
Investigating the Spatial Patterns of Common Childhood Morbidity in Six Neighboring West African Countries
- DOI
- 10.2991/jegh.k.191030.001How to use a DOI?
- Keywords
- Cough; diarrhea; fever; spatial analysis; West Africa
- Abstract
Children in developing countries have continued to suffer morbidity and mortality arising from a few illnesses. This study was designed to examine the within and between spatial variations in childhood morbidity from cough, fever, and diarrhea among six West African countries in a manner that transcends geographical boundaries. Data from six countries including their geographical boundaries were obtained from Demographic and Health Surveys. The spatial modelling was through Bayesian models and appropriate prior distributions were assigned to the different parameters of the model. Parameter estimation was through integrated nested Laplace approximation. Results show similar significant spatial distributions for the three illnesses, and they demonstrate that children in Benin Republic and Mali are less likely to suffer from these illnesses, whereas higher likelihood were obtained in the case of Cote d’Ivoire, Burkina Faso, Togo, and some parts of Ghana. The nonlinear effects of child’s age show that the risks of contracting the illnesses peak among children aged 10–14 months while, as the mothers advance in age, their children have reduced risks. Breastfeeding and a woman’s working status and education are among the significant factors that either aggravate or prevent these illnesses in the West African countries. The results pinpointed regions of the West African countries with high and low risks of the illnesses, and this would enhance intervention strategies of policy makers and international donors in the subregion.
- Copyright
- © 2019 Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
The world has been accelerating progress in reducing under-5 mortality rate. Sub-Saharan African countries also registered remarkable decline since year 2000, but this progress was insufficient to reach the Millennium Development Goal (MDG 4) target of a two-third reduction in under-5 mortality rate by year 2015, and is unlikely, in the present state, to attain the sustainable development goal target of a neonatal mortality rate of 12 deaths per 1000 live birth by 2030. West African countries have been identified as the major contributors to child mortality in sub-Saharan Africa, recording more than double the case recorded in southern or northern Africa [1,2]. Apart from malnutrition, leading causes of death among young children in Africa, like in most developing countries, have been identified to include preterm birth complications, malaria and non-malaria febrile, pneumonia, birth asphyxia, HIV/AIDS, and diarrhea [3,4].
Cough and breathing difficulty, usually caused by infectious agents including viruses and bacteria, are common issues faced by young children throughout Africa. Breastfed children with cough or cold may have difficulties in feeding; however, exclusive breastfeeding and adequate complimentary feeding are prescribed among the means of protecting against the occurrence [5]. Fever can also be caused by many infections and the proportion of fever attributed to malaria is usually high, ranging from 30% to 60% [6]. More than 60% of outpatient hospital visits in Nigeria, for instance, are a result of malaria/non-malaria febrile [7]. On the other hand, diarrhea, an infection–malnutrition link childhood disease, is described to be responsible for up to 80% of childhood growth retardation [8]. Both fever and diarrhea have been found to be inversely related to stunting and underweight among Malawian children [9].
It is evident that most diseases are spatially structured because individuals living in a geographical location are likely to behave in a similar manner that can either enhance or inhibit their well-being. Policy makers would therefore want to understand the geographical distributions of diseases rather than just the prevalence. Although most survey reports provide disease prevalence across different geographical locations, which could shed light on the spread across space, estimates from these reports may not be too reliable as they depend entirely on sample sizes taken from different locations and the effects of other contributory factors have not been accounted for. Model-based estimation of the distributions across space offers more reliable results as the procedures involve mechanisms that borrow strength from neighboring locations in the estimation process thereby yielding more reliable estimates [10].
There have been extensive discussions in the literature on the determinants and spatial distributions of childhood illnesses including fever, pneumonia, diarrhea, malaria, and anemia in most sub-Saharan African countries [4,5,11–13], and all the studies confirm the earlier submission of Kalipeni [14] that the geographic location where a child lives sets the context for child morbidity and mortality. However, all the studies cited above have been based on country-specific analysis. The distribution of the risk of anemia in preschool children after adjusting for nutritional status, parasitic infections, and other individual variables have been considered based on pooled data from three West African countries, namely: Burkina Faso, Mali, and Ghana [15]. The present study takes advantage of the geo-reference data provided by the Demographic and Health Surveys (DHS) to map the distribution of childhood illnesses in multiple West African countries. The DHS are nationally representative household surveys that employ stratified sampling procedures to collect accurate and representative data on population indicators, health, HIV, and nutrition particularly for women and children under 5 years, in most developing countries across the world at about 5 years interval. The survey utilizes mechanisms and procedures to ensure that the data collected are comparable across different geographical locations and over time [16]. Specifically, we investigate, in a manner that transcends geographical boundaries, the spatial distributions and determinants of fever, cough, and diarrhea in six neighboring West African countries, namely: Benin, Ghana, Togo, Ivory Coast, Burkina Faso, and Mali. We adopt structured additive regression analysis; an approach that allows to consider nonlinear effects of continuous variables, structured and unstructured random effects, and the usual linear effects in a single modelling framework [17]. With this methodology, we were able to discern not only the geographical distributions of the illnesses but also the detailed functional relationships between the diseases and continuous variables including child’s and mother’s age.
