI has potential for use in large scale trials, giving accurate, reproducible measurements of pSBP2 and pAIx, which show strong correlations with those of the SphygmoCor device.
References
Cite this article
TY - JOUR AU - Charlotte J. Richardson AU - Kaisa M. Maki-Petaja AU - Barry J. McDonnell AU - Stacey S. Hickson AU - Ian B. Wilkinson AU - Carmel M. McEniery PY - 2009 DA - 2009/02/28 TI - Comparison of estimates of central systolic blood pressure and peripheral augmentation index obtained from the Omron HEM-9000AI and SphygmoCor systems JO - Artery Research SP - 24 EP - 31 VL - 3 IS - 1 SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2009.02.001 DO - 10.1016/j.artres.2009.02.001 ID - Richardson2009 ER -