
Occurrence of acute respiratory infection, diarrhea and jaundice among Afghan pilgrims, 2010
Tel.: 0093799607107.
Tel.: 0093798036038.
Tel.: 0093700615156.
- DOI
- 10.1016/j.jegh.2012.11.003How to use a DOI?
- Keywords
- Mass Gathering; ARI; Diarrhea; Hajj; Afghanistan
- Abstract
Background: Annually 30,000 Afghans attend the Hajj in Saudi Arabia that is one of the largest mass gathering events in the world. We aimed to determine the prevalence of three syndromes of interest diarrhea, acute respiratory infections (ARI) and jaundice-among Hajjis gathering at the four transit sites in Afghanistan before, during, and after their voyage.
Methods: A total of 1659 Hajjis at four transit sites were selected and included a cross-sectional study. Information was collected prior Hajjis departure and upon their return from Saudi Arabia regarding demographics and experience of diarrhea, ARI and jaundice. Standardized case definitions were used for the three health outcomes of interest.
Results: The occurrence of diarrhea and jaundice remained constant over time. However, ARI increased from 1.4% at pre-transit to 4% at transit area and 37% during the Hajj. ARI rates among residents from the Central and Northern regions of Afghanistan were significantly higher at the post-Hajj stage, at 50% and 69%, respectively. There was no difference in ARI by sex among Hajjis.
Conclusions: There is a need to review the quality and effectiveness of the flu vaccine. Authorities should come up with the sound strategies to overcome ARI problems during Hajj.
- Copyright
- © 2012 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)
1. Introduction
Each year in the 12th month of the Islamic calendar (Dhul-Hijjah) Muslims from around the world begin observing activities associated with the annual Hajj, or pilgrimage to Mecca. Hajj is the largest annual Islamic mass gathering in the world with almost 3 million pilgrims known as “Hajjis” attending the event [1]. Being one of the enormous mass gatherings of its kind, the Hajj pilgrimage has its own health challenges. Pilgrims (Hajjis) coming from various parts of the globe represent diverse socio-demographic characteristics and health backgrounds. These factors could be suggestive of posing various health risks to pilgrims and even making them prone to especially communicable diseases, injuries and loss of hundreds of lives [2–4] while attending such a massive event.
Those health risks, particularly infectious diseases, could give rise to diseases such as; meningococcal meningitis, respiratory tract infections, and blood-borne diseases [5]. More importantly, outbreaks of infectious diseases, particularly acute respiratory tract infections (ARI), diarrheal diseases, and meningococcal meningitis, have been frequently reported among Hajjis [6]. Given that the average journey ranges between 30 and 45 days, most pilgrims will most likely be exposed to contracting various health problems. Such stay consists of around 6 days in Jeddah as their entry point to Saudi Arabia preparing for the arranged activities, then around 10 days to perform special prayers in the city of Medina, and almost 8 days in Mecca for performing the key tasks, and, finally, the rest period for preparing to return to their initial destination. That is common for Afghan Hajjis, which is not compulsory for all.
According to a survey completed in France addressing the Hajj associated problems, cough was the main complaint significantly high in individuals >55 years with the attack rate of 51%, and followed by headache, heat stress, and fever. Added to that, some travelers reported suffering from diarrhea and vomiting [7]. In 2006 in another study report published in Marseille, France, the attack rate for ARI was recorded to be up to 60% in cohorts of returned Hajj pilgrims [8]. As reported directly by the pilgrims, the main sources of contamination for ARI involved: sneezing and coughing (58.1%), dirty hands (43.9%), contact with ill persons (40.5%), saliva (17.2%), promiscuity (17.0%), food (12.1%), drink (9.1%), air conditioning (3.4%), and contact with animals (0.4%) [9].