2. MATERIALS AND METHODS
2.1. Data
The study utilizes data from DHS conducted in the six West African countries between 2010 and 2014. The data utilized were from the most recent surveys conducted in each country as at the time of this study. The DHS Program has, over the years, provided technical assistance on surveys in several developing countries, thereby advancing global understanding of health and population trends. DHS has developed standard procedures, methodologies, and manuals to guide the survey processes and to ensure that the data not only properly reflect the situations they are intended to describe, but are also comparable across countries and over time. The primary sampling units are usually defined on the basis of enumeration areas from the Census frames of the country to be surveyed. DHS samples are usually selected using two- or three-stage stratified design. Information are collected from all women aged 15–49 years present at the selected households as well as on all children younger than 5 years of age. The data were retrieved for each country after approval had been given by the DHS Program.
West African countries included in the study and the years of survey are as follows: Benin (2011–2012), Burkina Faso (2010), Ivory Coast (2011–2012), Ghana (2014), Mali (2012–2013), and Togo (2013–2014). In the case of Mali, three regions, namely: Tombouctou, Gao, and Kidal, were not covered during the surveys and were therefore excluded. The choice of countries is for reasons that they share common boundary, which is a requirement for the spatial modelling technique; they have surveys conducted at relatively close periods; and they have comparable sample sizes. Although the surveys are usually conducted at about 5 years interval, the period in which they are conducted differ from country to country leading to time misalignment for the data set used for this study. We, however, considered the period between 2010 and 2014 over which the data were collected to be relatively short and thus assumed that period effect on the prevalence of the diseases would be minimal. On the basis of a careful review of similar studies conducted in Nigeria and Malawi [11–13], the demographic variables that were considered include mother’s age, child’s age, type of place of residence, child’s birth order and gender, mother’s educational attainment and working status, household wealth index, electricity in household, toilet facility, water source, exposure to media (newspaper, radio, and television; whether or not the mother was exposed to each of these at least once a week), and whether or not the child was being breastfed. The regions, being the spatial unit of analysis, were geo-referenced.
2.2. Statistical Analysis
Assume that yi is a binary random variable that indicates whether or not child i suffers from each of the diseases being considered (cough, fever, or diarrhea), and this is available for n number of children, that is i = 1, …, n. Then yi is said to have a binomial distribution with parameters pi, the probability of success, taken to be the proportion of children that suffer from an illness, and n, the number of children. Assume further that a set of explanatory variables denoted by x1, …, xk is available. To model the binary response variable conditional on the covariates, binary logistic regression with logit link function within the framework of generalized linear model is usually considered. The logistic model is given by (Equation (1))
The logistic model in Equation (1) is then extended to capture the different types of variables at once through the structured additive model defined as (Equation (2)):
Bayesian approach is the common approach of estimating parameters of the structured additive model, where the parameters and functions are considered to be random variables and prior distributions are assigned to them.
For the linear parameters, we considered independent diffuse priors that ensured the parameters are estimated similar to the classical linear regression approach. For the smooth functions, Bayesian versions of penalized-spline, commonly called p-spline, prior proposed by Lang and Brezger [19] was utilized. The prior enables the function to be estimated in a nonparametric form as a linear combination of basis function (B-spline):
The posterior distribution for model of this nature is intractable, consequently, inference in this study was based on Integrated Nested Laplace Approximations (INLA) as implemented in R-INLA, a packaged built within the R statistical package for approximating complex Bayesian models [21]. Further details on structured additive regression models and other different parameters that can be accommodated including the estimation procedure can be found in Fahrmeir et al. [18].
3. RESULTS
Table 1 presents the descriptive statistics of children included in the study and for those who suffered from each of cough, fever, and diarrhea. Overall, 12.7% (6912/54,200), 16.0% (8655/54,200), and 12.1% (6554/54,200) of children suffered from cough, fever, and diarrhea, respectively. The highest proportion of children who suffered from fever [33.6% (2909/8655)] and diarrhea [30.5% (2001/6554)] lived in Burkina Faso, but in the case of cough, Burkina Faso and Ivory Coast share about the same proportion [20.3% (1400/6912) and 20.4% (1411/6912)], respectively. Majority of the children who suffered from cough [64.5% (4456/6912)], fever [71.3% (6172/8655)], and diarrhea [71.7% (4699/6554)] lived in rural areas. Similarly, the majority of the children who suffered from each of the illnesses belong to mothers that had no formal education. Whereas majority of the children from households who sourced their water from protected sources suffered from the illnesses, the reverse is the case for households with toilet facilities where 60.1% (4156/6912), 67.2% (5815/8655), and 67.0% (4390/6554) had cough, fever, and diarrhea, respectively. Further, the proportion of children who suffered from each of the three illnesses is higher among those who lived in households with no electricity and those whose mothers were working at the time of the survey. As for birth order, 41.6% (2873/6912) of the children who were of fourth or higher order against 22.3% (1637/6912) of first birth order suffered from cough; 46.1% (3991/8655) of fourth or higher order against 19.4% (1681/8655) of first birth suffered from fever, whereas the highest proportion of children who suffered from diarrhea are of second or third birth order [45.7% (2995/6554)]. However, about equal proportion of male and female children suffered from cough [male: 50.3% (3478/6912), female: 49.7% (3434/6912)]; fever [male: 51.7% (4475/8655), female: 48.3% (4180/8655)], and diarrhea [male: 52.7% (3453/6554), female: 47.3% (3101/6554)].
