
Care-Related Quality of Life of Caregivers of Beta-Thalassemia Major Children: An Epidemiological Study in Eastern India
- DOI
- 10.2991/jegh.k.200102.003How to use a DOI?
- Keywords
- Thalassemia; caregivers; quality of life; education; knowledge; social discrimination
- Abstract
Caregivers are the persons who provide care at the time of distress or illness. They face many stress and strain to provide the best possible medical care for their children. There are very few studies that explored the care-related quality of life (CarerQoL) of the caregivers of thalassemic children and its correlates. With this background, the current study was designed to explore the CarerQoL of the caregivers of β-Thalassemia Major (β-TM) children and its various correlates. It was a cross-sectional observational study conducted among caregivers of β-TM children attending a tertiary care health facility of Eastern India in between May 2016 and April 2017 with a structured schedule. The median CarerQoL score was found to be 5 with an interquartile range of 4–7 (range: 11). In the final multivariable logistic regression model, care receivers’ (thalassemic children) age [adjusted odds ratio (AOR): 2.2 (1.2–4.2)], spleen status [AOR: 4.1 (2.0–8.7)], blood transfusion frequency [AOR: 2.1 (1.1–3.9)], and quality of life (QoL) [AOR: 3.0 (1.6–5.5)] and caregivers’ educational level [AOR: 2.3 (1.2–4.1)], perceived social discrimination [AOR: 2.3 (1.3–4.1)], debt [AOR: 2.3 (1.2–4.3)], nongovernmental organization assistance [AOR: 2.0 (1.0–4.0)], and wage loss due to seeking treatment [AOR: 1.9 (1.1–3.4)] were significant predictors of CarerQoL of the study participants adjusted with their age, sex, working status, per-capita monthly income, knowledge level related to the disease, and care receivers’ comorbidity status. To conclude, CarerQoL of the study participants were significantly associated with QoL of their wards. Other significant associates of CarerQoL were caregivers’ education level, financial profile, patients’ age, and their clinico-therapeutic profile.
- Copyright
- © 2020 Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Thalassemia was coined from the Greek word “thalassa” meaning “the sea” because the condition was first observed in populations living near the Mediterranean Sea [1]. It arises from mutations, leading to deficient globin chain biosynthesis with high incidence rate affecting a large area of the globe extending from the Mediterranean Basin and parts of Africa, throughout the Middle East, the Indian subcontinent, Southeast Asia, and Melanesia into the Pacific Islands [2–4]. In India, the carrier rate for β-thalassemia varies from 1% to 17% with 10,000 children (one-tenth of the world) with β-thalassemia major (β-TM) are born every year [5–9]. It had been well documented that in West Bengal, every 10th person is a thalassemia carrier with abundance in Muslim, scheduled caste, and scheduled tribe populations [10].
Caregivers are the persons who provide care at the time of distress or illness. In the case of chronic diseases like thalassemia, their role becomes more evident. They face many challenges in providing high-quality care for their children. By definition, caregiver burden refers to a high level of stress or strain one experiences while caring for another person (usually a family member) with some illness. For example, a person caring for someone with a chronic disease like thalassemia may experience stressors such as financial strain, physical strain, their mental health, relationship with the care receiver, and social support. Cost of treatment of the disease and its complications impose a significant burden on the clients of thalassemia. It also imposes a significant burden on their caregivers too and the society at a large [11–13].
Caregivers of thalassemic children face many stress and strain to provide the best possible medical care for their children. Their quality of life (QoL), especially care-related quality of life (CarerQoL), is expected to be poor and dependent on QoL of their ward and other attributes (i.e., sociodemographic, clinico-therapeutic, perception related, financial) [11–26]. Determinants of QoL are different for different countries due to difference in sociocultural, socioeconomical, ethnicity, and other factors. Extensive research on therapeutic aspects of thalassemia are going on throughout the world compared to studies exploring QoL and its determinants, despite being equally important are very few. Again, most of the prior studies conducted on the area had investigated QoL of the thalassemic child only [27–33], ignoring the QoL of their caregivers. The researcher strongly felt that the assessment of QoL, especially CarerQoL of caregivers, is as essential as their wards’ QoL because there suffering is no less. Thus, the current study was designed to assess the CarerQoL of caregivers of β-TM children and also to determine the explanatory and contextual factors affecting it.
2. MATERIALS AND METHODS
The study was an observational study with a cross-sectional design. It was conducted among 328 caregivers with children affected by β-TM. Our method for data collection was face-to-face interview in a thalassemia outpatient department (OPD) of a medical college of Kolkata, West Bengal, situated in the eastern part of India from May 2016 to April 2017 with a structured schedule.
The schedule consisted of sociodemography (age, sex, education, and residence), socioeconomy [working status and per-capita monthly income (PCMI)] clinico-therapeutic [age at diagnosis, blood transfusion frequency, transfusion-transmitted infections (TTIs), last pre-transfusional hemoglobin (Hb) level, spleen status, and iron chelation status], caregivers’ knowledge regarding the disease, perceived level of social discrimination, Peds4QL [34] for assessing QoL of thalassemic children, and CarerQoL 7D [35] for QoL assessment of the caregivers of thalassemic children. The schedule was administered by the principal investigator himself to all the study participants. Notably, the study was conducted only on known β-TM children. These children were diagnosed as having β-TM by the medical officer in charge of the thalassemia unit using diagnostic criteria as a patient with Hb <7 g% with Hb F ≥70% and Hb A <30% on Hb electrophoresis at the time of diagnosis. After being diagnosed, these β-TM children attend thalassemia unit outdoor to get assessed by the concerned medical officer in charge for the need of blood transfusion (by Hb measurement and clinical examination) and other therapeutic interventions (i.e., iron chelators, vaccinations). Mostly, these visits are follow-up visits for treatment.
