
Prevalence of pulmonary tuberculosis among expatriates subjected to medical visa screening in Abu Dhabi, United Arab Emirates
- DOI
- 10.1016/j.jegh.2012.12.003How to use a DOI?
- Keywords
- Tuberculosis; Visa screening; Expatriates population; Prevalence
- Abstract
Introduction: All applicants for work and/or residence in Abu Dhabi are screened for tuberculosis at the time of issuing or renewing their residence visa. The purpose of this study is to assess the prevalence of TB among visa applicants and the likelihood of testing positive among different subgroups.
Methods: Data from the electronic visa screening system was used for a total of 948,504 applicants screened for residence in Abu Dhabi from January to December 2010.
Results: The screening identified 4577 suspected cases of pulmonary tuberculosis (PTB); 1558 people with chest X-ray findings suggestive of prior PTB; 235 smear-positives; and 132 culture-positive cases. The prevalence of active PTB was 39/100,000, with new applicants significantly more likely to test positive compared with renewals (OR: 2.05, 95% CI: 1.5–2.7, P < .001). People coming from African countries had the highest prevalence of TB compared with people from other regions (OR: 21.25, 95% CI: 6.72–67.17, P < .001).
Conclusion: The number of active PTB cases among applicants for visa screening is still of a real concern. Without a rigorous screening system, the disease can spread to the community and hit other people. Certain subgroups were more likely to have the disease; this could provide the scientific foundation for future amendments in the screening requirements.
- Copyright
- © 2012 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Tuberculosis (TB) is a global public health concern; where according to WHO estimates there are about 9 million new cases and 2 million deaths occurring annually worldwide [1]. Despite significant efforts and resources devoted to controlling TB, difficult challenges remain, mainly the alarming rise in multidrug-resistant TB (MDR-TB) and increasing mobility within and between countries [1–3].
The impact of immigrants’ health on the resident population was studied in a few countries, such as the United States and in Europe [4–6]. Epidemiologic studies using data from 2001 to 2006 in the US found that rates of TB among foreign-born persons are higher compared with the native-born population with 57% of all TB cases detected originating from the foreign-born persons. In addition, studies of TB genotypes suggest that, among foreign-born persons infected with TB, the infections were mostly reactivated latent ones, which were most likely acquired before arrival in the United States [7–9]. A study in Spain looked at the effect of emerging infections among immigrants over a 20-year period and found that latent TB was the most frequent type of infection [9,10]. The high rates of TB in developing countries continue to rise due to poor access to care and medical treatment, and this leads to chronic or latent disease that remains hidden for years [10].
According to the WHO TB report 2010, the incidence rate of TB in the United Arab Emirates (UAE) is 2.8 per 100,000 persons, which is considered relatively low [1]. Despite the fact that TB has a low incidence and prevalence rate in the UAE, TB control remains a challenge due to the high influx of the expatriate population, especially that the majority of them are coming from TB endemic areas. The population composition in Abu Dhabi consists of a majority of expatriates (4 of 5 residents are expatriates) [11].
This challenge enforced the establishment of a screening program for early detection and treatment of people applying for residence in the UAE. Around 1 million are screened for TB every year in Abu Dhabi.
Abu Dhabi is the capital of the UAE and has around 1.9 million residents [11]. Visa screening for expatriates is the most comprehensive screening program in the Emirate of Abu Dhabi, and it is a mandatory screening for all expatriates aged 18 years and above (newcomers and renewals). The Health Authority of Abu Dhabi (HAAD), which is the health regulator, has developed Visa Screening Standards with comprehensive guidelines on the screening and confirmatory testing of the targeted infectious diseases, including TB.
Active TB cases identified during the screening are referred to public hospitals for admission and treatment. Around five major hospitals provide special isolation and treatment for TB in Abu Dhabi. TB is also one of the reportable diseases in Abu Dhabi.
2. Methods
The study used HAAD electronic central database to perform secondary data analysis and assess the prevalence of TB among the expatriate population that applied for issuing or renewing their residence visa in Abu Dhabi from January to December 2010. This electronic visa screening system was established in June 2009 to monitor the screening process and control the issuance of fitness certificates. The method of this research was approved by the Institutional Review Board at Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland.