| Variables | Total number of children (%) | Cough (%) | Fever (%) | Diarrhea |
|---|---|---|---|---|
| Place of residence | ||||
| Rural | 37,919 (70.0) | 4456 (64.5) | 6172 (71.3) | 4699 (71.7) |
| Urban | 16,281 (30.0) | 2456 (35.5) | 2483 (28.7) | 1855 (28.3) |
| Level of education | ||||
| No Education | 37,729 (69.6) | 4104 (59.4) | 5837 (67.4) | 4392 (67.0) |
| Primary | 9195 (17.0) | 1555 (22.5) | 1696 (19.6) | 1322 (20.2) |
| Secondary | 6714 (12.4) | 1142 (16.5) | 1040 (12.0) | 799 (12.2) |
| High school | 562 (1.0) | 111 (1.6) | 82 (1.0) | 41 (0.6) |
| Water source | ||||
| Not protected | 14,592 (26.9) | 1803 (26.1) | 2352 (27.2) | 1762 (26.9) |
| Protected | 39,608 (73.1) | 5109 (73.9) | 6303 (72.8) | 4792 (73.1) |
| Toilet facility | ||||
| Not improved | 35,821 (66.1) | 4156 (60.1) | 5815 (67.2) | 4390 (67.0) |
| Improved | 18,379 (33.9) | 2756 (39.9) | 2840 (32.8) | 2164 (33.0) |
| Electricity | ||||
| No | 37,833 (69.8) | 4277 (61.9) | 6128 (70.8) | 4619 (70.5) |
| Yes | 16,367 (30.2) | 2635 (38.1) | 2527 (29.2) | 1935 (29.5) |
| Access to mass media | ||||
| Newspaper | ||||
| No | 50,577 (93.3) | 6248 (90.4) | 8051 (93.0) | 6157 (93.9) |
| Yes | 3623 (6.7) | 664 (9.6) | 604 (7.0) | 397 (6.1) |
| Radio | ||||
| No | 19,819 (36.6) | 2592 (37.5) | 3160 (36.5) | 2597 (39.6) |
| Yes | 34,381 (63.4) | 4320 (62.5) | 5495 (63.5) | 3957 (60.4) |
| Television | ||||
| No | 32,428 (59.8) | 3713 (53.7) | 5203 (60.1) | 4004 (61.1) |
| Yes | 21,772 (40.2) | 3199 (46.3) | 3452 (39.9) | 2550 (38.9) |
| Mother’s working status | ||||
| Not working | 16,432 (30.3) | 1637 (23.7) | 1889 (21.8) | 1736 (26.5) |
| Working | 37,768 (69.7) | 5275 (76.3) | 6766 (78.2) | 4818 (73.5) |
| Birth order | ||||
| 1st Birth | 10,791 (19.9) | 1544 (22.3) | 1681 (19.4) | 1276 (19.5) |
| 2nd or 3rd Birth | 19,276 (35.6) | 2495 (36.1) | 2983 (34.5) | 2995 (45.7) |
| 4th or Higher birth | 24,133 (44.5) | 2873 (41.6) | 3991 (46.1) | 2283 (34.8) |
| Sex | ||||
| Male | 27,495 (50.7) | 3478 (50.3) | 4475 (51.7) | 3453 (52.7) |
| Female | 26,705 (49.3) | 3434 (49.7) | 4180 (48.3) | 3101 (47.3) |
| Breastfeeding | ||||
| No | 21,161 (39.0) | 2785 (40.3) | 3531 (40.8) | 2348 (35.8) |
| Yes | 33,039 (60.0) | 4127 (59.7) | 5124 (59.2) | 4206 (64.2) |
| Country | ||||
| Benin | 12,587 (23.2) | 979 (14.2) | 1132 (13.1) | 811 (12.4) |
| Burkina Faso | 13,449 (24.8) | 1400 (20.3) | 2909 (33.6) | 2001 (30.5) |
| Ivory Coast | 6811 (12.6) | 1411 (20.4) | 1611 (18.6) | 1231 (18.8) |
| Ghana | 5460 (10.1) | 729 (10.5) | 807 (9.3) | 657 (1.0) |
| Mali | 9557 (17.6) | 734 (10.6) | 807 (9.3) | 840 (12.8) |
| Togo | 6336 (11.7) | 1659 (24.0) | 1389 (16.1) | 1014 (15.5) |
| Total | 54,200 | 6912 | 8655 | 6554 |
Percentage distribution of children included in the study and for those who suffered for each of the illnesses
Results of the spatial effects for cough, fever, and diarrhea are presented in Figures 1–3, respectively. Part (a) of the figures presents the maps of posterior means, whereas part (b) shows the maps of the location of the 95% credible intervals used in deciding the significance of the posterior mean estimates. From the maps of credible intervals, regions in black (white) shading are places where the estimates for a particular illness are significantly lower (higher), whereas estimates for regions shaded in gray color are not significant. The results for the three illnesses show some interesting spatial patterns that affirm the presence of strong spatial structures that transcend geographical boundaries of the countries under consideration. The results show that children were less likely to have suffered from cough throughout Benin Republic and Mali, and in some regions of Burkina Faso, and the estimates are significant. However, in Togo, where all the regions share boundary with Benin Republic, findings show that children from the country have higher likelihood of suffering from cough. Further, except for Zanzan, Vallee du Bandama, and N’zi-Comoe regions of Ivory Coast, children from other parts of the country and those from the eastern region of Ghana have higher likelihood of suffering from cough.