Additionally, one of the other common types of infectious diseases challenging the well-being of the pilgrims was diarrhea [10]. The result of a laboratory study of stool samples in Saudi Arabia revealed that most of the enteric virus infections causing diarrheal diseases occurred following the occurrence of the Hajj season and rotaviruses were significantly more common in non-Saudis than in Saudi citizens [11]. The source also speculated a likely relationship among the occurrence of hepatitis and travel, specifically among Hajjis undertaking a long and challenging journey. During this congregation, pilgrims stay under the tents shared by a large number of people often living on foods from street vendors and sharing common toilet facilities that can expose them to both hepatitis A and E. These circumstances are suggestive of the notion that pilgrims would be at high risk of developing hepatitis B or C, particularly due to undertaking certain activities, such as head shaving or trimming by fellow pilgrims or street barbers, who often re-use their razor. Hajjis could also get exposed to hepatitis B or C due to getting injured on their hands and possibly feet while sacrificing cattle and walking barefooted [12]. As per these reports supported by anecdotal evidences, a considerable number of Hajjis returning from Hajj report one or more cases of communicable diseases, such as respiratory, diarrheal and other types of infectious diseases.
Although no studies provide data on Hajj problems in Afghanistan, as anecdotally reported, the health concerns as mentioned earlier concern the Afghan public health authorities as this has the potential to pose serious effects on the health of an average of 30,000 Afghan Hajjis and their dependent families. To embark on this and assess the prevalence of ARI, diarrheal disease, and jaundice as a proxy for hepatitis among Afghan Hajjis, a cross-sectional study was conducted capturing data at three points of time: before arrival to the transit areas (departing airports), at the transit area and again upon arrival back from Hajj. Data from this study are also intended to guide the development of prevention guidelines by the Ministry of Public Health (MoPH) to provide a more responsive healthcare to the Afghan Hajjis.
2. Methods and materials
A cross-sectional study was conducted to collect data on three health problems: acute respiratory tract infection (ARI), diarrheal diseases (DD) and jaundice (as a proxy for viral hepatitis). The study was carried out at four points where the Afghan Hajj pilgrims gathered coming from four regions of the country and prepared to travel to Saudi Arabia. These points, called transit areas, are located in certain geographical locations of the country, namely: Kandahar, Balkh, Hirat and Kabul, serving residents of the South, North, West and Central regions of the country, respectively. The transit areas were located next to the airports with poor facilities where there is only one large waiting hall prior to departure. Previously, Hajjis waited for 24–48 h in transit areas, but during this study, the waiting time was decreased to 6–12 h due to slightly better arrangements in place. The target population for this survey was Afghan Hajjis who had completed their paperwork and were ready to travel to Saudi Arabia for Hajj Pilgrimage by November 2010.
Eligible participants included in the study were all pilgrims, including men and women, who were in transit areas carrying ID numbers issued by the Ministry of Religious Affairs, and those ready to travel to Saudi Arabia. Subjects were selected systematically using either the lists provided by the Ministry of Religious Affairs (e.g., every 20th Hajji on the list) or seats of the bus booked for each traveler arriving at the transit area (e.g., seats 3, 12 and 27 on each arriving bus).
Subjects’ age, sex, education level, residential areas and occupation were collected in addition to self-reported symptoms of ARI, DD and jaundice during three time periods being: at home during the 2 weeks prior to departure, at the time of the interview in the transit areas, and during Hajj through returning home. These diseases were addressed due to being highly prevalent compared with other health problems as per the surveillance data generated by the Afghan Ministry of Public Health on the general population in the country [13]. A structured questionnaire was developed and administered by experienced surveillance officers during two interviews: the first was conducted in-person at the transit area and ascertained the health status during the 2 weeks prior to arrival at the transit area. The second interview was conducted by phone 1–2 weeks following the return of pilgrims from Hajj. The same questionnaire was used to collect data on three periods. Fig. 1 shows the continuum for data collection.