β-TM children who had at least received one blood transfusion in the previous year and attended thalassemia day care unit along with a caregiver during the study period and consented to participate were included in the study. On the other hand, those who were critically ill were excluded. Here “critically ill” means thalassemic children who were bedridden and urgently required medical intervention to survive at the time of the data collection. One day in a week was allotted for data collection. On an average, thalassemia unit OPD serves 15–20 β-TM patients on a single day. Every second patient with accompanying caregiver attending the OPD was approached for the study by the principal investigator. Notably, the principal investigator of the study was a junior resident doctor then. An interview took on an average of 15–20 minutes. On average, eight patients and their caregivers could be interviewed on a single day. Before each interview, study participants were asked if they were interviewed before to prevent duplication. Total 41 days were available for data collection (excluding public holidays) in 1 year by this method and 328 caregivers could be interviewed in the stipulated study period. Among 328 study participants, data of 324 were analyzed for determining their CarerQoL and its predictors. Details were depicted in Figure 1.
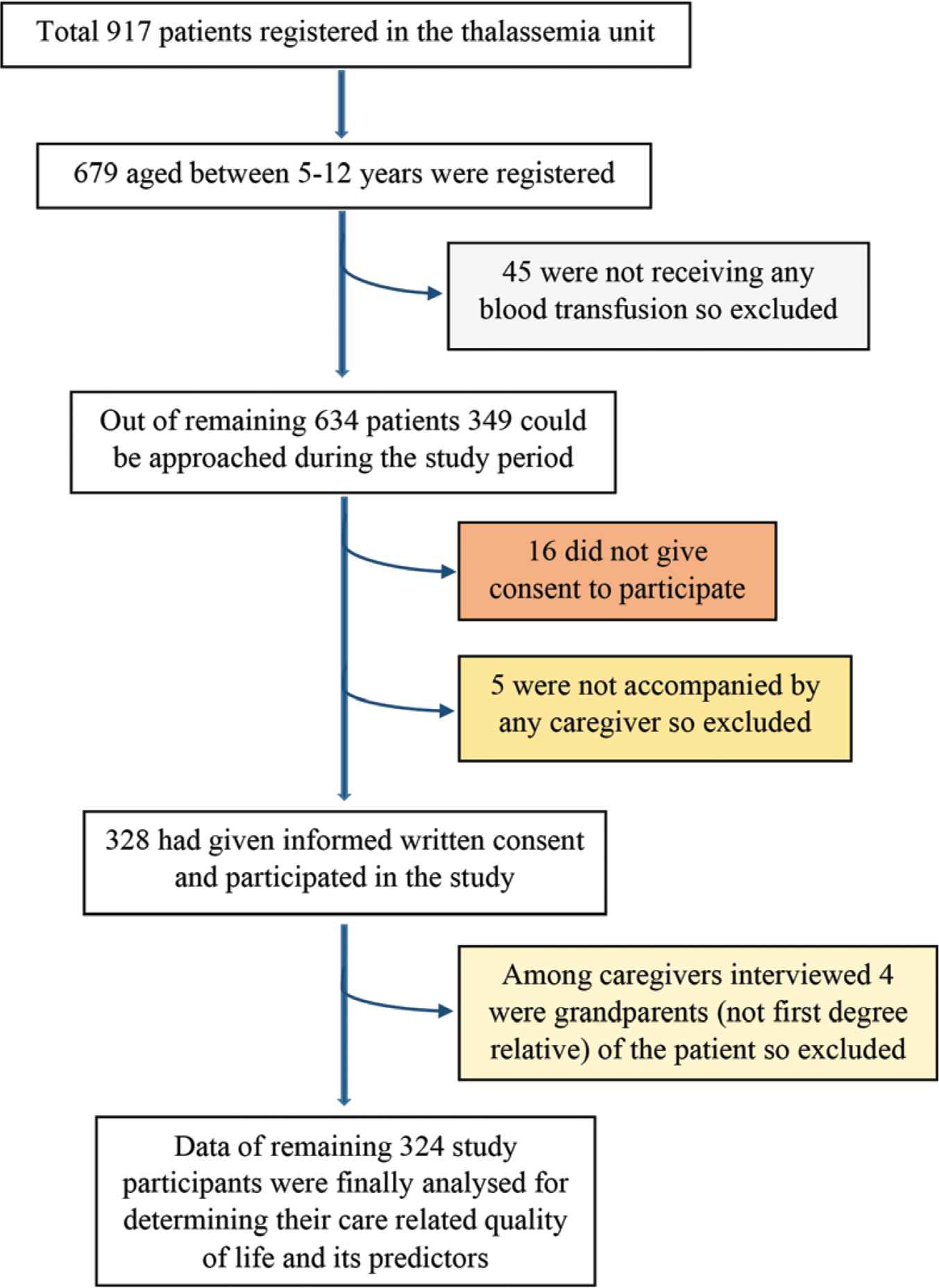
Flowchart showing selection of study participants.
Some operational definitions used in the study were as following:
2.1. CarerQoL Score
Scores of all items of the scale were added to obtain the total score. Summing the values for the seven dimensions, a score of 0 translates into the worst informal care situation; higher the score, better the care situation [35]. The minimum and maximum attainable scores were 0 and 14, respectively. As total CarerQoL score was not normally distributed as Kolmogorov–Smirnov and Shapiro–Wilk tests were significant. The CarerQoL score was divided into two outcomes (favorable and unfavorable) by its median (5) to perform a logistic regression analysis.
2.2. Peds4QL Score
Items of the Peds4QL scale were reverse scored and linearly transformed to a 0–100 scale as follows: 0 = 100, 1 = 75, 2 = 50, 3 = 25, and 4 = 0. Scores were obtained by summing of the items over the number of items answered. In this way, the total score was calculated, where higher the score more favorable QoL was [34]. In the present study, those who scored more than the median attained score (54.3) were considered to have favorable QoL.