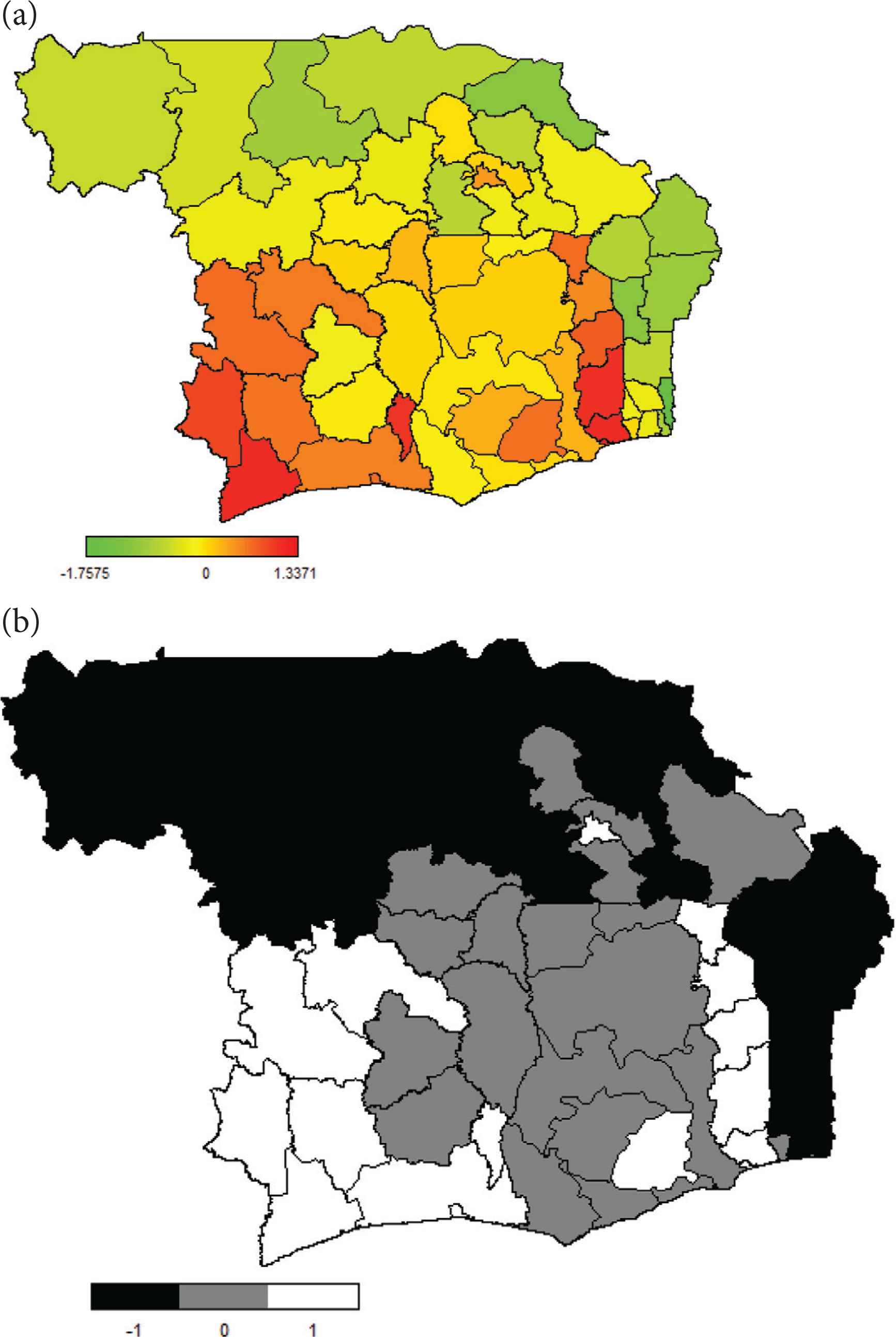
Estimated posterior mean spatial effects of cough (a) and the 95% credible interval (b).
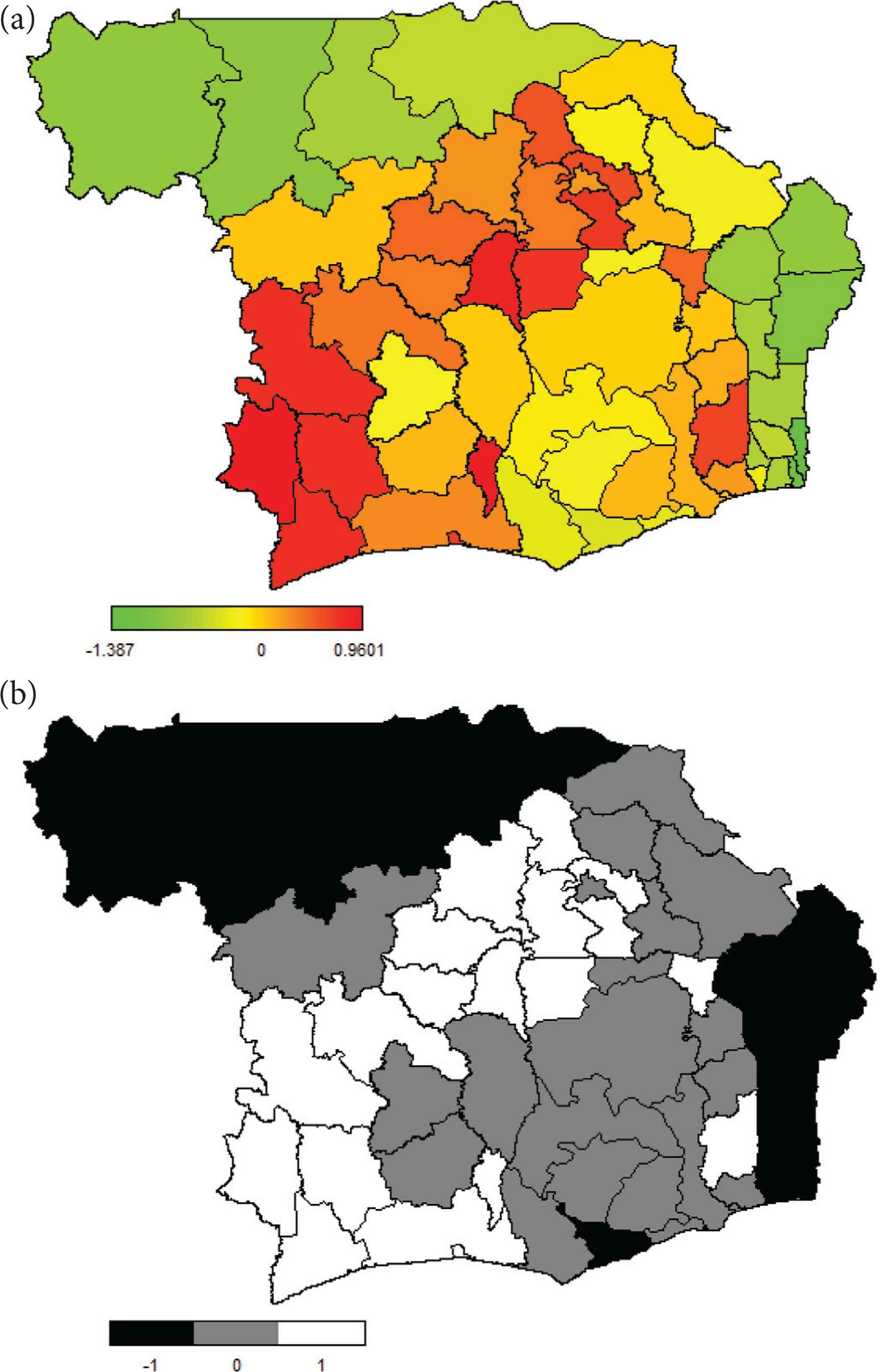
