
Magnitude and Reasons for Gaps in Tuberculosis Diagnostic Testing and Treatment Initiation: An Operational Research Study from Dakshina Kannada, South India
 , Akshaya Kibballi Madhukeshwar1, Poonam Ramesh Naik1, Badarudeen Mohammad Nayarmoole2, Srinath Satyanarayana3, 4
, Akshaya Kibballi Madhukeshwar1, Poonam Ramesh Naik1, Badarudeen Mohammad Nayarmoole2, Srinath Satyanarayana3, 4- DOI
- 10.2991/jegh.k.200516.001How to use a DOI?
- Keywords
- Tuberculosis; diagnosis; treatment; attrition; Nikshay; qualitative; SORT IT
- Abstract
Background: In India, ensuring all Persons with Presumptive TB (PPTB) undergo TB diagnostic tests and initiating all diagnosed TB patients on treatment are two major implementation challenges.
Objectives: In a coastal district of Karnataka state, South India, to (1) determine the number and proportion of PPTB who did not undergo any TB diagnostic test, and the number and proportion of TB patients who were not initiated on treatment (2) explore the facilitators and barriers in TB diagnostic testing and treatment initiation from health care providers’ perspective.
Methods: For objective-1, we used a cross-sectional design involving review of data of PPTB enrolled for care during January–March 2019 and for objective-2, we used a qualitative design involving key informant interviews of health care providers.
Results: Of 8822 PPTB patients enrolled for evaluation of TB, 767 (9%) had not undergone any TB diagnostic test. In those who had undergone any TB diagnostic test, a total of 822 were diagnosed with TB and of them, 26 (3%) were not initiated on treatment. Cartridge-based nucleic acid amplification tests was used as a diagnostic test only among 1188 (13.5%) PPTB patients. The gaps in diagnostic testing were due to: non-availability of doctors/lab-technicians, inadequate knowledge about TB diagnostic tests among health care providers, reluctance of patients to undergo the TB diagnostic tests due to stigma/confidentiality issues and sub-optimal engagement of private health facilities for TB control.
Conclusion: About 9% of PPTB not undergoing any test for TB and 3% of the TB patients not initiated on treatment are of major concern. Revised National TB Control Programme needs to address the identified barriers to improve the process of TB diagnosis and treatment initiation.
- Copyright
- © 2020 The Authors. Published by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
India has the highest Tuberculosis (TB) burden in the world with an estimated incidence of 2.7 million cases [1]. It is also estimated that TB kills approximately 480,000 Indians every year, which amounts to 1400 deaths every day [2]. To reduce the burden of TB in the country, Government of India has been implementing Revised National TB Control Programme (RNTCP). In 2017, RNTCP launched the National Strategic Plan (NSP) Phase-2 to eliminate TB in India by the year 2025 in line with the World Health Organisation’s global plan to end TB by 2030 [2].
Early diagnosis and treatment is essential for TB control. In India and other high TB burden countries, loss of patients during and after TB diagnosis prior to TB treatment initiation (also called as pre-diagnosis and pre-treatment attrition respectively) are major challenges [3–6]. In India, within the public health system, facilities for TB diagnosis and treatment are not available in all the health facilities, and therefore, patients’ and their information have to flow between health facilities to ensure that all persons identified with TB symptoms undergo diagnostic evaluation and are initiated on TB treatment. A systematic review on the TB care cascade in India indicates that ~40% of patients seeking care from the public health facilities are lost during the process of TB diagnosis and treatment initiation [7].
Previous studies have indicated that several patients and health system factors are responsible for pre-diagnostic and pre-treatment attrition [8–13]. Many of the health system factors relate to gaps in the information flow between various health facilities about patients, their movement and management. Identifying and ameliorating the gaps in the patient information flow is one of the key thrust areas of RNTCP under the NSP.
In September 2018, RNTCP launched version 2 of Nikshay (Nikshay-2), a web-based TB recording and reporting system. Nikshay-2 makes it possible to track every person with presumptive TB through diagnosis, treatment initiation and up to TB treatment outcome [14]. Nikshay-2 intended to mitigate the gaps in the information flow by making it fully electronic and readily available at various levels of the health system. Following the implementation of Nikshay-2, there have not been any studies to assess whether the introduction of Nikshay-2 has resulted in improvement in the number and proportion of patients who complete the TB diagnosis care cascade.
Dakshina Kannada is a district in the south Indian state of Karnataka. In this district, as per the RNTCP reports prior to the roll out of Nikshay-2, the pre-treatment attrition was about 12.4% and there was no information on pre-diagnosis attrition in the first quarter of 2017 [15].
We, therefore, undertook an operational research study with the following two objectives: First, among the presumptive TB patients enrolled into Nikshay-2 from Dakshina Kannada between January 1st 2019 and March 31st 2019, to determine the number and proportion of persons with presumptive TB who did not undergo any test for TB diagnosis, and the number and proportion of diagnosed TB patients who were not initiated on treatment; Second, to explore the reasons for not undergoing diagnostic testing and TB patients not being initiated on treatment from the health care providers perspective.
2. MATERIALS AND METHODS
2.1. Study Design
For the first objective we used a cross-sectional study involving review of existing data in Nikshay-2 and for the second objective we used a qualitative design involving key informant interviews with health care providers.
2.2. Study Setting
Dakshina Kannada (DK) district is a coastal district of Karnataka state in South India and has a geographical area of 4861 km2 and a population of 20,89,649 with a population density of 430 persons/km2 according to 2011 India census [16]. About 48% of the population of the district lives in urban areas. Mangaluru is the headquarters of Dakshina Kannada district.
The District Tuberculosis Centre (DTC), Mangaluru which is the nodal point for TB control activities of Dakshina Kannada district functions through a network of nine Tuberculosis Units (TUs). These TUs situated at the sub-district level, have one Medical Officer - Tuberculosis Control (MO-TC) and two full time supervisory staff - Senior Treatment Supervisor (STS) and Senior Treatment Lab Supervisor (STLS) for implementing the TB control activities. Each TU has a network of Designated Microscopy Centres (DMCs) and Peripheral Health Institutions (PHIs) for carrying out the diagnostic, treatment and preventive activities under RNTCP. Under the public–private partnership model, RNTCP has set up a DMC at every private medical college with a medical officer, laboratory technician and health visitor. From January 2019 onward, all the primary health centers have started performing sputum smear microscopy. Currently, there are 96 DMCs in the district.