2.3. Caregiver
In the present study, any adult first-degree relative who accompanied the thalassemic child during a visit to the thalassemia unit of the hospital and currently living with and taking care of the patient was considered as a caregiver.
2.4. Caregivers’ Knowledge Regarding the Disease
It was calculated by the addition of scores they received for each knowledge item where a higher score indicated a higher level of knowledge. The minimum and maximum attainable scores were 0 and 7, respectively. Meanwhile, the minimum and maximum attained scores were the same as achievable scores. Those who had scored more than equal to 4 (median achieved score) were considered having adequate knowledge, while those who scored less than 4 were marked as having unsatisfactory knowledge regarding the disease.
2.5. Transfusion‑Transmitted Infections
Those who were reported to be hepatitis B surface antigen (HBsAg), anti-hepatitis C virus (HCV), and anti-HIV‑1/HIV‑2 as per their medical records were considered as hepatitis B, hepatitis C, and HIV positive, respectively.
2.6. Splenomegaly
It was estimated by palpation of the abdomen of the patient in lying down position and expressed in centimeters.
2.7. Statistical Analysis
Data were analyzed using IBM SPSS (Version 16; Chicago, IL, USA). At first, bivariate analysis was done using Spearman’s rho correlation coefficient in between CarerQoL of the study subjects and its different attributes to identify the significant ones. Then, the significant variables in the bivariate analysis were entered domain wise (sociodemographic, patients’ clinico-therapeutic profile, QoL, caregivers’ perception, and financial profile) in the hierarchical multivariate logistic regression models to find out significant attributes of CarerQoL of the study subjects. Multivariable models were adjusted with the age, sex of the caregiver, and PCMI, despite being insignificant in the bivariate analysis to make the findings of the study more robust. The minimum acceptable confidence level was α = 0.95 for all statistics, and the maximum acceptable significance level was p < 0.05.
2.8. Ethical Considerations
Ethical clearance of Institutional Ethics Committee (IEC) of the respective medical college was taken before conducting the study. Informed written consent of each study participant was taken before their participation. During data collection, their confidentiality was assured.
3. RESULTS
Majority of the caregivers interviewed were mothers (75.9%) with a mean age of 29.8 years and the rest being fathers (24.1%) with a mean age of 34.8 years of the thalassemic children. Two-third of them (66.4%) were educated up to primary level with more than half of them (53.4%) were not working for pay. Most of the thalassemic children were diagnosed as thalassemic within the first year of their lives (55.9%) with a mean age at diagnosis of 20.4 months. Three-fifth (60.8%) of them were having a palpable spleen while the palpable size of spleen ranged from 1 to 8 cm. Majority of them were receiving blood transfusion once or less than once a month (63.9%) with most having pre-transfusional Hb level between 5.3 and 5.9 g/dl (35.2%). Two-fifth of them (39.8%) were suffering from TTIs, of which 34.3% were anti‑HCV positive, while 4.3% and 1.9% were HBsAg and anti‑HIV positive, respectively (Table 1).
| Variables | Mean ± standard deviation, n (%) |
|---|---|
| Caregiver interviewed (concerning the patient) | |
| Father | 78 (24.1) |
| Mother | 246 (75.9) |
| Age of the caregiver in completed years | 31.8 ± 6.3 |
| Educational level of the caregiver: (completed years of schooling) | |
| Illiterate (0) | 76 (23.5) |
| Below primary (0–4) | 58 (17.9) |
| Primary (5–7) | 81 (25.0) |
| Middle (8–9) | 64 (19.8) |
| Secondary and above (≥10) | 45 (13.8) |
| Occupation of the caregiver | |
| Not working | 173 (53.4) |
| Semi-skilleda | 62 (19.2) |
| Unskilledb | 81 (25.0) |
| Professionalc | 5 (1.5) |
| Service | 3 (0.9) |
| Age of the patient in completed years | 8.0 ± 2.3 |
| Sex of the patient | |
| Male | 177 (54.6) |
| Female | 147 (45.4) |
| Place of residence | |
| Urban | 91 (28.1) |
| Rural | 233 (71.9) |
| Per-capita monthly income in USD | 23.2 ± 12.5 |
| Number of blood transfusion received by the patient in the previous year | 11.6 ± 4.8 |
| Last pre-transfusional Hb level of the patient in g/dl | 5.5 ± 0.8 |
| Whether patient had undergone splenectomy: (Yes) | 81 (25.0) |
| Size of the palpable spleen of the patient in cm | 2.9 ± 2.8 |
| Whether the patient is on iron chelators: (Yes) | 302 (93.2) |
| Duration since patient receiving iron chelators in months | 33.3 ± 21.4 |
| Caregivers who had faced social discrimination for being a caregiver of a thalassemic child: (Yes) | 135 (41.7) |
| Caregivers who had taken loan for treatment of the patient: (Yes) | 239 (73.8) |
| Caregivers who had received nongovernmental organization assistance for treatment of the patient: (Yes) | 68 (21.0) |
| Caregivers who had lost their wage in order to seek treatment for the patient: (Yes) | 185 (57.1) |
Includes ASHA, Biri binder, cook, barber, driver, carpenter, cobbler, electrician, mechanic, mason, mosaic worker, gold smith, factory worker, tailor, shopkeeper, vendor.
Includes aya, cultivator, farmer, housemaid, laborer, maulana, rickshaw puller, watchman.
Includes school teacher, lawyer, painter.