2.1. Measures
The electronic records for visa screening applicants extracted from the HAAD database for the year 2010 was examined. The records have multiple dimensions for patient information such as demographic information, including date of birth, gender, occupation, occupational categories, visa status, and type of visa the person is applying for. The system captures the coded investigation results including blood investigation for HIV, Hepatitis B, and syphilis, as well as chest X-ray readings [12]. If any of the results are positive, then a second set of investigations is required for confirmation. If the X-ray indicates suspicion of TB, the system requires that the film be reviewed by a second radiologist followed by a set of investigations according to the findings. The electronic system processes the information received to generate an outcome that defines the required next steps. If all investigations are normal, the fitness certificate is generated. The system has a verification step, where the data is rejected if not defined within the set of coding systems and an error message is generated. The second verification step is done by HAAD staff manually, with strict control measures, for cases with incomplete investigations or if additional investigations are done outside the screening centers in a secondary or tertiary care hospital. All of this information is added to the system and a new action is generated based on the additional medical reports.
2.2. Study subjects
The study population included all visa screening applicants from January to December 2010. It consisted of people who are 18 years old and above, as children below 18 are not subjected to medical screening for issuance of a residence visa. Table 1 shows the characteristics of the study subjects.
| Variable | All screened No. (%) | Smear positive No. (%) | Smear negative No. (%) | Old PTB No. (%) | Prevalence of TBd(per100,000) |
|---|---|---|---|---|---|
| Age years median [IQR]a | 33.3(21–53) | 31(27–54) | 32.3(25–50) | 40.6(31–62) | |
| Gender | |||||
| Female | 203,697(21.5) | 81(34.5) | 37(34) | 367(23.56) | 238.1 |
| Male | 744,807(78.5) | 154(65.5) | 95(71.97) | 1191(76.4) | 193.3 |
| Residence status | |||||
| New | 531,838(56.07) | 170(72.3) | 92(69.8) | 670(43) | 175.2e |
| Renew | 416,666(43.93) | 65(27. 7) | 40(30.3) | 888 (57) | 238.3 |
| Occupational oriesb | |||||
| Category A | 773,722(81.57) | 171(72.8) | 92(69.7) | 1239(79.5) | 194.1 |
| Category Bi | 134,243(14.15) | 53(22.6) | 31(23.5) | 237(15.2) | 239.1 |
| Category Bii | 40,539(4.27) | 11(4.68) | 9(6.8) | 82(5.2) | 251.6 |
| Nationality groupsc | |||||
| African | 34,884(3.68) | 21(8. 9) | 9(6.82) | 97(6.22) | 364.1 |
| Region of Americas | 9620(1.01) | 0 | 0 | 3(0.19) | 31.2 |
| South East Asia | 493,896 | 112(47.7) | 79(59.85) | 759(48.7) | 192.4 |
| European | 20,832(2.20) | 0 | 0 | 12(0.77) | 57.6 |
| Eastern Mediterranean | 310,594(32,75) | 44(18.7) | 21(15.91) | 489(31.39) | 178.4 |
| Western Pacific | 78,678(8.29) | 58(24.7) | 23(17.42) | 198(12.7) | 354.6 |
Inter-quartile range.
Category A: Office workers, ordinary workers, drivers, other professionals. Category Bi: Domestic workers including housemaids and private drivers. Category Bii: Food handlers, workers in restaurants and salons, workers in nurseries.
Nationalities were grouped according to WHO regions.
Prevalence of TB (total of old TB, smear positive TB, or smear negative TB) per 100,000 screened applicants of that subgroup.
After excluding old TB, new applicants had more than double the risk to have active TB (OR = 2.05, 95% CI: 1.5–2.7, P < .001).
Socio-demographic characteristics of visa screening applicants in Abu Dhabi, 2010.
2.3. Definitions
2.3.1. Residence status
- –
New: The subject is coming for the first time to issue a residence visa in Abu Dhabi.