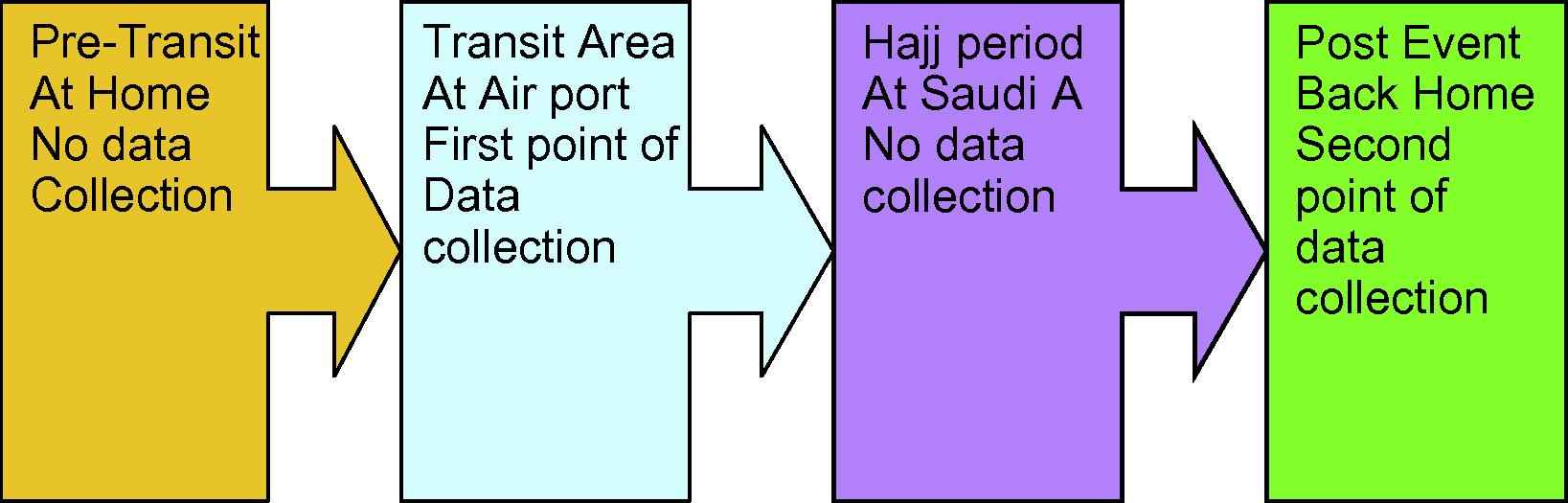
Continuum of data collection at different points.
All case definitions were based on self-reported symptoms recorded during the interview with Hajjis at the time of staying in Afghanistan and the two-week period while preparing for the overseas travel, followed by the second interview after returning from Saudi Arabia. Additionally, surveillance case definition was also used for this study. Explicitly, a case of ARI was defined as an illness characterized by the existence of cough, fever and a sore throat. A case of diarrhea was defined by more than three smooth and watery defecations in a 24-h period. Jaundice was defined by the appearance of yellowness in the sclera or skin.
The goal of interviewing 422 attendees from each transit site was determined given that: attendees from these four sites were not necessarily homogenous; data showing the prevalence of ARI, DD and jaundice among Hajj pilgrims were unavailable; and taking into consideration an assumed maximum prevalence of 50%, margin of error 0.05, confidence level of 95% as well as adding a 10% non-response rate. The actual numbers interviewed varied based on flight schedules of each transit area, and the interviews were conducted during the month of October and the first week of November 2010.
Following this, the proposal was submitted to the Institution Review Board (IRB) at the Ministry of Public Health, and provisional approval was obtained. Subsequently, the verbal informed consent was received from the study participants prior to an interview taking place. Lastly, data were entered into the Access system and consequently analyzed using the SPSS version 18, and tests such as the Student’s t-test, chi-square, and Cochran’s test were the main statistical tests used in this study.
3. Results
The prevalence study was designed in a Mass Gathering workshop conducted by EMPHNET (Eastern Mediterranean Region Public Health Training Network) and the CDC in Jordan in October 2010. The study was then implemented in Afghanistan before Hajj rituals started. There were 1659 Afghan pilgrims who were interviewed, including 426 for the south transit area, 425 for the west, 393 for the north, and 415 for the central. The mean age of subjects was 45 (SD 12), with a range of 9–85 years; roughly 75% of participants were between 31 and 60 years of age. The majority of subjects (88%) were males with land farming and shop keeping being the most frequently reported occupations. Over half of the total study participants were illiterate or had no formal education (Table 1).