2.3. Nikshay Version 2.0
Nikshay version 2.0 is a web-based recording and reporting system for TB patient management in India. It is an updated version of an earlier Nikshay-1 and has been introduced in September 2018. This version includes unified interface for public and private health providers, integration of data on treatment adherence technologies, unified Drug Sensitive TB (DSTB) and Drug Resistant (DRTB) data entry forms. PHI level users can access and update the data through either website or mobile phone application. The demographic and clinical details of all persons with presumptive TB (including diagnostic tests, diagnosis of TB and treatment) are entered into Nikshay-2. A seven-digit unique patient ID gets generated on enrolment of the patients. This facilitates movement and tracking of patients through a referral and feedback mechanism and sharing of their information across various diagnostic and treatment facilities. All persons with TB symptoms are expected to undergo diagnostic tests [such as sputum smear, chest radiography, Cartridge-based Nucleic Acid Amplification Tests (CB-NAAT), culture and drug susceptibility tests] as per the RNTCP algorithm and those diagnosed with TB are expected to be initiated on TB treatment as per the RNTCP TB treatment guidelines [17]. These guidelines are in accordance with the WHO’s standard TB treatment guidelines.
2.4. Study Population
For the first objective, the study population included all the presumptive TB cases and TB cases enrolled in the Nikshay-2 portal in Dakshina Kannada district from 1st January 2019 to 31st March 2019.
For the second objective, health care providers involved in implementation of RNTCP [Medical Officer at PHIs, STS, STLS, health care staff involved in entering the patient data on Nikshay-2 portal such as TB Health Visitor (TBHV), Laboratory Technician (LT), pharmacist, staff nurse, lower division clerk, health workers at PHI and public–private mix coordinator] constituted the study population. Using purposive sampling method, health care providers from one urban and two rural TUs of Dakshina Kannada were selected to ensure representation from both urban and rural areas.
2.5. Data Variables, Sources of Data and Data Collection
For the first objective, data was obtained from the Nikshay-2 portal during June and August 2019. The following individual patient data were extracted from the Nikshay-2 portal: patient’s age, gender, enrolment facility, date of enrolment, date of sputum smear microscopy, results of sputum smear microscopy, name of DMC, date of CB-NAAT testing, CB-NAAT results, dates of radiography and results, date of diagnosis of TB, date and place of treatment initiation, type and site of TB. TB treatment initiation refers to a TB positive person being started on treatment.
For the second objective, data was collected during the months of June, July and August 2019. We conducted one-to-one Key Informant Interviews (KIIs) with a sample of health care providers (MO, STS, STLS, TBHV, LT, pharmacist, staff nurse, health worker and public–private coordinator). The Principal Investigator (PI) conducted the interviews. Interviews were done in the local language (Kannada) at the date, time and place convenient to participants. PI is a faculty member in a medical college and trained in the use of qualitative research methods. Participants were informed about the purpose of the study; the PI conducted one-to-one interviews after obtaining their permission and consent to participate in the study. Only the participant and the researcher were present during the interview. The PI also obtained consent from the participants for audio recording. To ensure participant validation, the summary of the interviews was read back to the participants before completing the interview. Field notes were made from the observations during data collection.
2.6. Analysis and Statistics
For the first objective, data from the Nikshay-2 portal was obtained as MS Excel File. The data were imported into the statistical software - SPSS (version 23.0 IBM, NY, USA) and STATA (version 15, Stata Corporation, College Station, TX, USA) and analyzed. The patient data on various variables has been summarized using numbers and proportions. The duration (in days) between TB diagnosis and treatment initiation in TB patients has been described using median and interquartile range. We quantified two key parameters: (a) Presumptive TB who had not undergone any one test for TB and (b) Presumptive TB not initiated on TB treatment after being diagnosed with TB. We took a cut-off date of 31st July 2019 to assess these two attritions.
We have used multivariable log binomial models to assess the association between demographic and clinical characteristics in persons who had not undergone any diagnostic test among presumptive TB patients and TB patients who were not initiated on TB treatment. The associations are reported as risk ratios and adjusted risk ratios along with the confidence intervals. A p-value <0.05 is taken as statistically significant.
We did not exclude patients with missing data as the data were not missing at random. In operational research, we believe that excluding patients with missing data will result in excluding patients who may have experienced/received sub-optimal care. Hence, we created a separate category for missing data within each variable and used that variable for analysis.
For the second objective, the PI generated transcripts either on the same day or within 48 h, whichever was earlier, based on the notes and audio records of the KIIs. Inductive approach was used and manual descriptive content analysis was done to identify the codes and themes [18,19]. These were reviewed by the co-investigators (AKM and SS) to reduce bias, increase inter-coder reliability and enhance interpretative credibility. The decision on coding rules and theme generation were done by using standard procedures and based on consensus. Differences if any were resolved by discussion. Coding of qualitative data was done. Similar codes were combined into themes. To ensure that the results are a reflection of the data, the codes/themes were related back to the original data. The findings are reported by using ‘Consolidated Criteria for Reporting Qualitative Research’ [20].
2.7. Ethics and Consent
Ethics approval was obtained from the Institutional Ethics Committee of Yenepoya Medical College, Yenepoya (Deemed to be University), Mangaluru (No 2019/019 dated 18th March 2019) and the Ethics Advisory Group of the International Union against Tuberculosis and Lung Disease, Paris, France (No 131/18 dated 18th January 2019). Permission was obtained from the State TB office for conducting the study. Written informed consent was obtained from health care providers for KIIs.
3. RESULTS
A total of 8822 presumptive TB patients were enrolled into Nikshay-2 from Dakshina Kannada District between 1st January and 31st March 2019. This included both pulmonary and extra-pulmonary presumptive TB patients. Of these, 8674 (98%) were enrolled from public health facilities (including DMCs from medical college hospitals) and 148 (2%) were enrolled from the private sector which included private hospitals and clinics. The mean (SD) age of the presumptive TB patients was 47.5 (18.1) years. About 4868 (55%) of the patients were males and 8221 (93%) of the patients were enrolled from PHIs. The proportion of key populations such as patients with diabetes, tobacco users, migrants, health workers, urban residents and Human Immunodeficiency Virus (HIV) seropositive has been presented in Table 1.