- –
Renew: The subject is residing in Abu Dhabi and coming to renew their residence visa.
2.3.2. Nationality group
A total of 169 nationalities exist in the database and these were grouped into six regions according to the Member States of the six WHO Regional Offices (African Region, Region of the Americas, South East Asia Region, European Region, Eastern Mediterranean Region, and the Western Pacific Region).
2.3.3. Occupational category
The occupations in the visa screening application are grouped into three main categories; these categories have been defined based on how a given occupation would put served contacts at risk of infection.
- –
Category A: includes office workers, ordinary workers, drivers, other professionals.
- –
Category Bi: includes domestic workers like housemaids and private drivers (i.e. a driver that works with a family).
- –
Category Bii: includes food handlers, and workers in restaurants, salons, and nurseries.
2.3.4. Clinical definitions
- –
Suspected TB: is referring to all applicants who were found to have X-ray readings suggestive of old or active PTB and subjected to further review and/or investigation (irrespective of whether they were subsequently ruled out or confirmed as old or active TB).
- –
TB cases: in visa screening this applies to all of the following:
- a)
Old Pulmonary TB: cases with evidence of a fibrotic lesion consistent with old TB in the chest X-ray confirmed by at least two radiologists.
- b)
Active Pulmonary TB: cases with X-ray findings indicating suspicion of active TB that were confirmed when subjected to further investigations and assessment. According to the WHO definitions [1], such cases are further categorized as:
- a)
- –
Smear Positive PTB, where at least one out of three sputum specimens were found positive for AFB by microscopy.
- –
Smear Negative PTB, where all sputum specimens were found negative for AFB in microscopy but the applicant was found to have:
- ○
Culture positive result for Mycobacterium tuberculosis, OR
- ○
Radiological findings consistent with active PTB [12] and the patient is not responding to a course of broad-spectrum antibiotics; plus the decision of a physician to treat the patient with a full course of anti-tuberculosis treatment.
Cases with smear positive or smear negative active PTB require immediate admission and treatment with anti-tuberculosis medications.
2.3.5. Additional tests
- –
TST Positive: Tuberculin Skin Test (TST) is considered positive if the size of the induration was 15 mm or above.
- –
IGRA Positive: Interferon Gamma Release Assay (IGRA) is considered positive for a result with the following criteria (Nil ⩽8.0 IU/ml, TB antigen minus Nil is ⩾0.35 IU/ml and ⩾25% of Nil, with any Mitogen response).
- –
It should be noted that, screening for TB in the visa screening process starts with a chest X-ray, and only those with suggestive findings of TB are subjected to further testing, including TST and IGRA (i.e. TST and IGRA are used only to support the diagnosis of TB infection among people with positive X-ray findings).
3. Analysis
Data from HAAD visa screening electronic system was exported for secondary analysis after removing applicants’ identifiers, such as names. STATA IC version 11 [13] was used to perform descriptive statistics on the applicants’ demographic data and TB diagnosis (old TB, smear negative PTB, or smear positive PTB), and to compare across subgroups. Logistic regression was performed to examine the relationship between potential risk factors and the likelihood of having TB. The multivariate logistic regression model was used to analyze differences in TB prevalence by countries of origin (region). Adjustment was done for age, gender and occupational categories. In addition, simple and multiple logistic regression was done to examine the relationship between the smear-positive TB cases and the visa status (new vs. renew). Adjustments were made in the multiple logistic regression for age, gender, occupational categories, and nationality. The odds ratios with P-values <0.05 were considered statistically significant. The Hosmer–Lemeshow test was used to assess model fit.
4. Results
A total of 948,504 people applied for visa screening during the year 2010, of which 4577 applicants were suspected to have TB based on chest X-ray results. Fig. 1 shows the process of confirmation for a suspected TB case during visa screening.