Estimated posterior mean spatial effects of fever (a) and the 95% credible interval (b).
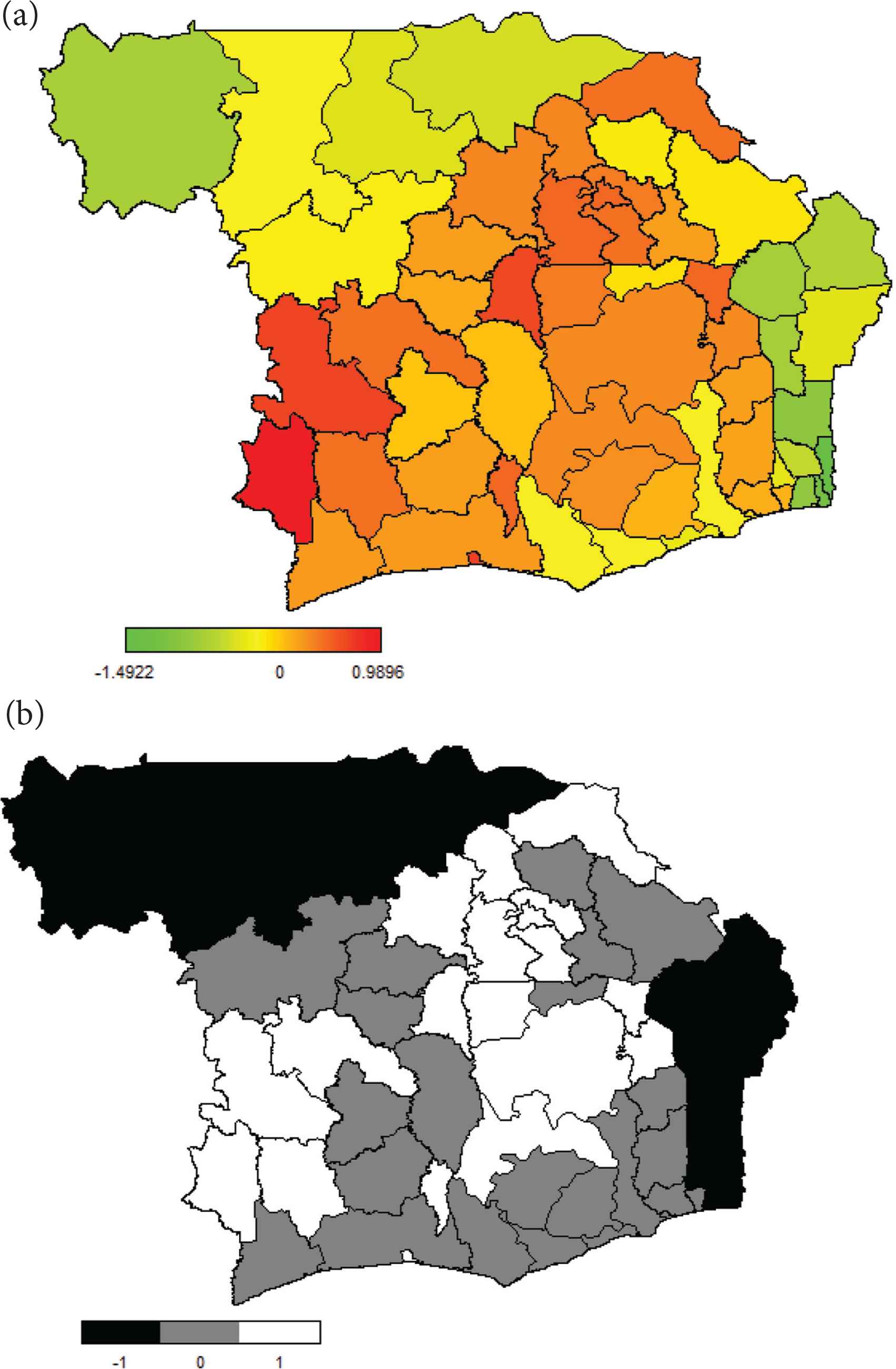
Estimated posterior mean spatial effects of diarrhea (a) and the 95% credible interval (b).