| Variables | Total | |
|---|---|---|
| N = 8822 (100) | n (%) | |
| Age (years) | ||
| <15 | 404 (4.6) | |
| 15–24 | 683 (7.7) | |
| 25–34 | 1073 (12.2) | |
| 35–44 | 1323 (15) | |
| 45–54 | 1801 (20.4) | |
| 55–64 | 1740 (19.7) | |
| ≥65 | 1792 (20.3) | |
| Unknown | 6 (0.1) | |
| Gender | ||
| Male | 4868 (55.2) | |
| Female | 3944 (44.7) | |
| Transgender | 10 (0.1) | |
| Enrollment Center | ||
| District | 145 (1.6) | |
| Peripheral health institute | 8221 (93.2) | |
| Private chemist | 9 (0.1) | |
| Private health facility | 167 (1.9) | |
| Private lab | 17 (0.2) | |
| Tuberculosis unit | 248 (2.8) | |
| Unknown | 15 (0.2) | |
| Contact of TB case | ||
| Yes | 141 (1.6) | |
| No | 8681 (98.4) | |
| Diabetes mellitus | ||
| Yes | 241 (2.7) | |
| No | 8566 (97.1) | |
| Unknown | 15 (0.2) | |
| Tobacco intake | ||
| Yes | 344 (3.9) | |
| No | 8478 (96.1) | |
| Migrant | ||
| Yes | 20 (0.2) | |
| No | 8802 (99.8) | |
| Health worker | ||
| Yes | 17 (0.2) | |
| No | 8805 (99.8) | |
| Urban slum resident | ||
| Yes | 7 (0.1) | |
| No | 8815 (99.9) | |
| HIV status | ||
| Positive | 107 (1.2) | |
| Negative | 4195 (47.6) | |
| Unknown | 4520 (51.2) | |
Demographic and clinical characteristics of presumptive TB patients enrolled into Nikshay from Dakshina Kannada, India, January–March 2019 (N = 8822)
Out of the total 8822 presumptive TB patients, 6839 (77.5%) underwent sputum microscopy for acid fast bacilli, 1188 (13.5%) underwent CB-NAAT by Xpert and 245 (2.8%) underwent other tests such as culture and line probe assay (Figure 1). Among the presumptive cases, 1025 (11.6%) patients had not undergone any microbiological testing such as sputum microscopy for acid fast bacilli, CB-NAAT or line probe assay and 767 (8.7%) had not undergone any TB test (Figure 2).
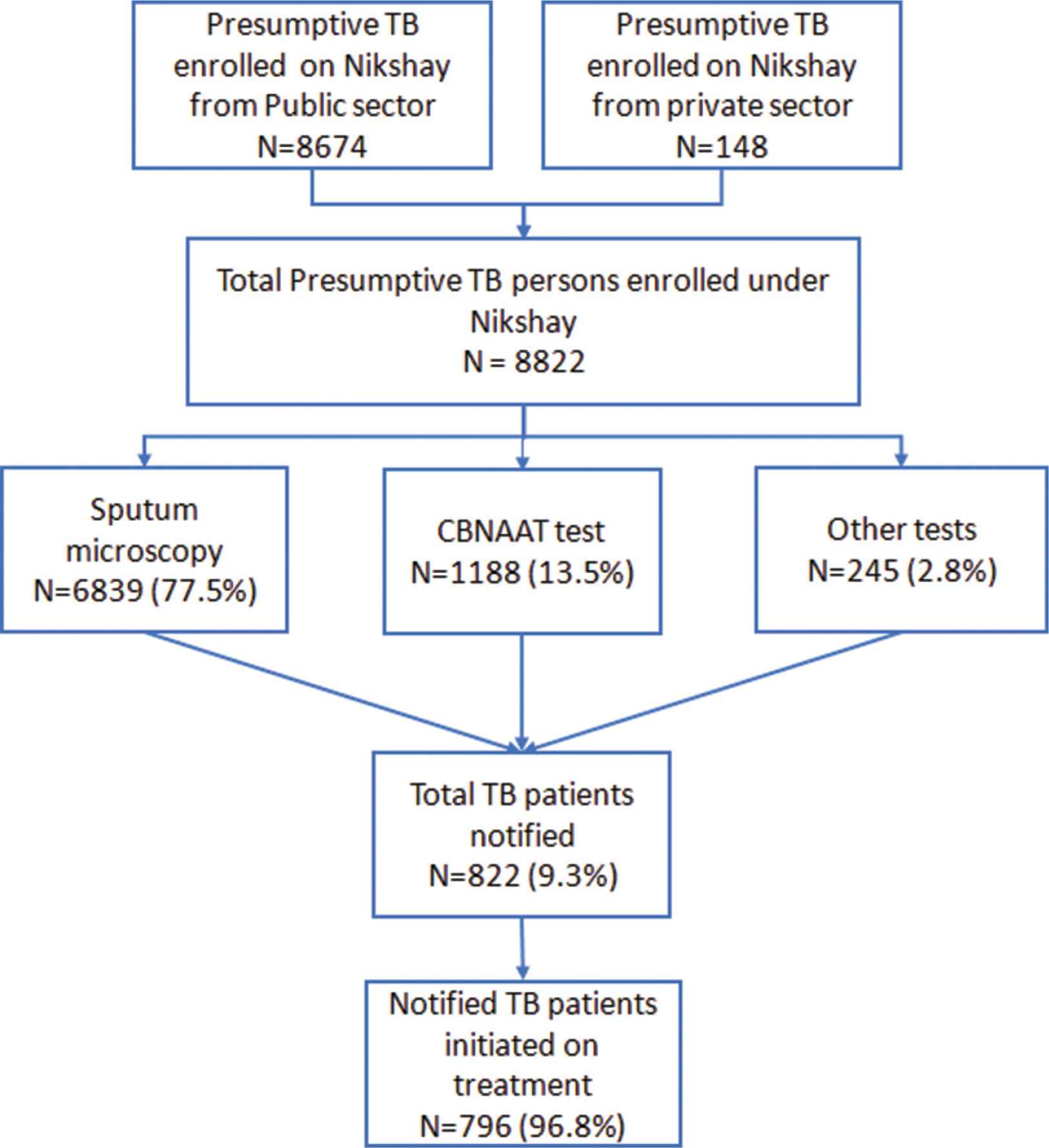
Documentation of the presumptive TB patients enrolled under Nikshay and TB patients notified in Dakshina Kannada, India, January–March, 2019 (N = 8822). Other test, culture and line probe assay.