Background characteristics of the study participants: n = 324
Table 2 shows knowledge of caregivers regarding different aspects of thalassemia. The attained knowledge score had a mean ± standard deviation of 3.5 ± 1.5 and a median (interquartile range) of 4 (2–5).
| Variables | Frequency | Percentage (%) | Score |
|---|---|---|---|
| Do you know how this disease is caused? | |||
| Yes | 189 | 58.3 | – |
| No | 135 | 41.7 | |
| Cause of thalassemia as specified by the caregiver | |||
| Correct knowledge (genetic) | 156 | 48.2 | 1 |
| Incorrect knowledge(destiny/contact with other thalassemic) | 33 | 10.1 | 0 |
| Do not know | 135 | 41.7 | 0 |
| Have you ever heard about premarital counseling? | |||
| Yes | 168 | 51.8 | 1 |
| No | 156 | 48.2 | 0 |
| Have you ever heard about antenatal screening? | |||
| Yes | 163 | 50.3 | 1 |
| No | 161 | 49.7 | 0 |
| Do you know about the treatment of thalassemia? | |||
| Yes | 300 | 92.6 | – |
| No | 24 | 7.4 | |
| Treatment modalities as specified by the caregivera | |||
| Only blood transfusion | 54 | 16.7 | 1 |
| Only iron chelation | 0 | 0.0 | 1 |
| Both blood transfusion and iron chelation | 246 | 75.9 | 2 |
| Splenectomy | 63 | 19.4 | 1 |
| Bone marrow transplantation | 9 | 2.8 | 1 |
| Do not know | 24 | 7.4 | 0 |
Multiple responses.
Distribution of the study participants according to their knowledge regarding the disease: n = 324
The median total Peds4QL score was 54.3 with an interquartile range of 43.4–67.4 (range: 71.7), while median CarerQoL score was 5 with an interquartile range of 4–7 (range: 11). Individual item responses of CarerQoL 7D are depicted in Table 3.
| No | Some | A lot of | ||||
|---|---|---|---|---|---|---|
| Frequency (%) | Score | Frequency (%) | Score | Frequency (%) | Score | |
| Fulfillment from carrying out care tasks | 99 (30.6) | 0 | 200 (61.7) | 1 | 25 (7.7) | 2 |
| Relational problem with care receiver | 141 (43.5) | 2 | 68 (21.0) | 1 | 115 (35.5) | 0 |
| Problems with own mental health | 38 (11.7) | 2 | 3 (0.9) | 1 | 283 (87.3) | 0 |
| Problems combining my care tasks with own daily activities | 146 (45.1) | 2 | 90 (27.8) | 1 | 88 (27.2) | 0 |
| Financial problem because of my care tasks | 36 (11.1) | 2 | 125 (38.6) | 1 | 163 (50.3) | 0 |
| Support with carrying out my care tasks, when I need it | 215 (66.4) | 0 | 96 (29.6) | 1 | 13 (4.0) | 2 |
| Problems with my own physical health | 46 (14.2) | 2 | 206 (63.6) | 1 | 72 (22.2) | 0 |
Distribution of the study participants according to the responses of various items of care-related quality of life scale: n = 324
In the final multivariable logistic regression model, care receivers’ (thalassemic children) age [adjusted odds ratio (AOR): 2.2 (1.2–4.2)], spleen status [AOR: 4.1 (2.0–8.7)], blood transfusion frequency [AOR: 2.1 (1.1–3.9)], and QoL [AOR: 3.0 (1.6–5.5)] and caregivers educational level [AOR: 2.3 (1.2–4.1)], perceived social discrimination [AOR: 2.3 (1.3–4.1)], debt [AOR: 2.3 (1.2–4.3)], nongovernmental organization (NGO) assistance [AOR: 2.0 (1.0–4.0)], and wage loss due to seeking treatment [AOR: 1.9 (1.1–3.4)] were significant predictors of CarerQoL of the study participants adjusted with their age, sex, working status, PCMI, knowledge level related to the disease, and care receivers’ comorbidity status. Independent variables in the final model were explaining 40.4% variability of the CarerQoL of the study participants with a predictive accuracy rate of 76.9% (Tables 4 and 5).
| A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A | 1.0 | −0.4* | 0.0 | 0.4* | 0.0 | 0.0 | −0.2* | 0.3* | 0.2* | −0.1** | 0.2* | 0.0 | −0.1** | 0.0 | 0.0 | 0.0 | 0.0 | 0.1 | 0.1 | 0.0 |
| B | 1.0 | 0.1** | −0.1 | 0.0 | −0.1** | 0.1** | −0.6* | 0.0 | −0.2* | 0.0 | 0.0 | 0.0 | 0.0 | −0.1 | 0.0 | 0.1 | −0.1 | 0.0 | 0.0 | |
| C | 1.0 | 0.1 | 0.0 | 0.0 | −0.1 | 0.1 | −0.1 | 0.0 | 0.1 | −0.1 | 0.0 | 0.1 | 0.0 | −0.1** | 0.0 | 0.0 | 0.0 | 0.0 | ||
| D | 1.0 | 0.0 | −0.1 | −0.2* | 0.0 | 0.03* | −0.2* | 0.2* | 0.0 | 0.0 | 0.1 | 0.0 | 0.0 | 0.1** | 0.1 | 0.1** | 0.1** | |||
| E | 1.0 | −0.1 | 0.0 | 0.1 | 0.1 | −0.1 | 0.1 | 0.0 | 0.0 | 0.1 | 0.0 | 0.0 | −0.1 | 0.0 | 0.1** | 0.1 | ||||
| F | 1.0 | 0.0 | 0.0 | 0.0 | −0.2* | 0.0 | 0.1** | −0.1** | 0.2* | 0.2* | 0.1** | 0.1 | −0.1** | 0.3* | 0.1** | |||||
| G | 1.0 | −0.2* | −0.1 | −0.1 | 0.0 | 0.0 | 0.0 | 0.0 | 0.1 | 0.1** | −0.1 | 0.0 | 0.0 | 0.1** | ||||||
| H | 1.0 | 0.0 | 0.1 | 0.0 | 0.0 | −0.1 | 0.1 | 0.1 | −0.1 | 0.0 | −0.2* | 0.1 | 0.1** | |||||||
| I | 1.0 | 0.3* | 0.3* | 0.0 | 0.0 | 0.1 | 0.2* | 0.0 | 0.1 | −0.1** | −0.1 | 0.1** | ||||||||
| J | 1.0 | −0.4* | 0.1** | 0.0 | −0.1 | 0.0 | 0.0 | 0.0 | 0.2* | 0.4* | 0.2* | |||||||||
| K | 1.0 | −0.1 | 0.0 | 0.1 | 0.1 | −0.1 | 0.0 | 0.0 | 0.3* | 0.1 | ||||||||||
| L | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.1 | 0.0 | 0.1 | |||||||||||
| M | 1.0 | 0.1** | 0.2* | 0.1 | 0.0 | 0.0 | 0.3* | 0.2* | ||||||||||||
| N | 1.0 | 0.2* | 0.1** | 0.2* | 0.2 | 0.3* | 0.3* | |||||||||||||
| O | 1.0 | 0.0 | 0.0 | 0.0 | 0.2* | 0.3* | ||||||||||||||
| P | 1.0 | 0.1 | 0.0 | 0.1** | 0.2* | |||||||||||||||
| Q | 1.0 | 0.0 | 0.1 | 0.1** | ||||||||||||||||
| R | 1.0 | 0.1 | 0.1** | |||||||||||||||||
| S | 1.0 | 0.4* | ||||||||||||||||||
| T | 1.0 |
Correlation is significant at the 0.01 level.