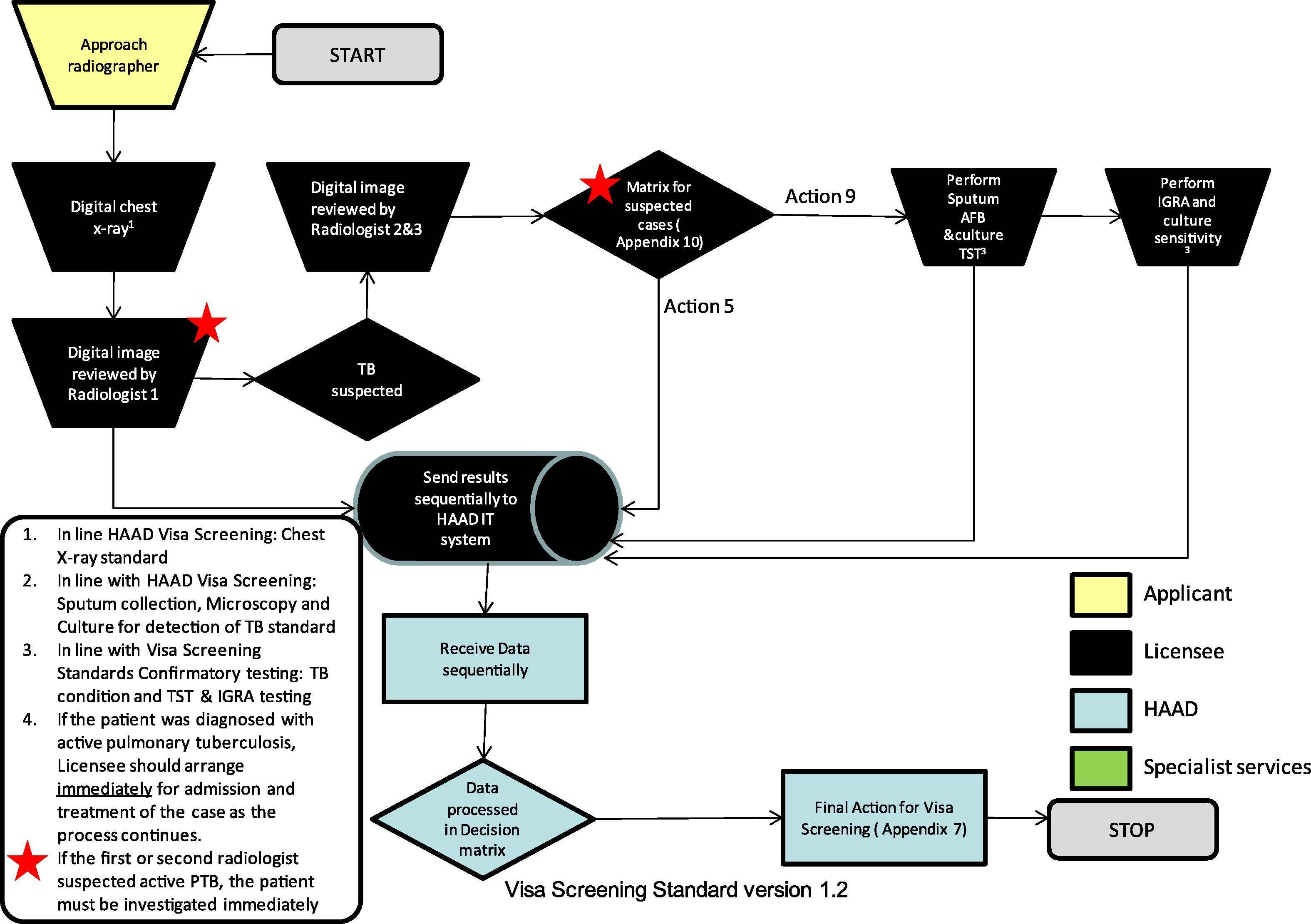
Process of confirmation for suspected TB cases in visa screening.
Fig. 2 summarizes the main findings of the TB screening among all applicants during the year of the study. Of all suspected cases, a total of 367 (8%) were found to have active TB (indicating a prevalence of 38.7 per 100,000 screened applicants), with 235 patients testing smear positive and 132 smear negative). In addition, 1558 (34%) of the suspected cases found to have old TB lesions in the chest X-ray, and with further testing found that 138 (9%) had a TB positive skin test and 221 (14%) had IGRA positive results.