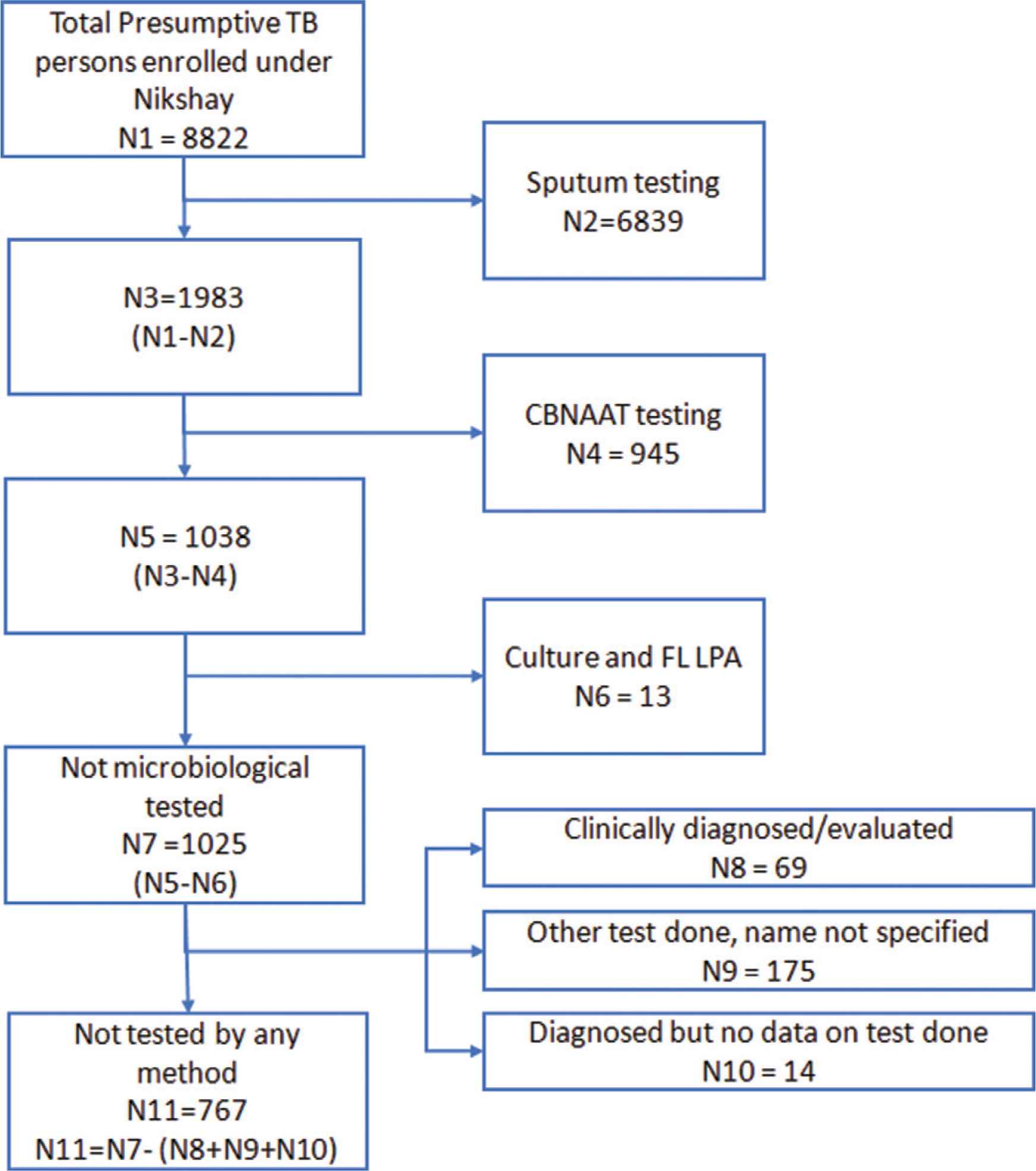
Flow diagram of the presumptive TB patients enrolled under Nikshay who have not undergone any microbiological test/diagnostic test in Dakshina Kannada, India, January–March, 2019 (N = 8822). FL LPA, First line - line probe assay; Not microbiological tested, not undergone sputum smear microscopy, cartridge-based nucleic acid amplification tests, culture and drug susceptibility tests for Mycobacterium tuberculosis.
Among the study cohort of 8822 presumptive TB patients, 822 were diagnosed with TB and of them, 796 (96.8%) were initiated on treatment. Among the 822 diagnosed TB cases, the basis of diagnosis was sputum microscopy in 296 (36.0%), CB-NAAT in 192 (23.3%), culture and line probe assay in 229 (27.9%) and clinical diagnosis in 105 (12.8%). The 796 TB patients who were initiated on treatment were largely by Government (89.2%) and rest by private (10.8%). The median time duration between TB diagnosis and treatment initiation was 1 day (interquartile range 0–3 days).
We assessed for the association between various demographic and clinical factors with presumptive cases not undergoing any test. In bivariable analysis, patients who were enrolled from private health facility, district TB centre, tuberculosis unit, those with unknown HIV status, those without contact with a TB case and those who did not have diabetes had higher probability of not undergoing any TB test (Table 2). However, on multivariable analysis enrolment in private health facility, tuberculosis unit and unknown HIV status were the only factors that were independently associated with a presumptive patient not undergoing any diagnostic test. We also assessed the association between various demographic and clinical factors with presumptive cases not undergoing any microbiological test (Supplementary Table 1).
| Variables | Total | Not undergone any TB test* | RR (95% CI) | aRR (95% CI) | p-value |
|---|---|---|---|---|---|
| N | n (%) | ||||
| 8822 | 767 (8.7) | ||||
| Age (years) | |||||
| <15 | 404 | 42 (10.4) | 1.19 (0.85–1.67) | 1.07 (0.77–1.50) | 0.660 |
| 15–24 | 683 | 56 (8.2) | 0.94 (0.69–1.28) | 0.93 (0.69–1.25) | 0.651 |
| 25–34 | 1073 | 110 (10.3) | 1.17 (0.91–1.51) | 1.16 (0.91–1.48) | 0.211 |
| 35–44 | 1323 | 115 (8.7) | Ref | ||
| 45–54 | 1801 | 153 (8.5) | 0.97 (0.77–1.23) | 1 (0.80–1.26) | 0.951 |
| 55–64 | 1740 | 147 (8.4) | 0.97 (0.76–1.22) | 0.97 (0.77–1.22) | 0.820 |
| ≥65 | 1792 | 144 (8.0) | 0.92 (0.73–1.16) | 0.88 (0.69–1.10) | 0.276 |
| Unknown | 6 | – | |||
| Gender | – | ||||
| Male | 4868 | 413 (8.5) | Ref | Ref | |
| Female | 3944 | 352 (8.9) | 1.05 (0.91–1.20) | 1.04 (0.91–1.19) | 0.521 |
| Transgender | 10 | 2 (20.0) | 2.35 (0.68–8.17) | 1.97 (0.54–7.19) | 0.301 |
| Enrollment Center | |||||
| District | 145 | 18 (12.4) | 1.6 (1.03–2.48) | 1.41 (0.91–2.18) | 0.122 |
| Peripheral health institute | 8221 | 636 (7.7) | Ref | Ref | |
| Private chemist | 9 | 2 (22.2) | 2.87 (0.84–9.77) | 1.62 (0.45–5.83) | 0.459 |
| Private health facility | 167 | 27 (16.2) | 2.09 (1.46–2.97) | 1.86 (1.31–2.65) | <0.001 |
| Private lab | 17 | 1 (5.9) | 0.76 (0.11–5.09) | 0.62 (0.09–4.16) | 0.625 |
| Tuberculosis unit | 248 | 83 (33.5) | 4.34 (3.59–5.25) | 3.66 (3.0–4.42) | <0.001 |
| Unknown | 15 | – | |||
| Contact of TB case | |||||
| Yes | 141 | 5 (3.5) | 0.4 (0.17–0.95) | 0.42 (0.17–1.00) | 0.052 |
| No | 8681 | 762 (8.8) | Ref | Ref | |
| Diabetes mellitus | |||||
| Yes | 241 | 11 (4.6) | 0.51 (0.28–0.92) | 0.76 (0.42–1.37) | 0.368 |
| No | 8566 | 756 (8.8) | Ref | Ref | |
| Unknown | 15 | – | – | ||
| Tobacco intake | |||||
| Yes | 344 | 20 (5.8) | 0.65 (0.42–1.01) | 0.9 (0.91–1.39) | 0.665 |
| No | 8478 | 747 (8.8) | Ref | Ref | |
| HIV status | |||||
| Positive | 107 | 10 (9.3) | 1.79 (0.97–3.27) | 1.79 (0.97–3.28) | 0.059 |
| Negative | 4195 | 219 (5.2) | Ref | Ref | |
| Unknown | 4520 | 538 (11.9) | 2.27 (1.95–2.65) | 2.06 (1.76–2.41) | <0.001 |
TB test, Sputum smear microscopy, cartridge-based nucleic acid amplification tests, Culture and drug susceptibility tests for Mycobacterium tuberculosis, chest radiography; RR, relative risk; aRR, adjusted relative risk.