Results for fever show similar pattern as those for cough. Again, the likelihood of children suffering from fever was significantly lower among those residing in all the regions of Benin Republic, all but Sikasso regions of Mali, and in the Central region of Ghana. Places where higher likelihoods were obtained are: all regions of Ivory Coast except Zanzan, Vallee du Bandama, Sud-Comoe, and N’zi-Comoe; Cascade, Sud-Ouest, Hauts-Bassins, Centre_Ouest, Boucle du Mouhoun, Nord, Centre-Sud, and Plateau-Central regions of Burkina Faso; and Plateaux and Savanes regions of Togo. As for diarrhea, the pattern of spatial variations is again similar to those of cough and fever. Children from Benin Republic and Mali have less likelihood of suffering from the illness, whereas those from northern Ghana, eastern Ivory Coast, western Burkina Faso, and northern Togo have higher likelihoods.
Estimates for the nonlinear effects of child’s age and mother’s age for the three illnesses are presented in Figure 4a–f, which presents the posterior means (middle lines) and 95% credible intervals. Findings show identical patterns for all the three illnesses under consideration, for both mother’s and child’s ages. The results demonstrate an inverted ‘U’ relationships between child’s age and each of the three illnesses, signifying that the likelihood of suffering from any of cough, fever, or diarrhea in the West African countries increases as a child grows older to peak between ages 10 and 14 months from where it drastically drops as the child further advances in age. As for mother’s age, the results show that as a mother advances in age, the likelihood that her child would suffer from the illnesses reduces accordingly. The patterns are consistent for all the illnesses, just like for child’s age.
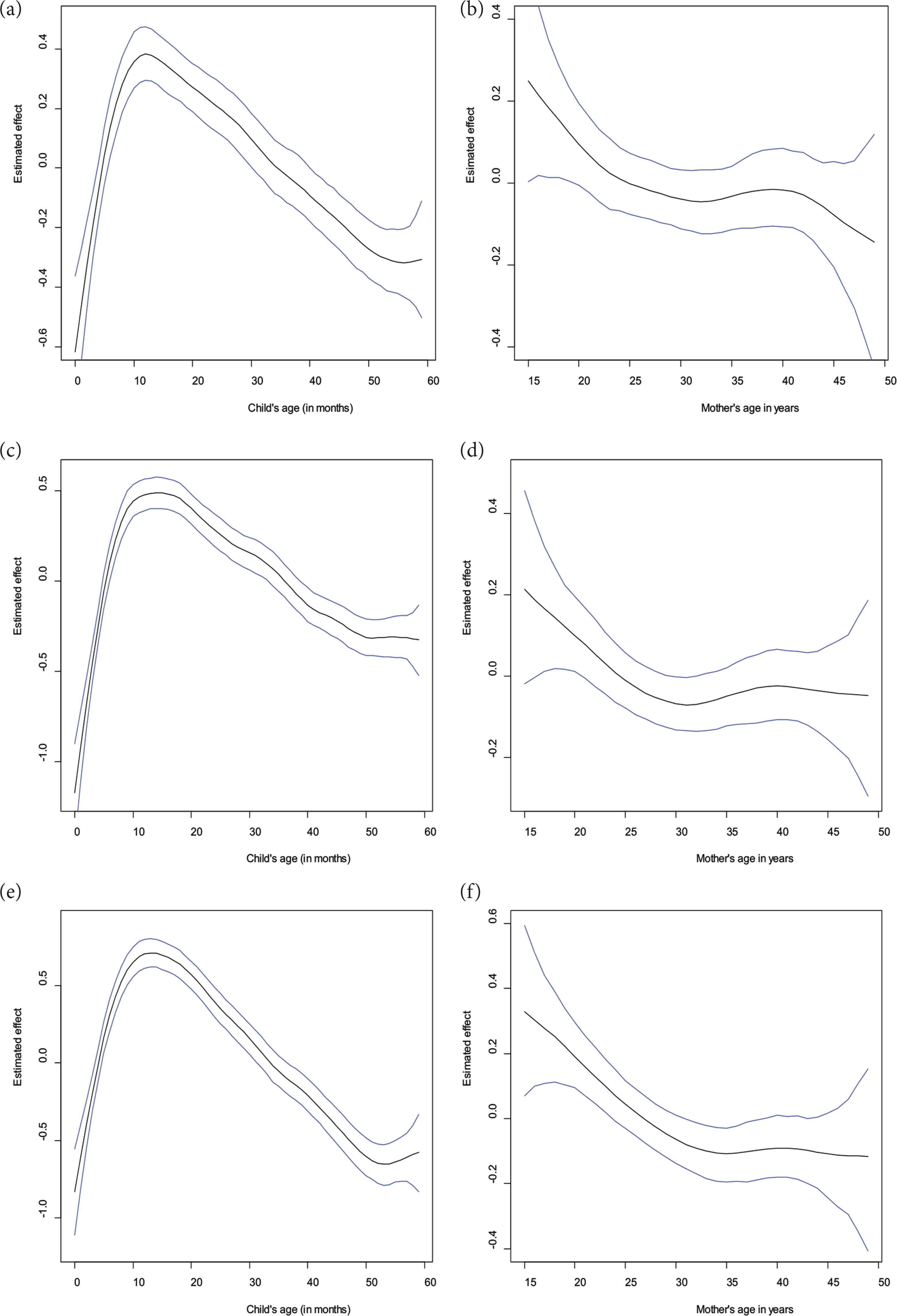
Nonlinear effects of child’s age and mother’s age for cough (a and b), fever (c and d), and diarrhea (e and f).