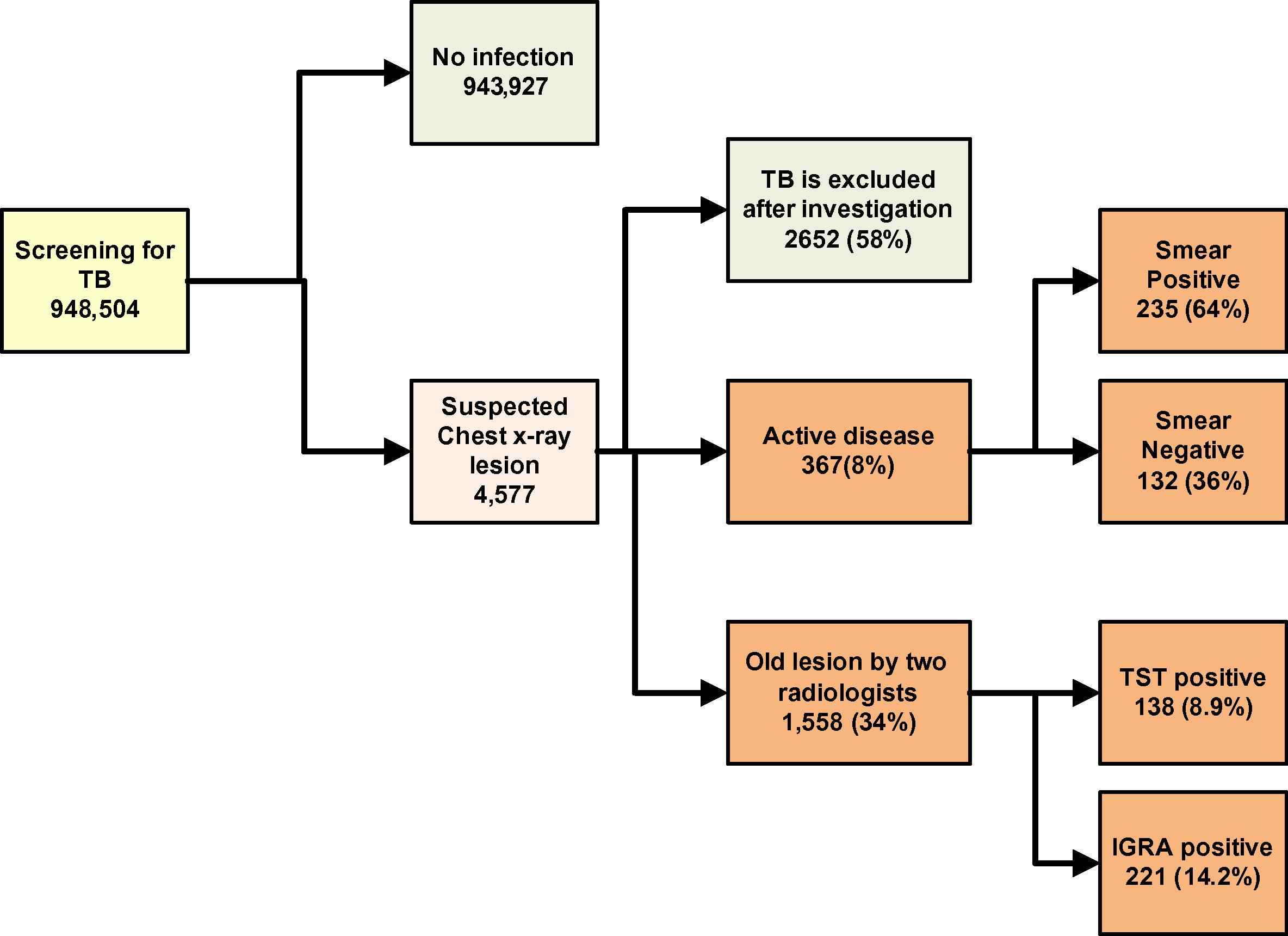
Results of screening for TB among the visa applicants in Abu Dhabi Emirate, 2010.