Demographic and clinical characteristics of presumptive TB patients who did not undergo any test for TB in Dakshina Kannada, India, January–March, 2019 (N = 8822)
Similarly, we assessed for the association between various demographic and clinical factors with a diagnosed TB positive patient not initiated on treatment. On bivariable analysis patients diagnosed from a private health facility or private laboratory, retreatment cases had higher probability of not getting initiated on treatment (Table 3).
| Variables | Total | Not initiated on treatment | RR (95% CI) | aRR (95% CI) | p-value |
|---|---|---|---|---|---|
| N = 822 | n (%) | ||||
| Total | 26 (3.2) | ||||
| Age (years) | |||||
| <15 | 22 | 0 | – | – | |
| 15–24 | 114 | 3 (2.6) | 0.8 (0.19–3.27) | 0.74 (0.17–3.23) | 0.691 |
| 25–34 | 135 | 5 (3.7) | 1.12 (0.33–3.80) | 1.21 (0.32–4.58) | 0.775 |
| 35–44 | 152 | 5 (3.3) | Ref | Ref | |
| 45–54 | 173 | 5 (2.9) | 0.87 (0.25–2.97) | 1.05 (0.32–3.45) | 0.935 |
| 55–64 | 120 | 3 (2.5) | 0.76 (0.18–3.11) | 0.88 (0.20–3.73) | 0.866 |
| ≥65 | 106 | 5 (4.7) | 1.43 (0.42–4.83) | 1.46 (0.36–5.81) | 0.591 |
| Gender | |||||
| Male | 561 | 16 (2.9) | Ref | Ref | |
| Female | 260 | 10 (3.8) | 1.34 (0.62–2.93) | 1.38 (0.67–2.85) | 0.374 |
| Transgender | 1 | 0 | |||
| Enrollment Center | |||||
| District | 0 | 0 | – | – | |
| Peripheral health institute | 679 | 15 (2.2) | Ref | Ref | |
| Private chemist | 7 | 0 | – | – | |
| Private health facility | 105 | 7 (6.7) | 3.01 (1.26–7.22) | 2.73 (1.08–6.90) | 0.034 |
| Private lab | 16 | 2 (12.5) | 5.65 (1.40–22.70) | 5.12 (1.38–18.92) | 0.014 |
| Tuberculosis unit | 0 | 0 | – | – | |
| Unknown | 15 | 2 (13.3) | |||
| Contact of TB case | |||||
| Yes | 24 | 1 (4.2) | 1.33 (0.18–9.41) | 0.83 (0.85–8.24) | 0.880 |
| No | 798 | 25 (3.1) | Ref | Ref | |
| Diabetes mellitus | |||||
| Yes | 106 | 1 (0.9) | 0.26 (0.03–1.93) | 0.33 (0.04–2.7) | 0.304 |
| No | 701 | 25 (3.6) | Ref | Ref | |
| Type of TB | |||||
| New | 729 | 18 (2.5) | Ref | Ref | |
| Recurrent | 93 | 8 (8.6) | 3.04 (1.55–7.78) | 3.2 (1.38–7.46) | 0.007 |
RR, relative risk; aRR, adjusted relative risk.
Demographic and clinical profile of notified TB patients who were not initiated on TB treatment in Dakshina Kannada, India, January–March, 2019 (N = 822)
Seventeen staff of the public health system were approached for the KIIs and 15 of them consented to participate in the interview. They were: three MO’s, one STS, one STLS, one laboratory technician, two pharmacists, one staff nurse, one health worker, three TB health visitors, one lower division clerk and one public–private mix coordinator. The qualitative findings exploring the implementation challenges in the diagnostic and treatment cascade of presumptive TB patients have been presented in two separate sections: perceived facilitators and barriers. They have been summarised in Figure 3.