Findings for the categorical variables that were estimated as linear effects are presented in Table 2. The table shows the posterior odds ratio and 95% credible intervals for each illness. Findings reveal that when compared with rural areas, the odds that a child living in an urban area would have cough, fever, or diarrhea were not significant. Children whose mothers attained primary level of education have higher odds in the case of cough and diarrhea, whereas higher level of education translates to significantly lower odds for fever. The results show lower odds for fever in the case of children living in households with improved toilet facilities, whereas estimates for cough and diarrhea are not significant. Children whose mothers listen to radio at least once a week have lower odds of contracting diarrhea, but those whose mothers watch television have higher odds for fever and cough. Estimates based on electricity are not significant for any illness.
| Variables | Cough | Fever | Diarrhea | |||
|---|---|---|---|---|---|---|
| Odds ratio | 95% CI | Odds ratio | 95% CI | Odds ratio | 95% CI | |
| Place of residence | ||||||
| Rural | 1 | 1 | 1 | |||
| Urban | 1.009 | 0.910, 1.122 | 0.996 | 0.905, 1.097 | 0.984 | 0.889, 1.098 |
| Level of education | ||||||
| No Education | 1 | 1 | 1 | |||
| Primary | 1.112 | 1.008, 1.224 | 1.088 | 0.992, 1.195 | 1.214 | 1.091, 1.341 |
| Secondary | 1.062 | 0.931, 1.215 | 0.986 | 0.868, 1.122 | 1.097 | 0.961, 1.257 |
| High School | 0.877 | 0.618, 1.226 | 0.582 | 0.392, 0.866 | 0.632 | 0.389, 1.019 |
| Water source | ||||||
| Not protected | 1 | 1 | 1 | |||
| Protected | 0.966 | 0.887, 1.055 | 0.984 | 0.910, 1.062 | 0.965 | 0.886, 1.054 |
| Toilet facility | ||||||
| Non-improved | 1 | 1 | 1 | |||
| Improved | 1.001 | 0.904, 1.107 | 0.878 | 0.795, 0.962 | 0.952 | 0.849, 1.054 |
| Electricity | ||||||
| No | 1 | 1 | 1 | |||
| Yes | 0.961 | 0.858, 1.076 | 0.911 | 0.819, 1.013 | 0.900 | 0.799, 1.009 |
| Access to mass media | ||||||
| Newspaper | ||||||
| No | 1 | 1 | 1 | |||
| Yes | 1.088 | 0.939, 1.255 | 1.039 | 0.897, 1.191 | 0.911 | 0.763, 1.067 |
| Radio | ||||||
| No | 1 | 1 | 1 | |||
| Yes | 0.953 | 0.882, 1.037 | 1.042 | 0.972, 1.122 | 0.842 | 0.777, 0.913 |
| Television | ||||||
| No | 1 | 1 | 1 | |||
| Yes | 1.151 | 1.041, 1.267 | 1.100 | 1.005, 1.208 | 1.065 | 0.965, 1.176 |
| Mother’s working status | ||||||
| Not working | 1 | 1 | 1 | |||
| Working | 1.272 | 1.168, 1.377 | 1.358 | 1.257, 1.461 | 1.095 | 1.006, 1.191 |
| Birth order | ||||||
| 1st Birth | 1 | 1 | 1 | |||
| 2nd or 3rd Birth | 0.940 | 0.846, 1.045 | 1.010 | 0.916, 1.118 | 1.065 | 0.955, 1.190 |
| 4th or Higher birth | 0.971 | 0.854, 1.104 | 1.119 | 0.996, 1.260 | 1.212 | 1.063, 1.387 |
| Sex | ||||||
| Male | 1 | 1 | 1 | |||
| Female | 1.022 | 0.954, 1.096 | 0.950 | 0.891, 1.013 | 0.897 | 0.835, 0.963 |
| Breastfeeding | ||||||
| No | 1 | 1 | 1 | |||
| Yes | 0.889 | 0.818, 0.963 | 0.824 | 0.763, 0.889 | 0.858 | 0.785, 0.934 |
Posterior means and 95% Credible Intervals (CIs) for the fixed effects [Odds Ratio derived from estimates obtained from Equation (2)]
The working status of the mothers shows, surprisingly, that the children whose mothers were working had higher odds for the three illnesses compared with children of non-working mothers and the estimates are significant. Children of fourth or higher birth order were significantly more likely to suffer from diarrhea but the other estimates on birth order are not significant. Similar findings were obtained for gender, showing that female children were significantly less likely to contract diarrhea. As expected, for the three illnesses, children who were being currently breastfed have lower odds of contracting any of the illnesses.
4. DISCUSSION
This study adopts structured additive regression modelling technique to elucidate the spatial patterns and determinants of common childhood illnesses, pooling data from six neighboring West African countries. The results show that the illnesses, namely, cough, fever, and diarrhea, are spatially structured, displaying similar patterns across the countries under consideration. The reasons for the strong spatial structure of the illnesses are not revealed by this study; however, previous studies have postulated vast inequality in effective coverage of essential health interventions within the countries and poor sanitation, with widespread open defecation taking place in both rural and urban centers of most of the countries, to be the obvious causes of morbidity among children [22,23]. For instance, poor sanitation in Ghana has been driven by bad attitude and perception toward sanitation and extensive utilization of shared and public toilets; however, several recent reforms and programs have been put in place to ensure accelerated improvements in water and sanitation in every part of the country [24]. However, in Ivory Coast, although 91.5% of the urban population can access improved drinking water, improved sanitation is only available to 31.7% of the people and the country faced an increase in urbanization leading to informal and sprawling settlements, which further confound the sanitation conditions [25]. Similar alarming situation has been reported in the case of Mali but a community-led total sanitation program has helped to improve the situation in the country [26,27]. The identification of regions of the West African countries with high and low risks of the illnesses would enhance intervention strategies of policy makers and donors in the subregion, who are aiming at saving the lives of the young children.