Correlation is significant at the 0.05 level.
A = age of the caregiver (increasing); B = sex of the caregiver (female); C = per-capita monthly family income (increasing); D = age of the patient (≥8 years); E = sex of the patient (female); F = place of residence (rural); G = caregivers educational level (primary and above); H = caregivers work for pay (yes); I = undergone splenectomy (no); J = blood transfusion frequency (<12 times); K = last pre-transfusional hemoglobin level (increasing); L = taking iron chelators (yes); M = transfusion-transmitted infections (no); N = caregivers knowledge level [(satisfactory) ≥4]; O = caregivers faced discrimination (no); P = taken loan for patient’s treatment (no); Q = received nongovernmental organization assistance (yes); R = wage lost for seeking treatment (no); S = Peds4QL score [(favorable) >54]; T = CarerQoL score [(favorable) >5].
Spearman’s rho correlation matrix showing various correlates of the favorable care-related quality of life (CarerQoL) of the study subjects: n = 324
| Variables | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 |
|---|---|---|---|---|---|
| AORa (95% CI) | AORa (95% CI) | AORa (95% CI) | AORa (95% CI) | AORa (95% CI) | |
| Sociodemographic domain | |||||
| Caregivers age (increasing) | 1.0 (0.9–1.0) | 1.0 (0.9–1.0) | 1.0 (0.9–1.0) | 1.0 (0.9–1.1) | 1.0 (0.9–1.1) |
| Caregivers sex | |||||
| Female | 1.7 (0.8–3.6) | 1.2 (0.6–2.7) | 1.4 (0.6–3.2) | 1.2 (0.5–2.9) | 1.2 (0.5–2.8) |
| Male | Ref. | Ref. | Ref. | Ref. | Ref. |
| Per-capita monthly income (increasing) | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) |
| Age of the patient in years | |||||
| ≥8 | 1.9 (1.1–3.1) | 2.4 (1.4–4.4) | 2.3 (1.3–4.3) | 2.1 (1.1–4.0) | 2.2 (1.2–4.2) |
| <8 | Ref. | Ref. | Ref. | Ref. | Ref. |
| Caregivers educational level | |||||
| Primary and above | 2.0 (1.2–3.3) | 1.9 (1.1–3.1) | 1.8 (1.0–3.1) | 2.2 (1.2–4.0) | 2.3 (1.2–4.1) |
| Below primary | Ref. | Ref. | Ref. | Ref. | Ref. |
| Caregiver work for pay | |||||
| Yes | 2.2 (1.2–4.0) | 2.1(1.1–3.9) | 2.0 (1.0–4.0) | 2.1 (1.1–4.3) | 2.0 (0.9–4.1) |
| No | Ref. | Ref. | Ref. | Ref. | Ref. |
| Patients’ clinico-therapeutic profile domain | |||||
| Undergone splenectomy | |||||
| No | 3.8 (2.0–7.4) | 3.6 (1.8–7.3) | 4.0 (1.9–8.4) | 4.1 (2.0–8.7) | |
| Yes | Ref. | Ref. | Ref. | Ref. | |
| Blood transfusion frequency | |||||
| <12 units | 3.0 (1.8–5.1) | 2.9 (1.6–5.0) | 3.1 (1.7–5.5) | 2.1 (1.1–3.9) | |
| ≥12 units | Ref. | Ref. | Ref. | Ref. | |
| Had transfusion-transmitted infections | |||||
| No | 2.5 (1.5–4.1) | 2.0 (1.2–3.4) | 1.9 (1.1–3.4) | 1.6 (0.9–2.9) | |
| Yes | Ref. | Ref. | Ref. | Ref. | |
| Caregivers perception domain | |||||
| Caregivers knowledge level | |||||
| [(Satisfactory) ≥4] | 2.2 (1.3–3.8) | 1.7 (1.0–3.0) | 1.5 (0.8–2.6) | ||
| [(Unsatisfactory) <4] | Ref. | Ref. | Ref. | ||
| Caregiver faced discrimination | |||||
| No | 2.5 (1.5–4.4) | 2.6 (1.5–4.6) | 2.3 (1.3–4.1) | ||
| Yes | Ref. | Ref. | Ref. | ||
| Caregivers financial profile domain | |||||
| Taken loan for the patients’ treatment | |||||
| No | 2.4 (1.3–4.5) | 2.3 (1.2–4.3) | |||
| Yes | Ref. | Ref. | |||
| Received nongovernmental organization assistance for the patients’ treatment | |||||
| Yes | 2.1 (1.1–4.0) | 2.0 (1.0–4.0) | |||
| No | Ref. | Ref. | |||
| Wage loss for seeking treatment for the patient | |||||
| No | 1.9 (1.1–3.3) | 1.9 (1.1–3.4) | |||
| Yes | Ref. | Ref. | |||
| Patients’ quality of life domain | |||||
| Patients Peds4QL score | |||||
| [(Favorable) > 54] | 3.0 (1.6–5.5) | ||||
| [(Unfavorable) ≤ 54] | Ref. | ||||
| Negelkerke R2 | 0.072 | 0.222 | 0.310 | 0.366 | 0.404 |
| R2 change | 0.072 | 0.150 | 0.088 | 0.056 | 0.038 |
| Omnibus test | 0.007 | 0.000 | 0.000 | 0.000 | 0.000 |
| Hosmer–Lemeshow | 0.298 | 0.284 | 0.144 | 0.110 | 0.120 |
Adjusted odds ratio.