As shown in Table 1, the median age for smear-positive cases was around 31 years (95% CI: 27–54), which is relatively close to the median age of the screened population. In comparison, the median age for cases with old TB lesions was about 41 years (95% CI: 31–62).
Table 1 also shows the distribution of TB cases among different subgroups. Most of the smear-positive or smear-negative active TB cases were found among the new visa applicants (about 72% and 70% of the smear-positive and -negative cases, respectively).
The same table showed that the occupational group Category A consisted of the largest percentage of all detected TB cases (72% of the smear positive, 70% of the smear negative, and about 80% of old PTB cases). However, the prevalence of TB was the least among this group compared with the other two categories.
It has also been shown that applicants from South East Asia made up close to half of the smear positive and old TB cases, and about 60% of the smear negative cases (Table 1).
Performing simple logistic regression showed that the new visa screening applicants had more than double the risk of having active TB than renewals (OR = 2.05, 95% CI: 1.5–2.7, P < .001). The risk remained high and significant after adjustments for age, gender and occupation.
Table 2 shows that, with multivariate logistic regression, the risk of TB increased with age (OR increased by 1.05 for each 1 year increase in age; 95% CI: 1.05–1.059, P < 0.000). This association was adjusted for gender, occupational categories, and nationality groups.
| Factors | Odds ratiod | 95% Confidence interval | P value | Overall P value |
|---|---|---|---|---|
| Age | 1.056 | (1.05–1.059) | 0.0000 | |
| Gender | ||||
| Female | 0.93 | (0.816–1.06) | 0.286 | |
| Malec | 1.00 | |||
| Occupational categoriesa | 0.009 | |||
| Category Ac | 1.00 | |||
| Category Bi | 1.09 | (0.935–1.26) | 0.28 | |
| Category Bii | 1.39 | (1.11–1.72) | 0.003 | |
| Nationality groupsb | 1.00 | |||
| Americasc | (6.72–67.17) | 0.000 | 0.000 | |
| African | 21.25 | |||
| South East Asia | 8.97 | (2.88–27.93) | 0.000 | |
| European | 2.26 | (0.63–8.03) | 0.206 | |
| Eastern Mediterranean | 7.35 | (2.36–22.86) | 0.001 | |
| Western Pacific | 15.46 | (4.94–48.38) | 0.000 | |
Category A: Office workers, ordinary workers, drivers, others. Category Bi: Domestic workers including housemaids and private drivers. Category Bii: Food handlers, workers in restaurants and salons, workers in nurseries.
Nationalities were grouped according to WHO regions.
Reference category.
Adjusted for other variables in the table.
Socio-demographic factors and associations with TB diagnosis among visa screened applicants in Abu Dhabi, 2010.
Females were less likely to be screened as TB cases, i.e. with old or active PTB (OR = 0.93); however, this finding was not statistically significant (95% CI: 0.816–1.06).
Applicants from the African Region had the highest risk of being diagnosed with TB (old or active) compared with applicants from other regions and this difference was statistically highly significant (OR = 21.25; 95% CI: 6.72–67.17, P < 0.000). Applicants from the Western Pacific Region had the second highest risk of having TB (OR = 15.46; 95% CI: 4.94–48.38, P < 0.000).
The occupational Category Bii (i.e. food handlers, workers in restaurants, salons, or nurseries) showed a slightly increased risk of having TB as compared with other occupational categories (OR = 1.39, 95% CI: 1.11–1.72, P = 0.003).
The Hosmer–Lemeshow goodness-of-fit test showed that the logistic model fit the data adequately, (p = 0.07).
Fig. 3 summarizes the rate of TB per 100,000 nationality group and by results of TB screening.