Findings on child’s age conform to other studies in Africa and point to the influence of breastfeeding that younger children take from their mothers and thus, share directly from their mothers’ immunity [11–13]. Of particular interest here is the finding that shows high risks of the illnesses among children around aged 10–14 months. Early weaning and missed immunization have been found to increase the incidence of diarrhea and other childhood illnesses among children aged 1 year or younger [28–30]. Breast milk contains many immunological properties that protect against many infections. Children who are weaned early suffer from increased risks due to contamination from bottles or other objects used by the caregivers to nourish the young child [28,31,32]. More publicity that will encourage women to adhere to the WHO recommended 6 months of exclusive breastfeeding coupled with sustained and continued breastfeeding for longer periods thereafter would therefore provide more benefits to the children, more so that the results of the categorical variables from our analysis show that children receiving breast milk have lower risks of suffering from any of the illnesses. The observed low risks of the three illnesses among children of older women could be attributed to more experience on child care practices and disease prevention that would have come from previous births and child care [33–35]. The findings therefore strengthen the call for more attention to be given to younger women on child care and disease prevention strategies.
The findings on educational level of the mothers are expected as educated women would be able to adequately utilize their knowledge for the basic care of their households and to know how to take full advantage of available healthcare system for their benefits. They would also be able to express themselves clearly to health practitioners than a less educated woman would do. A previous study on Nigeria has shown that household structure and composition have significant effects on fever among young children, as evident from the findings on improved toilet facilities on fever in this study [4]. Whereas the results on television may be unexpected as messages on healthy lifestyle are disseminated through all available mass media throughout the countries, radio has more coverage than the other media because it is easily accessible to individuals in the interior areas and is easily carried along to places. The lack of significant effect of watching television could be due to the fact that more time is devoted to watching home videos and movies for pleasure than listening to messages on health issues that could benefit the entire household. When properly explored for message dissemination, radio can be more promising in reaching majority of the women, particularly the uneducated. Although one may expect that working women would have the resources to take good care of their children, these women often have less time for the welfare of their children including adequate breastfeeding because of the demands of their jobs. In most cases, the care of the young children is left in the hands of nannies or housemaids who may have little understanding of child care practices and thus, exposing the young children to high risks of diseases and malnutrition [36].
This study is not without some limitations. First, we were unable to make inference about causal effects for our findings due to the fact that our data come from cross-sectional survey. Second, the illnesses considered were obtained by asking the mothers to state if the child suffered from a symptom of each illness in the two weeks prior to the survey. Thus, the outcomes are subject to the ability of the mothers, some of whom are illiterate, to understand the symptom being described or their willingness to reveal the true state even when they understood. Thus, issues of underreporting cannot be ruled out. Further, the units used for spatial analysis in the study are the region of residence of the children, which are naturally composed of several smaller geographical dwelling units and thus, within region variations can be expected. A further analysis at more disaggregated smaller units could reveal local variations. It could have also been better if the data sets for all the countries were collected at the same time as this would remove all doubts about period effects, but this is not the case as these countries often depend on donor agencies to assist in conducting national surveys. Notwithstanding these limitations, the DHS data provide national coverage of the illnesses considered and are comparable across space and time thus remain the most viable option for studies of this nature.
5. CONCLUSION
The study on geographical variations in childhood morbidity in a region with adverse child health indicators is an effort in the right direction as it has pinpointed areas needing more attention among the West African countries considered. Governments of each country needs to consider identifying remote causes of high incidence of each of the illnesses in regions with higher likelihood of occurrence while at the same time, sustain the measures that results on the lower likelihoods in the other regions. Intensified health education on the benefits of sustained breastfeeding needs to be provided to all women while working-women should be encouraged to give more time to the care of their young children.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHOR CONTRIBUTIONS
E.G. and O.B.A. did study conceptualization. E.G., O.B.A., O.M.O. and P.O. wrote (original draft, review, and editing) the manuscript. E.G. performed data curation. E.G., P.O. and S.B.A. performed formal analysis. E.G., O.B.A., P.O. and S.B.A. contributed to the investigation. E.G., P.O. and S.B.A. contributed in methodology. E.G. and S.B.A. contributed to software. E.G. contributed in supervision.
ACKNOWLEDGMENT
The authors appreciate the DHS Program for granting access to the data analyzed.
Footnotes
Data availability statement: The data used for the study are freely available upon request at https://dhsprogram.com/.
REFERENCES
Cite this article
TY - JOUR AU - Ezra Gayawan AU - Olabimpe Bodunde Aladeniyi AU - Olubimpe Mercy Oladuti AU - Paul Olopha AU - Samson Babatunde Adebayo PY - 2019 DA - 2019/11/08 TI - Investigating the Spatial Patterns of Common Childhood Morbidity in Six Neighboring West African Countries JO - Journal of Epidemiology and Global Health SP - 315 EP - 323 VL - 9 IS - 4 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.191030.001 DO - 10.2991/jegh.k.191030.001 ID - Gayawan2019 ER -