| Characteristics | North | Central | West | South | National |
|---|---|---|---|---|---|
| Occupation | |||||
| Shopkeeper | 85(5.2) | 63(3.9) | 92(5.60 | 74(4.5) | 314(19.2) |
| Farmer | 88(5.4) | 29(1.8) | 69(4.2) | 120(7.3) | 306(18.7) |
| Housewife | 46(2.8) | 26(1.6) | 60(3.7) | 46(2.8) | 178(10.9) |
| Jobless | 29(1.8) | 18(1.1) | 65(4) | 46(2.8) | 158(9.7) |
| Business | 5(0.3) | 98(6) | 22(1.3) | 16(1) | 141(8.6) |
| Gov. employee | 10(0.6) | 52(3.2) | 21(1.3) | 3(0.2) | 86(5.3) |
| Teacher | 17(1) | 32(2) | 33(2) | 11(0.7) | 93(5.7) |
| Others | 113(6.9) | 83(5.1) | 63(3.9) | 100(6.1) | 359(22) |
| Age groups | |||||
| <20 | 7(0.4) | 6(0.4) | 6(0.4) | 1(0.1) | 20(1.2) |
| 20–30 | 35(2.1) | 44(2.7) | 55(3.3) | 46(2.8) | 180(10.9) |
| 31–40 | 79(4.8) | 127(7.7) | 110(6.6) | 110(6.6) | 426(25.7) |
| 41–50 | 102(6.2) | 98(5.9) | 124(7.5) | 119(7.2) | 443(26.8) |
| 51–60 | 112(6.8) | 97(5.9) | 110(6.6) | 108(6.5) | 427(25.8) |
| 61–70 | 55(3.3) | 35(2.1) | 20(1.2) | 36(2.2) | 146(8.8) |
| >70 | 3(0.2) | 6(0.4) | 0 | 6(0.4) | 15(0.9) |
| Sex | |||||
| Male | 343(20.7) | 388(23.4) | 359(21.7) | 378(22.8) | 1468(88.6) |
| Female | 49(3) | 26(1.6) | 66(4) | 48(2.9) | 189(11.4) |
| Level of education | |||||
| Illiterate/no education | 203(12.3) | 142(8.6) | 214(12.9) | 345(20.8) | 904(54.5) |
| Primary school | 92(5.6) | 79(4.8) | 75(4.5) | 41(2.5) | 287(17.3) |
| Secondary School | 51(3.1) | 89(5.4) | 80(4.8) | 33(2) | 253(12.3) |
| Higher education | 47(2.8) | 103(6.2) | 56(3.4) | 7(0.4) | 213(12.8) |
Demographic Characteristics of Afghan pilgrims.
Overall, the second interview was conducted with 1529 (92%) subjects. There was a particularly prominent loss with regard to following up with those Hajjis from the northern region. Of the 393 Hajjis from the north who were interviewed at the transit area, follow-up interviews by telephone with only 287 (73%) of them were conducted.
A significant increase in ARI was recorded, rising from 1.8% (CI 1.3–2.6) during pre-transit to 4% (CI 3.2–5.1) at the transit area, and 37% (CI 34–39) during Hajj (P value < 0.001). Compared with the South region, the prevalence of ARI during the Hajj was the highest among participants from the central and the north regions (P value < 0.001 for each). The prevalence of ARI among males and females Fig. 2 was almost the same: 38.3% and 33.5%, respectively (P value = 0.238). There was no significant association between ARI and the occupation of the participants. The number of pilgrims who complained of jaundice was significantly reduced during Hajj (P value = 0.008). No significant change was observed in the prevalence of diarrhea in pre-transit, transit and the Hajj period at the national level (P value = 0.862) (Table 2).