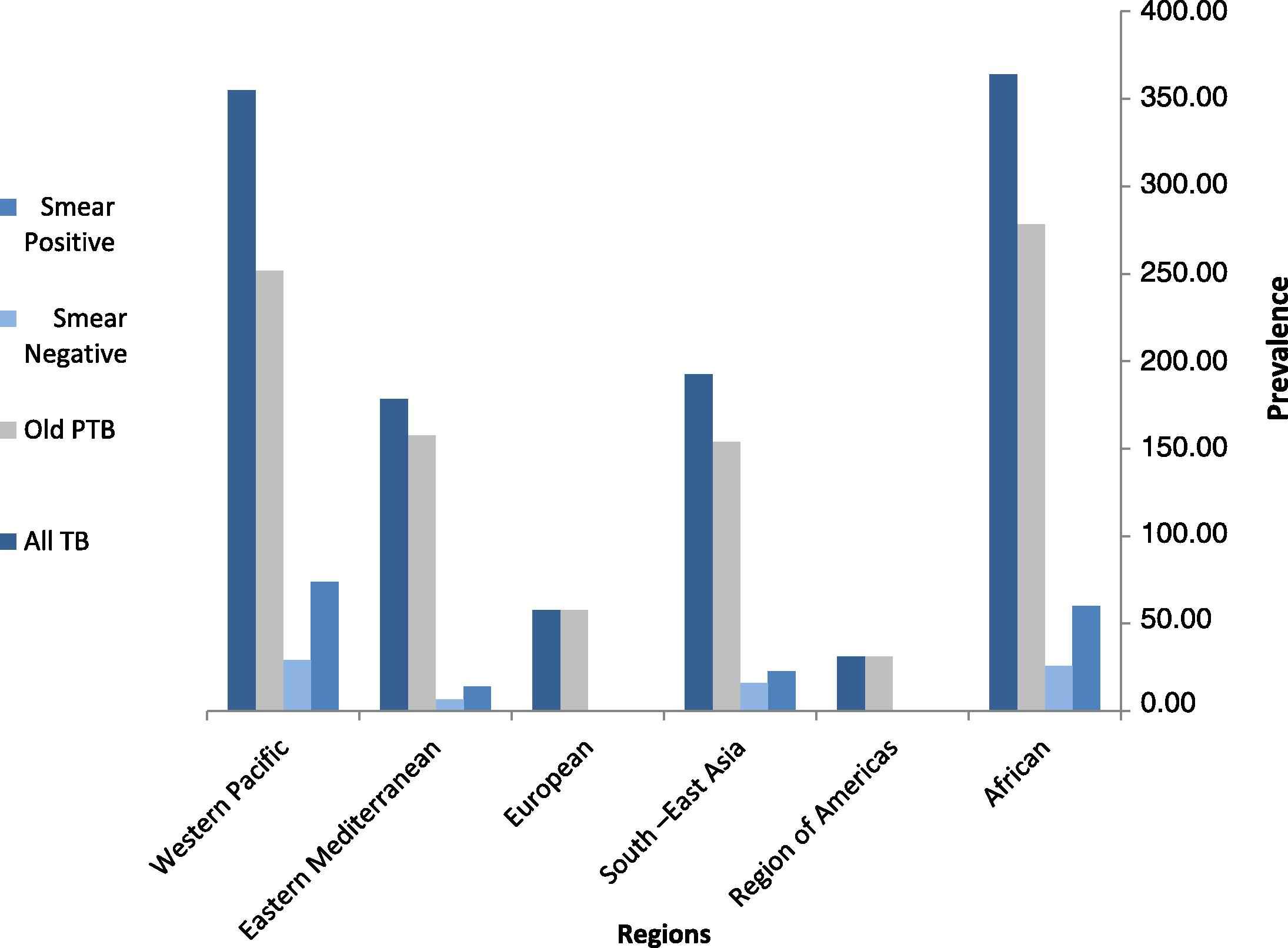
Prevalence of TB per 100,000 nationality group among visa screened applicants in Abu Dhabi, 2010.