Hierarchical logistic regression analysis showing predictors of favorable care-related quality of life of the study subjects: n = 324
Figure 2 showing various predictors of CarerQoL of the study subjects in the final multivariable logistic regression model in the forest plot, with patients QoL being the strongest predictor with higher AOR (3.0) and narrow CI (1.6–5.5).
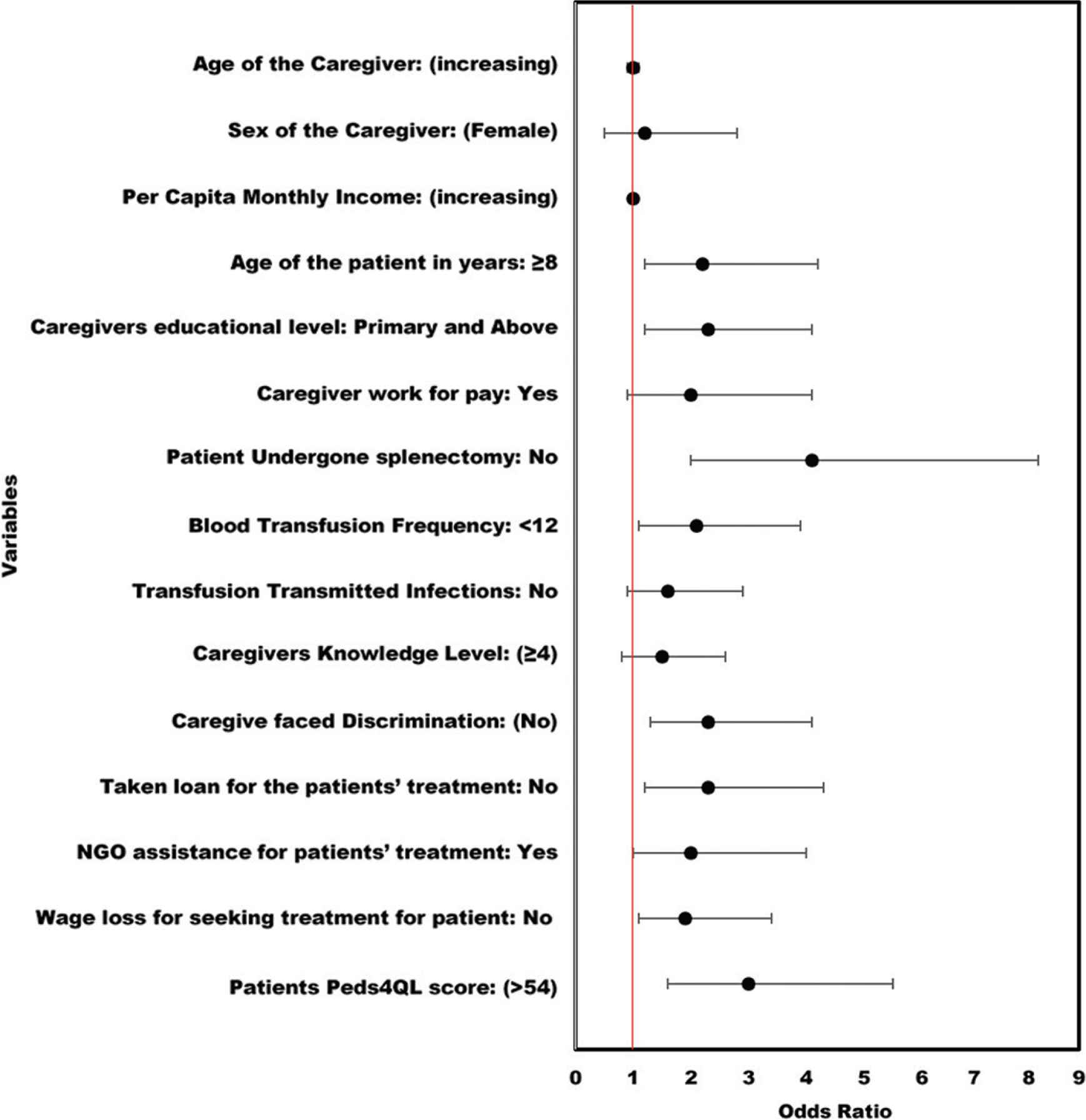
Forest plot showing predictors of care-related quality of life of caregivers of thalassemic children: n = 324.
4. DISCUSSION
It was a cross-sectional, hospital-based observational study, aimed to assess the CarerQoL of the caregivers of β-TM children and also to determine the explanatory and contextual factors affecting it.