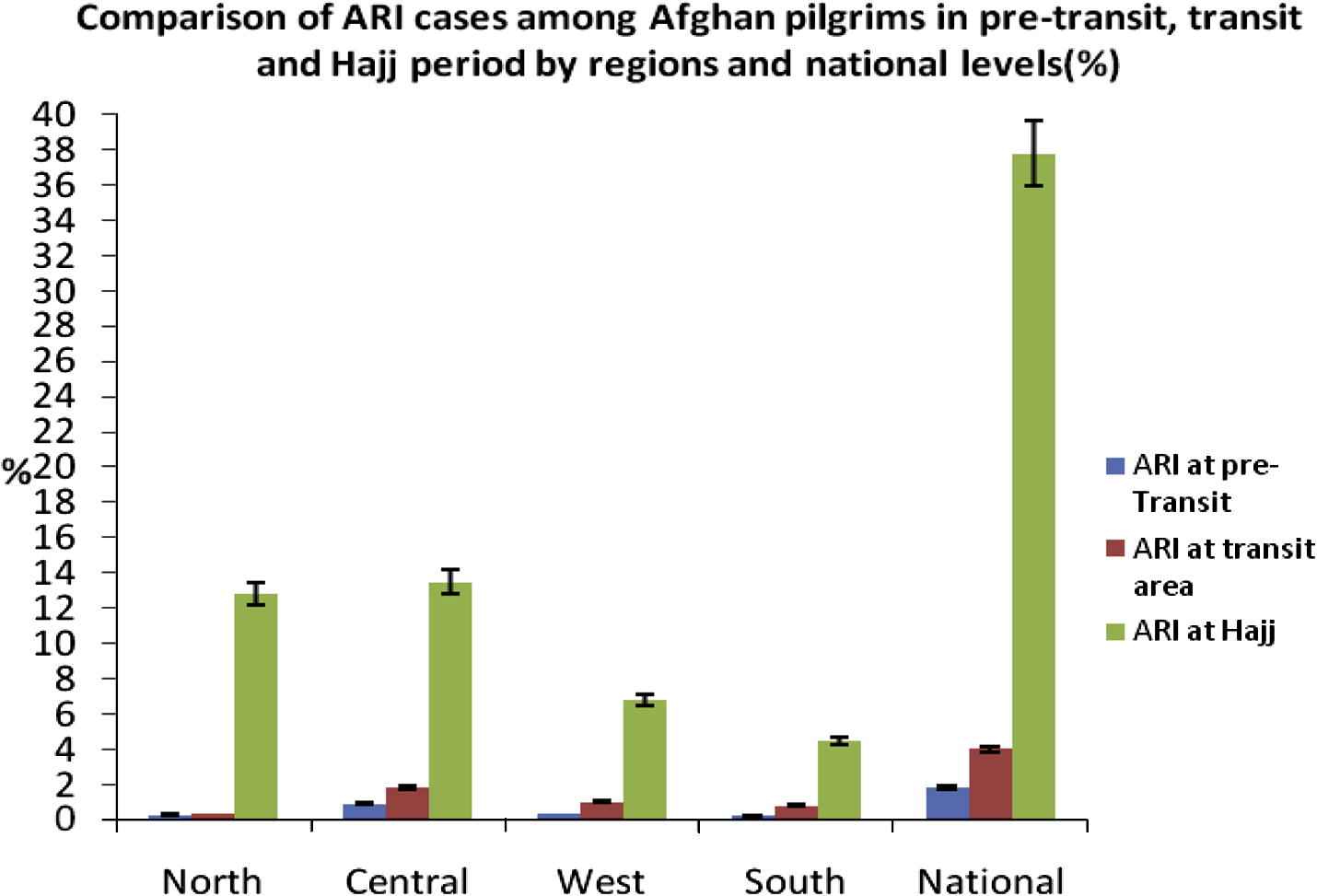
Comparison of ARI cases among Afghan pilgrims in three different periods.
| Variables | Transit (N = 1657) | Hajj (N = 1523) | P value |
|---|---|---|---|
| Duration of pilgrims’ stay | 12–24 h | 30–45 days | |
| Jaundice N (%) | 2 (0.2) | 3 (0.2) | 0.008 |
| Diarrhea N (%) | 20 (1.2) | 18 (1.1) | 0.862 |
| ARI N (%) | 67 (4) | 576 (37.8) | 0.000 |
Prevalence of ARI, Diarrhea and jaundice among Afghan pilgrims.