5. Discussion
This is the first comprehensive study on the prevalence of TB among expatriates applying for residence visas in Abu Dhabi. The results of the study indicate that the prevalence of active TB among adult expatriates subjected to screening (about 39 per 100,000) is around 14-fold higher than the estimated prevalence of TB in the UAE. The prevalence of active TB was even more among the new applicants (49.3 per 100,000) compared with 25.2 per 100,000 among renewals (P < .001). New visa screening applicants were also more likely to be smear positive compared with renewals (OR: 2.05, 95% CI: 1.5–2.7). This finding is consistent with previous studies in the States that showed higher rates of TB among immigrants [7,14]. This emphasizes the importance of having efficient screening for expatriates coming to reside in Abu Dhabi for early detection and management of TB, as this would help combat the illness and prevent its spread in the community. The findings also support the importance of having a home screening program for newcomers to Abu Dhabi, which will help decrease the numbers of active TB cases among the newcomers to the UAE. This study showed that in the year 2010 alone, a total of 367 people (about 8% of all suspected cases) were found to have active TB disease among all applicants for residence visas. Additionally, it showed that 1558 applicants presented with old TB lesions in the chest X-rays (34% of suspected cases), of whom 14% were IGRA positive and 9% were TST positive. These findings again highlight the importance of early detection and management of TB cases and the importance of follow-up and treatment of people with latent TB infections; especially since many of the applicants are coming from countries where the management of TB is not optimal.
While the median age of smear-positive TB cases was close to that of the whole screened population (31 vs. 33 years), applicants with evidence of old PTB were of older ages (a median of about 41 years old). This finding is not unexpected given the age distribution of the disease [9]. Moreover, the likelihood of having TB among the study population increases with age (OR = 1.05 for each 1 year increase of age; 95% CI: 1.05–1.059, P = 0.000). This finding was also biologically plausible, as the older the age of applicants, the more likely they have had TB infection at some point of their lifespan, with more risk of reactivation as they get older and have lowered immunity.
It was very interesting to find that the likelihood of having TB was highly related to the region where the applicant came from (compared with the Region of the Americas as the reference category, people coming from the African Region were more than 21-fold more likely to have TB, and this was highly statistically significant). Applicants from the Western Pacific and South East regions had the second and third highest risks, respectively. The association was highly significant across all groups except for the European Region in which the apparent increase in risk was lacking statistical significance. These findings came in line with the WHO report 2010 [1] that showed most of the TB cases were from the regions of South East Asia (35%), Africa (30%), and the Western Pacific (20%).
The study also found that the occupational Category Bii had the highest risk of having TB. Given that the Bii group includes people working in nurseries, this finding might pose a special risk to the children they are taking care of, especially that newcomers to the UAE have 60 days to complete their visa issuance. This risk should therefore be further assessed and considered in visa and medical screening regulations.
The research findings recommend replication of the study where consistency of the results can provide the scientific foundation for any future amendments in the visa screening requirements.
The study did not examine the prevalence of antimicrobial-resistant TB strains, such as multi-drug resistant (MDR), among the screened population. The electronic data used did not include information about resistant strains. It is therefore recommended that this important aspect be assessed in future studies.
6. Conclusion
The number of active PTB cases among applicants for visa screening is still of a real concern. Without a rigorous screening system, the disease can spread to the community and hit other people. Certain subgroups were more likely to have the disease, with an increased risk among newcomers compared with renewals. The findings highlight the importance of having strict measures to control TB in Abu Dhabi, and points to the important role home screening can play in decreasing TB among newcomers.
Conflict of interest
None declared.
Acknowledgements
We would like to acknowledge Johns Hopkins Bloomberg School of Public Health for reviewing and approving the study protocol, and special thanks to Professor David D. Celentano (ScD MHS, Chair of the Department of Epidemiology), and Professor James Tonascia (PHD, Department of Epidemiology and Biostatistics) for their thorough review and comments.
References
Cite this article
TY - JOUR AU - Farida I. Al Hosani AU - Ghada A. Yahia PY - 2013 DA - 2013/02/01 TI - Prevalence of pulmonary tuberculosis among expatriates subjected to medical visa screening in Abu Dhabi, United Arab Emirates JO - Journal of Epidemiology and Global Health SP - 23 EP - 30 VL - 3 IS - 1 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2012.12.003 DO - 10.1016/j.jegh.2012.12.003 ID - AlHosani2013 ER -