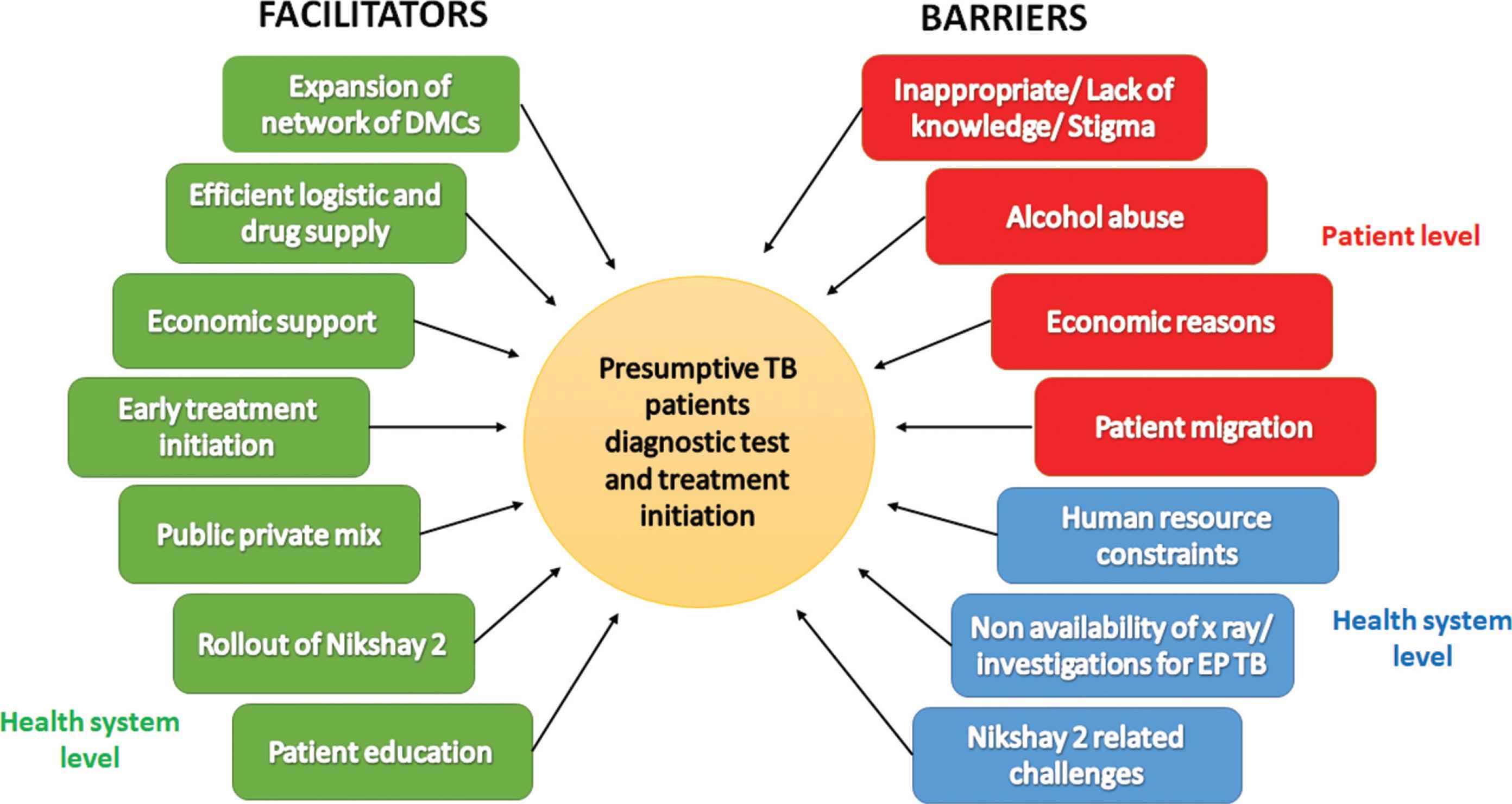
Non-hierarchical thematic diagram showing facilitating factors and barriers for presumptive TB patients to undergo diagnostic test and treatment initiation in Dakshina Kannada, India. DMCs, Designated Microscopy Centers; Nikshay, Web-based TB recording and reporting platform; EP TB, extrapulmonary tuberculosis.
3.1. Facilitators
- (i)
Expansion of network of DMCs: Currently, all the primary health centers are upgraded to function as microscopy centers under RNTCP with the laboratory technician of the primary health centers trained in performing sputum microscopy and send the sputum for CB-NAAT testing and enter the details on Nikshay-2.
- (ii)
Efficient logistics and drug supply: Timely supply of lab consumables and drugs ensures that the investigations are performed without delay and the patient is not made to wait for starting treatment.
- (iii)
Economic support: The health care staff interviewed felt that the introduction of monetary benefits for the patients under RNTCP such as Nikshay Poshan Yojana and some local financing mechanisms at the level of PHCs act as facilitators.
“Now due to the monetary benefit, when we counsel the patients that along with medicines you will get money for food, patient acceptance is better.”
(TBHV, 37 years, female)“I help the patients from the Arogya Raksha Samithi (patient welfare committee) fund including reimbursement for chest radiograph done in private medical college hospital when they bring the bill.”
(MO, 55 years, male) - (iv)
Early treatment initiation: Starting the treatment early for patients who were found to be sputum positive helps to reduce the pre-treatment loss to follow up.
- (v)
Public private mix: The health workers felt that the involvement of the medical colleges in the programme is good. There is an increase in the number of presumptive TB patients and TB patients notified from the medical colleges. The medical college also helps in providing a larger basket of diagnostic tests.
“The details of the patients who have taken anti-TB drugs from the hospital pharmacy are provided to us which helps in identifying the cases which have not been notified and take follow-up actions.”
(TBHV, 45 years, female) - (vi)
Roll out of Nikshay-2: The health workers interviewed felt that the Nikshay-2 is an efficient system for patient data capture. It avoids duplication of patient records. There is also better co-ordination of logistics especially while placing order for medicines. Overall, it helps in improving referral and feedback mechanism across health facilities. There was also mention of the user friendly mobile application.
“Before Nikshay, we would just make note of presumptive cases sent to DMC and there was no follow up, whether the sample was processed or not.”
(MO, 55 years, male) - (vii)
Patient education: The health care providers felt that educating patients about the disease and its treatment has helped them to accept the tests and the treatment.
“We give counselling from the beginning to the end of treatment. This helps in better treatment acceptance by the patients. We also tell them the facts that if you do not take the tablets properly now, then you will need to take double tablets along with injections in future.”
(TBHV, 47 years, male)
3.2. Barriers
The barriers identified have been segregated into patient level barriers (four) and health system level barriers (three).
3.2.1. Patient level barriers
- (i)
Inappropriate/lack of knowledge/stigma: According to the health care staff, a presumptive TB patient is in a state of denial and lacks risk perception. There is also a fear of disease and its long course of treatment along with a lack of trust in the public health system.
“For some patients when they are asked to undergo TB test, they don’t like it. They tell no one in our family has TB and that’s why they do not want the TB test.”
(STLS, 44 years, female) - (ii)
Alcohol abuse: People with alcohol abuse generally do not get themselves tested for TB.
“In an alcoholic patient, if family members force and bring him to health center, the person will tell that he does not have any problem and he is fine. Instead of giving sputum, they will give saliva and we may miss the diagnosis.”
(STLS, 44 years, female) - (iii)
Economic reasons: Patients especially daily wage workers need to lose their income and also take care of the transportation costs during their travel to the health facilities. This acts as a barrier to get them to undergo the tests early.
“If I am sick and need to go to a health center, I need money. I may need to borrow it. Who will give the transport charges? This was asked by a patient to me”
(MO, 55 years, male) - (iv)
Patient migration: It is difficult to enroll patients who are from outside the state/country under Nikshay and have a follow up as mentioned by a health worker.
“We had a patient from Nepal who is a canteen worker and had received 2 months of TB treatment there. Now, how do I show this case in Nikshay?”
(TBHV, 45 years, female)
3.2.2. Health system level barriers
- (i)
Human resource constraints: Non-availability of lab technicians was cited by a heath care provider as one of the reasons for losing patients before getting their sputum tested.
“We do not have a lab technician in our PHC. For presumptive TB patients, we cannot have a sputum examination here and we send them to the DMC of taluk hospital. They may not go and this could be a reason for missing cases.”
(MO, 30 years, male) - (ii)
Non-availability of X-ray facility/other investigations for extrapulmonary TB: Non availability of diagnostic facilities in the public health sector was mentioned by the health workers as a barrier for not getting evaluated as per the diagnostic algorithm by patients.