In the present study, out of 324, 99 (30.6%) caregivers had no fulfillment on carrying out their care tasks, which was similar to the findings of Aziz et al. [36] (30.0%). Majority of them (87.3%) had problems with their mental health, which was similar to Aziz et al. [36] (82.0%) and somewhat similar to Haq et al. [37], which reported 61.7% depression and 36.7% anxiety among them. Most of them, 206 (63.6%), had some problems with their physical health for their care tasks. This finding was supported by the results of Yengil et al. [38], which reported that β-thalassemia negatively affects the physical and mental components of QoL. One-fourth of them, 88 (27.2%), were facing a lot of problems combining their care tasks with their daily activities, while 146 (45.1%) had no difficulty in doing so. Half of them (50.3%) reported a lot of financial problem because of their care tasks, which was concurrent with the findings of Ishfaq et al. [39]. Two-third of them (66.4%) reported no support in carrying out their care tasks while 96 (29.6%) reported some support, which was contrary to finding of Haq et al. [37] in which 61.7% caregivers reported support from other family members. Of 324 caregivers of the study participants, 135 (41.7%) had favorable QoL. Thalassemia exerts a significant amount of stress and strain on the QoL of their caregivers. The case–control study conducted by Pruthi et al. [40] reported that caregivers of thalassemia patients had significantly higher psychological burden compared to the cerebral palsy group and stated the reason for this being complex treatment and regular visit to the hospital.
Considering sociodemographic attributes of CarerQoL, in the current study, caregivers whose wards age was 8 years or more (median 8 years) had significantly higher odds of having favorable CarerQoL, which was contrary to the findings of Shanmugam et al. [14] that reported positive correlation in between stress and duration of contact of the caregiver with the child. This variability of findings may have resulted from geographical plausibility and the influence of other contextual factors. In our study, caregivers with higher educational level had significantly higher odds of having favorable CarerQoL, which was similar to Ismail et al. [15] and Shaligram et al. [11]. This association was not observed by Inamdar et al. [13], which reported no in-between difference level of education and psychosocial burden of the caregiver. This may be because an educated caregiver is likely to be more resilient, thus have more capabilities to cope up with the stress and strain the disease of his/her child puts onto him/her. Considering the working status of the caregivers, in the present study, those who were working for pay had higher odds of having favorable CarerQoL in all the multivariable logistic regression models except the final model. This was similar to the findings of Miskam et al. [16], which reported that working mothers had good QoL compared to those who were not working, and Hazlina et al. [17], which found significant association between mothers working status and QoL. Financial autonomy enables a caregiver to meet his/her care receiver’s needs more meticulously, which in turn gives more self-satisfaction resulting in the betterment of QoL. In the present study, other sociodemographic attributes like patient’s sex, caregiver’s age, sex, and PCMI of the family did not show any significant association with CarerQoL of the study subjects. The study conducted by Mashayekhi et al. [12] had shown a significant positive correlation of maternal age and caregiver burden, which in turn had an inverse relationship with their income. On the other hand, Muazzam et al. [18] reported male gender of the child, caregivers of younger age, and being female had higher burden compared to others. The variability of the findings may be attributed to geographical plausibility, socioeconomic, and sociocultural differences of the study participants of those studies [17,18] compared to the current research.
Considering patients’ clinico-therapeutic profile-related attributes of CarerQoL, in our study, caregivers whose child did not undergo splenectomy had significantly higher odds of having favorable CarerQoL. Splenectomy reduced blood requirement, thus likely to result in reduced iron deposition and improved QoL of the clients of thalassemia; on the other hand, splenectomy imposes a significant financial burden to the caregivers of these children. In the present study, many of the caregivers borrowed thousands of rupees during their child’s splenectomy. Thus, the inverse relationship of splenectomy and CarerQoL of the study subjects was wholly justified in the present context of the study. In the present study, caregivers whose ward was receiving less than the median number of blood transfusions (12 units) in the previous year had significantly higher odds of having favorable CarerQoL. The findings were concurrent with findings of Shaligram et al. [11], which showed the frequency of blood transfusion as a significant predictor GHQ score of the caregiver. With the reduction in transfusion requirement of a child, hospital visit requirement of the caregiver also reduces, which saves caregivers money and time, which he/she can vest in his/her child-caring or earn wages to offer their child and themselves a better QoL.
On the other hand, with a reduction in transfusion requirement, chances of occurrence of transfusion-related complications in the child also reduces, which may be another cause of finding such results. Considering TTIs, in the current study, caregivers whose ward were not suffering from any TTIs had significantly higher odds of having favorable CarerQoL in all the multivariable model, excepting the final model where it was attenuated adjusted with QoL of the patient. Thalassemia itself a chronic disease; thus, those infected with TTIs laid significant impact on QoL of their caregivers as seen in a study conducted by Bass et al. [19] where HIV-infected children put substantial effects on their caregivers’ QoL.
Considering caregivers’ perception-related attributes of CarerQoL, in the present study, caregivers whose knowledge scores regarding the disease were satisfactory had significantly higher odds of having favorable CarerQoL. A caregiver who has a better understanding of the illness of his child is likely to better cope up with the challenges and difficulties his/her child’s disease presents to him. A knowledgeable caregiver is expected to seek timely, relevant management for his/her child’s illness, which leads to the betterment of their children’s QoL, which in turn results into the improvement of their CarerQoL too. In the present study, caregivers who did not face any discrimination for being a caregiver of a thalassemic child had 2.2 times significantly higher odds of having favorable CarerQoL in the final multivariable model. Social support is vital in maintaining self-esteem, which influences QoL, as shown by Hazlina et al. [17].