4. Discussion
The study found a significant increase in ARI prevalence during Hajj with cases reporting as much as 69% of Hajjis from northern areas and 50% from central areas of the country being affected. Generally, ARI increased from 1.8% during pre-transit to 4% at the transit area and 37% during Hajj. These figures refer to a mass of approximately 15,000 Afghan Hajjis affected by ARI, which shows a significant public health concern. Additionally, this indicates that ARI is one of the commonly occurring incidences that can also lead to an outbreak during the Hajj event and as well upon the arrival of local pilgrims back home. Additionally, even the ARI has increased the rate of hospital admission during Hajj season in the host country hospitals [14]. In the meantime, the regional differences in ARI cases among Afghani Hajjis were unexpected. This could be partly explained by the sudden change of climate experienced by Hajjis coming from the colder areas of Afghanistan and getting suddenly exposed to the warmer climate of Saudi Arabia. Another study conducted in Saudi Arabia also claims that respiratory tract infection during Hajj is a common illness with 40% of Hajjis developing symptoms of ARI [15,16]. No considerable changes in the prevalence of diarrhea and jaundice in the pre- transit, transit and Hajj periods were found. The low rate of diarrheal diseases among Afghan Hajjis was also surprising and suggestive of further analysis. A comparison for these findings could not be established with other similar studies. Nevertheless, the prevalence of ARI’s symptoms among Malaysian pilgrims was higher (58.9%), about the same (35.2%) among pilgrims from Iran, and lower (15.6%) among French pilgrims [21,22]. This could be explained by not using a standard definition for ARI and the recall bias being a possible limitation of this study. In the meantime, documentation of 54% of the Hajjis being illiterate can also affect the symptoms of diseases being reported by the respondents. Additionally, a loss in the follow-up of as many as 28% among Hajjis from the northern part of the country limits acceptability of the results. Also, low coverage of the phone network in the north being the main means of gathering subjective data from Hajjis upon their arrival in turn delaying interviewing Hajjis could further limit acceptability of the findings. Not only that, cluster sampling used as the study’s main method also limited generalizability of the findings. Above all, a high level of motivation among Hajjis contributed to a considerable level of participation in the study, which resulted in the study results being promising. Lastly, realizing that local pilgrims were exposed to being infected by viral hepatitis due to their undertaking certain risky activities, the study did not find any positive cases of viral hepatitis. This is also a part of the study limitations caused by difficulty in following up with local pilgrims after their arrival back home, as well as the long incubation period of the disease itself. Attempting to establish identified cases of jaundice on the subjective complaint of “visible yellowish skin or sclera” and then base it as a proxy indicator for detecting hepatitis was another limitation of the study. In the meantime, the duration of 30–45 days that the local pilgrims stayed in Hajj was not a long enough time to detect symptoms for blood-borne hepatitis, particularly hepatitis B, as the overage timing required for relevant symptoms to appear is approximately 90 days.
Since the prevalence of ARI increased up to 37% during Hajj, further investigation is required to be carried out to determine the possible causes of ARI among Afghan pilgrims during Hajj. Secondly, follow-up studies need to be conducted to determine the incidence of viral hepatitis among local pilgrims. This will enable the Afghan MoPH to come up with practically sound strategies to overcome the case of ARI among pilgrims during Hajj. Additionally, further research is needed to better address contributing factors to ARI in spite of Hajjis being given the flu vaccine in their home country. Meanwhile, in order to be more proactive and regularly alerted, the current surveillance system in the MoPH needs to be strengthened and upgraded in order to initiate a regular follow-up of the Hajjis upon their arrival back home. This will enable the researchers to track possible changes in their health status, more importantly focusing on the possible development of hepatitis cases. Although some studies during Hajj investigated the etiology of ARI and reported bacterial pathogens in 29.9% of sputum specimens and throat swabs and viruses in 19.5% [17], including influenza [18], a laboratory-supported survey is recommended to reveal the etiology of ARI among pilgrims. With this in mind, ARI transmission can be efficiently reduced by simple and low-cost physical measures, including the use of facemasks and hand hygiene. However, awareness and acceptability of these measures among pilgrims are limited and highly concerning which give the alert to put pragmatic measures in place to tackle the problems [19].
Additionally, noticing the nationwide data on local pilgrims showing that a large number of Hajjis are either illiterate or have a low level of education, the national health promotion strategy of the MoPH needs to include a special section on educating and orienting local pilgrims about the health risks they face while staying in the transit area and during the event. Hajj as a mass gathering provides an opportunity to improve health systems and strengthen surveillance to minimize health risks and improve health behaviors [20]. To this end, it could be recommended that the Afghan MoPH needs to launch an agreement with their counterparts in Saudi Arabia on initiating a pragmatic rapid detection and response mechanism to tackle commonly occurring communicable diseases among all Hajjis, in particular the Afghan Hajjis during the event.
References
Cite this article
TY - JOUR AU - Khwaja Mir Islam Saeed AU - Jawad Mofleh AU - M. Hafiz Rasooly AU - M. Iabal Aman PY - 2012 DA - 2012/12/27 TI - Occurrence of acute respiratory infection, diarrhea and jaundice among Afghan pilgrims, 2010 JO - Journal of Epidemiology and Global Health SP - 215 EP - 220 VL - 2 IS - 4 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2012.11.003 DO - 10.1016/j.jegh.2012.11.003 ID - Saeed2012 ER -