“In smear negative cases, sending them for X-ray is a problem.”
(MO, 55 years, male) - (iii)
Nikshay-2 related: Apart from the above mentioned facilitators and barriers, there were challenges about the Nikshay-2 the interviewees also mentioned a few issues in recording, updating and tracking information on presumptive TB patients in Nikshay-2.
4. DISCUSSION
This is one of the first studies from India to assess the diagnostic tests undergone by persons with presumptive TB enrolled in Nikshay-2 and whether the diagnosed TB patients have been initiated on treatment. This study showed that 8.7% of the persons with presumptive TB in this cohort had not undergone any diagnostic test and of those diagnosed with TB, 3.2% were not initiated on treatment. The study also highlights that CB-NAAT testing remains low as only 13.5% of the presumptive TB persons got evaluated by it.
This study’s findings have the following implications on policy and practice.
First, nearly 98% of the persons with presumptive TB enrolled on Nikshay-2 were from the public health facilities (includes private medical college hospitals). Dakshina Kannada district has large numbers of private health facilities with a large number of people (including those with TB symptoms) seeking health care from private health facilities [21,22]. Therefore, only 2% from the private sector indicates major deficiencies in enrolling persons with presumptive TB from the private health facilities. The qualitative part of our study also indicates that the engagement and participation of the private health facilities in the TB control efforts in the district is sub-optimal. The exact reasons why private health care facilities do not report details of persons with presumptive TB in Nikshay-2 is unknown and this is an area for future research. Undertaking this research will help in formulating context specific strategies to address this deficiency.
Second, we found that about 9% of the presumptive TB patients did not undergo any of the diagnostic tests and about 12% had not undergone any of the microbiological tests. This is for the first time that such data is available from any district in the country, and therefore, we are unable to compare and contrast this study finding with any other studies. Globally, in some countries, ‘cough registers’ or ‘presumptive TB registers’ are maintained for documenting and tracking whether persons with presumptive TB have undergone TB tests or not. Studies from these countries have previously reported that 7–19% of those enrolled in such registers had not undergone any of the desired TB test [23–25]. Persons with presumptive TB not undergoing any diagnostic tests are missed opportunities for TB diagnosis which must be reduced on-priority by programmatic efforts.
Third, about 77.5% and 13.5% of the persons with presumptive TB enrolled in Nikshay-2 had undergone sputum smear microscopy and CB-NAAT respectively. We did not have information on chest radiography status of all the persons with presumptive TB. It was not clear whether this is due to the deficiency in data entry, data extraction from Nikshay-2 or operational challenges in tracking whether the enrolled presumptive TB patients have undergone chest radiography. Unfortunately, we did not explore this aspect in our qualitative study, and therefore, we are unable to provide any insights into it. As we did not have information on chest radiography results (because it was not recorded in Nikshay), we were unable to assess whether all those with chest radiography lesions suggestive of TB underwent CB-NAAT test or not. Given this scenario, we believe that sputum smear microscopy of 77.5% and particularly CB-NAAT of 13.5% in this cohort is low and this should be an area for major concern. Currently there are two CB-NAAT testing centres where the samples are being sent through an established courier mechanism. There is a need to have more CB-NAAT testing centres in the district to support evaluation of all the suspected TB cases as per the standard guidelines.
Fourth, as per the India’s National TB Programme guidelines, all presumptive TB patients should be offered voluntary HIV counselling and testing and those found to be HIV positive are expected to be fast tracked for TB testing [2]. As per the data shown in Table 2, nearly half of presumptive TB patients had not undergone HIV testing (i.e., those with “unknown” results). We do not know whether those with “unknown” test results were not offered voluntary counselling and testing or they refused to undergo HIV testing. In addition, the proportion not tested for TB appears to be relatively higher among those with HIV ‘unknown’ or HIV ‘positive’ results when compared those with HIV negative results. We feel that this association is not an epidemiological or clinical association but an association highlighting similar operational challenges in testing such patients for TB.
Fifth, several facilitators and barriers were reported by the interviewed health care providers as affecting the uptake of diagnostic tests and TB treatment. These are similar to what has been reported from previous literature [8,23,26]. We feel that these facilitators and barriers may exist in other districts of Karnataka state and also in other districts of the country. Therefore, RNTCP must not sideline these findings as a random finding of one district, but instead formulate policies/strategies to address these barriers across the country.
Sixth, nearly 97% of the diagnosed patients have been initiated on TB treatment with only 3% pre-treatment loss to follow up. This is much lower than what has been reported about pre-treatment loss to follow up in public health facilities [3,7]. Of the several facilitators listed by the interviewees, and based on information from previous literature, we feel that initiating patients on TB treatment within 1 day of diagnosis is the major reason for the low pre-treatment loss to follow up observed in our study [8].
Finally, Nikshay-2 has created a platform for documenting information on each person with presumptive TB identified in the country, the diagnostic tests they undergo, and their TB diagnosis and treatment initiation status. We recommend that every district in the country must utilize the data on this platform and undertake measures to address the gaps in diagnosis and treatment initiation cascade.
The major limitations of the study were: (a) We used data from Nikshay-2 for our study. If there are any deficiencies in recording or updating information on Nikshay-2, then our study results are likely to be biased. Dakshina Kannada is one of the better performing districts in the state of Karnataka with relatively strong supervision and monitoring systems. We believe that the errors in recording patients’ information are likely to be low and random and therefore there are unlikely to be any major biases in the results. (b) We interviewed only health care providers of the public health system to know the facilitators and barriers for TB testing and initiating diagnosed patients on TB treatment. Due to operational constraints, we did not interview a sample of private health care providers or patients to know their perspectives about these issues, and therefore, our study results are deficient on this aspect. (c) We also missed probing a few quantitative study findings in our qualitative study (for e.g., why presumptive TB patients with HIV positive or unknown results were less likely to undergo TB testing) as these issues were identified at a later date while conducting detailed analysis of the quantitative aspects of our study.
5. CONCLUSION
About 9% of PPTB not undergoing any test for TB and 3% of the TB patients not initiated on treatment are of major concern. RNTCP must undertake measures to address the barriers for testing and treatment initiation identified in the study if it has to plug the gaps in loss of patients during TB diagnosis and treatment initiation.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
IMI, AKM, PRN, BMN and SS contributed in study protocol. IMI, AKM and BMN contributed in data collection. IMI, AKM and BMN contributed in data analysis and interpretation. IMI, AKM, PRN and SS contributed in drafting the manuscript (original). IMI, AKM, PRN, BMN and SS contributed in critical review and approval of final manuscript.