On the other hand, discrimination from relatives and neighbors impairs a caregivers’ QoL. A similar finding was observed in a qualitative study conducted in Iran by Shahraki-vahed et al. [20] among parents of thalassemic children where a mother opined “Everybody reproaches us, including relatives and strangers. They allow themselves to talk about our child disease, unfairly and unreasonably…Thus it is not wondering if this behaviour hurts a mother…” Another qualitative study conducted in the United States among caregivers of southeast Asian thalassemic children by Liem et al. [21] where a mother stated “‘sometimes it’s embarrassing because like, somebody who don’t know us but they heard from rumours that my kids have that (thalassemia) and they think that I have disease. Asian and Cambodians, they would think like ‘Oh, she has AIDS, HIV’…so I usually do not tell anyone about it besides our family.”’ The finding indicates the level of stigma/discrimination a caregiver faces for being a caregiver of a thalassemic child.
Considering the financial attributes of CarerQoL, in our study, caregivers who had not taken any loan for their child’s treatment had significantly higher odds of having favorable CarerQoL. Research conducted by Singh et al. [23] shown that immense medical cost makes a substantial financial burden on the families of thalassemic children, which is of significant concern for low-income families. It also reported the reason being that a regularly transfused patient should take iron chelation, periodic relevant laboratory investigations, use of leucocyte filtration blood set, proper immunization, and treatment for complications, which on an average cost around 2500 Indian rupees per month in a government set up, which was afforded by very few in that study. So, it is not surprising that those who were relatively more economically sound (need not to borrow money for the child’s treatment) had better CarerQoL. Similarly, in the present study, those who had received NGO assistance for treatment of their ward had significantly higher odds of having favorable CarerQoL. The survey conducted by Surapolchai et al. [24] showed the importance of financial support in QoL of a thalassemic child, which indirectly affects CarerQoL of their caregivers too. In the present study, caregivers who did not have to lose their wage to seek treatment for their ward had significantly higher odds of having favorable CarerQoL. This finding was supported by finding of a qualitative study by Pouraboli et al. [25] where a father of thalassemic child uttered “One of the most annoying days in the week is the day I come here. I miss a lot of my plan and have to take a day off to come here...” Another qualitative study by Mohammad et al. [26] conducted among Jordanian mothers where one of the participants stated “I have to leave my work because of my child’s illness. He must visit the clinic every month, and I have to stay with him to receive blood and take his medication. Our income is now less than before…” Similarly, in our study, majority of the caregivers were semi-skilled/unskilled laborers. A day of wage loss means a lot for them and affects their CarerQoL.
Considering the relationship between CarerQoL of the caregiver and QoL of their ward, those whose child had favorable Peds4QL score had significantly higher odds of having favorable CarerQoL in both bivariate analysis and multivariable model. This was supported by findings of Shaligram et al. [11] in which QoL of youngster predicted 45% variation of QoL score of the caregiver. This was a prominent outcome as a child whose QoL is favorable is likely to give less stress and strain to his/her caregiver. This leads to the betterment of CarerQoL of their caregivers.
In strengths, it was one of the fewer studies exploring the CarerQoL of the caregivers of the thalassemic children and its various correlates with considerably large sample size than prior studies. It additionally used logistic regression to find out the strength of association of multiple attributes (especially QoL of the clients of thalassemia) of CarerQoL of the caregivers of the thalassemic children, which in turn will help in planning and prioritizing interventions targeting alleviation of this problem.
Limitations of the study were a cross-sectional design, which cannot establish the causal association between CarerQoL and its attributes. For establishing a causal association, a longitudinal design would have been better, but due to feasibility issue and time constraint, it could not be done. On the other hand, some may argue that case–control design would have been better for the study, as done in some previous studies [37,41]. Still, the researcher thought it would be unethical if CarerQoL of caregivers of thalassemic children (cases) would be compared with CarerQoL of caregivers of healthy children of the same age and sex (controls). Second, most of the data were self-reported by the caregivers of thalassemic children. Thus, there may be under or overreporting, and chances of social desirability bias cannot be overlooked. Third, in the present study, QoL of accompanying caregiver was assessed who may not be the principal caregiver in every instance as the QoL of a primary caregiver is likely to be affected the most. Fourth, as it was an institution-based study, the environmental condition of the study subjects (i.e., overcrowding) could not be assessed, which may be an essential determinant of their QoL. Finally, there may be specific other factors (i.e., caregiver’s health status, the total number of people they need to care for) influencing CarerQoL of the study participants, which we did not examine.
5. CONCLUSION
CarerQoL of the study participants were significantly associated with QoL of their wards. Other significant associates of CarerQoL were caregivers’ education level, financial profile, patients’ age, and their clinico-therapeutic profile. The various associates of CarerQoL found in the study should be further investigated by future studies in this regard to bring about a better understanding of the issue and plan more meticulous interventions to address it.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
BB conceptualized and conducted the study and wrote the manuscript. KB, NNN and AD helped in designing the study and reviewed the manuscript. BP and RB helped in statistical analysis and manuscript writing.
FUNDING
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ACKNOWLEDGMENTS
The authors would like to express their gratitude toward all the staff of thalassemia unit of Calcutta National Medical College who helped immensely during data collection.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
All participants voluntarily agreed to participate. The IECs of the All India Institute of Hygiene and Public Health and Calcutta National Medical College and Hospital, Kolkata, approved the study. The study was conducted as per Helsinki Declaration of 1975, as revised in 2000 (available at http://www.wma.net/e/policy/17-c_e.html).
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Bijit Biswas AU - Narendra Nath Naskar AU - Keya Basu AU - Aparajita Dasgupta AU - Rivu Basu AU - Bobby Paul PY - 2020 DA - 2020/02/11 TI - Care-Related Quality of Life of Caregivers of Beta-Thalassemia Major Children: An Epidemiological Study in Eastern India JO - Journal of Epidemiology and Global Health SP - 168 EP - 177 VL - 10 IS - 2 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.200102.003 DO - 10.2991/jegh.k.200102.003 ID - Biswas2020 ER -