FUNDING
The training program, within which this paper was developed, and the open access publication costs were funded by the
ACKNOWLEDGMENTS
This research was conducted through the Structured Operational Research and Training Initiative (SORT IT), a global partnership led by the Special Programme for Research and Training in Tropical Diseases at the World Health Organization (WHO/TDR). The model is based on a course developed jointly by the International Union Against Tuberculosis and Lung Disease (The Union) and Medécins sans Frontières (MSF/Doctors Without Borders). The specific SORT IT programme which resulted in this publication was jointly developed and implemented by: The Union South-East Asia Office, New Delhi, India; the Centre for Operational Research, The Union, Paris, France; Medécins sans Frontières (MSF/Doctors Without Borders), India; Department of Preventive and Social Medicine, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India; Department of Community Medicine, All India Institute of Medical Sciences, Nagpur, India; Department of Community Medicine, ESIC Medical College and PGIMSR, Bengaluru, India; Department of Community Medicine, Sri Manakula Vinayagar Medical College and Hospital, Puducherry, India; Karuna Trust, Bangalore, India; Public Health Foundation of India, Gurgaon, India; The INCLEN Trust International, New Delhi, India; Indian Council of Medical Research (ICMR), Department of Health Research, Ministry of Health and Family Welfare, New Delhi, India; Department of Community Medicine, Sri Devaraj Urs Medical College, Kolar, India; and Department of Community Medicine, Yenepoya Medical College, Mangalore, India.
We thank the State Tuberculosis Officer, Karnataka for providing permission and the staff of District Tuberculosis Office, Dakshina Kannada for providing data required for the study. We thank Dr. Spoorti Gowda and Dr. Shazia Anjum, WHO-RNTCP consultants, Karnataka state and Dr. Nischith KR, WHO-RNTCP consultant, Chattisgarh for their technical support. We acknowledge Dr. Chidananda Sanju, District Tuberculosis Officer, Udupi, Karnataka for permitting and facilitating pilot testing of the key informant interview guide in Udupi. We thank Dr. Abhay S Nirgude, Professor and Head, Department of Community Medicine, Yenepoya Medical College, Mangalore for his motivation and technical support toward the study. We thank the health care providers who kindly agreed to participate and provided valuable insights to the study.
SUPPLEMENTARY TABLE
| Variables | Total | Not undergone any microbiological TB test* | RR (95% CI) | aRR (95% CI) | p-value |
|---|---|---|---|---|---|
| N = 8822 | n = 1025 (11.6%) | ||||
| Age (years) | |||||
| <15 | 404 | 55 (13.6) | 1.15 (0.86–1.53) | 1.16 (0.87–1.55) | 0.285 |
| 15–24 | 683 | 96 (14.1) | 1.19 (0.94–1.51 | 1.14 (0.91–1.44) | 0.240 |
| 25–34 | 1073 | 160 (14.9) | 1.26 (1.02–1.55) | 1.18 (0.97–1.45) | 0.094 |
| 35–44 | 1323 | 156 (11.8) | Ref | Ref | |
| 45–54 | 1801 | 209 (11.6) | 0.98 (0.80–1.19) | 1 (0.83–1.21) | 0.934 |
| 55–64 | 1740 | 177 (10.2) | 0.86 (0.70–1.05) | 0.86 (0.70–1.05) | 0.151 |
| ≥65 | 1792 | 172 (9.6) | 0.81 (0.66–0.99) | 0.81 (0.66–0.99) | 0.048 |
| Unknown | 6 | 0 | – | – | |
| Gender | |||||
| Male | 4868 | 577 (11.9) | Ref | Ref | |
| Female | 3944 | 446 (11.3) | 0.95 (0.84–1.07) | 0.96 (0.85–1.07) | 0.515 |
| Transgender | 10 | 2 (20.0) | 1.68 (0.48–5.84) | 0.84 (0.22–3.12) | 0.796 |
| Enrollment Center | |||||
| District | 145 | 18 (12.4) | 1.24 (0.80–1.93) | 1.2 (0.78–1.86) | 0.394 |
| Peripheral health institute | 8221 | 818 (9.9) | Ref | Ref | |
| Private chemist | 9 | 8 (88.9) | 8.93 (7.02–11.35) | 6.96 (5.6–8.67) | <0.001 |
| Private health facility | 167 | 84 (50.3) | 5.05 (4.29–5.95) | 4.71 (3.97–5.59) | <0.001 |
| Private lab | 17 | 12 (70.6) | 7.09 (5.18–9.70) | 6.08 (4.35–8.51) | <0.001 |
| Tuberculosis unit | 248 | 83 (33.6) | 3.37 (2.80–4.07) | 3.23 (2.68–3.9) | <0.001 |
| Unknown | 15 | 2 (13.3) | – | – | |
| Contact of TB case | |||||
| Yes | 141 | 11 (7.8) | 0.66 (0.37–1.18) | 0.69 (0.39–1.22) | 0.204 |
| No | 8681 | 1014 (11.7) | Ref | Ref | |
| Diabetes mellitus | |||||
| Yes | 241 | 33 (13.7) | 1.18 (0.86–1.63) | 1.5 (1.07–2.1) | 0.016 |
| No | 8566 | 988 (11.5) | Ref | Ref | |
| Unknown | 15 | 4 (26.7) | 2.31 (0.99–5.36) | 1.18 (0.52–2.69) | 0.682 |
| Tobacco intake | |||||
| Yes | 344 | 28 (8.1) | 0.69 (0.48–0.99) | 0.87 (0.6–1.25) | 0.469 |
| No | 8478 | 997 (11.8) | Ref | Ref | |
| HIV status | |||||
| Positive | 107 | 15 (14.0) | 1.46 (0.90–2.36) | 1.54 (0.95–2.50) | 0.08 |
| Negative | 4195 | 401 (9.6) | Ref | Ref | |
| Unknown | 4520 | 609 (13.5) | 1.4 (1.25–1.58) | 1.26 (1.11–1.42) | <0.001 |
Microbiological TB test, Sputum smear microscopy, cartridge-based nucleic acid amplification tests, culture and drug susceptibility tests for Mycobacterium tuberculosis; RR, relative risk; aRR, adjusted relative risk.
Demographic and clinical characteristics of presumptive TB patients who did not undergo any microbiological test for TB in Dakshina Kannada, India, January–March, 2019 (N = 8822)
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Imaad Mohammed Ismail AU - Akshaya Kibballi Madhukeshwar AU - Poonam Ramesh Naik AU - Badarudeen Mohammad Nayarmoole AU - Srinath Satyanarayana PY - 2020 DA - 2020/05/23 TI - Magnitude and Reasons for Gaps in Tuberculosis Diagnostic Testing and Treatment Initiation: An Operational Research Study from Dakshina Kannada, South India JO - Journal of Epidemiology and Global Health SP - 326 EP - 336 VL - 10 IS - 4 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.200516.001 DO - 10.2991/jegh.k.200516.001 ID - Ismail2020 ER -