
Using Fuzzy Sets in Surgical Treatment Selection and Homogenizing Stratification of Patients with Significant Chronic Ischemic Mitral Regurgitation
- DOI
- 10.2991/ijcis.d.190923.002How to use a DOI?
- Keywords
- Conditional degrees of membership; Fuzzy samples; Product t-norm; Bayesian classifier; Independent continuous features
- Abstract
We present three (main one and two auxiliary) fuzzy algorithms to stratify observations in homogenous classes. These algorithms modify, upgrade and fuzzify crisp algorithms from our earlier works on a medical case study to select the most appropriate surgical treatment for patients with ischemic heart disease complicated with significant chronic ischemic mitral regurgitation. Those patients can be treated with either surgical revascularization and mitral valve repair (group A) or with isolated surgical revascularization (group B) depending on their health status. The main algorithm results in a fuzzy partition of patients in two fuzzy sets (groups A and B) through identification of their degrees of membership. The resulting groups are highly non-homogenous, which impedes subsequent proper comparisons. So, the two auxiliary algorithms further stratify each group into two homogenous subgroups with comparatively preserved medical condition (A1 and B1) and with comparatively deteriorated medical condition (A2 and B2). Those two algorithms perform fuzzy partition of patients from A and B respectively into A1, A2, B1 and B2 by identifying their conditional degrees of membership to those subgroups. We then utilize the product t-norm to calculate the degree of membership of patients to their respective subgroup as an intersection of two fuzzy sets. We demonstrate how to form fuzzy samples for medical parameters for any subgroup. We also compare the performance of the fuzzy algorithms with their preceding crisp version, as well as with eight Bayesian classifiers. We then assess the quality of classification by modified confusion matrices, summarized further into four criteria. The fuzzy algorithms show total superiority over the other methods, and excellent differentiation of typical patients and outliers. On top, only the fuzzy algorithms provide a measure of how typical a patient is to its subgroup. The fuzzy algorithms clearly outline the role of the Heart Team, which is missing in the Bayesian classifiers.
- Copyright
- © 2019 The Authors. Published by Atlantis Press SARL.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
The ischemic heart disease (IHD) is considered one of the most widely spread heart disease globally. When it is further complicated with ischemic mitral regurgitation (IMR, also referred as functional mitral regurgitation in recent works—FMR), the mitral valve (MV, between the left atrium and left ventricle) does not function well and part of the blood pumped from the left ventricle returns to the left atrium. Recent research shows a tendency for this medical condition to occur not only among elderly people, but also among patients between 40 and 50 years old [1]. The prognosis for patients with IMR is worse than for patients with mitral regurgitation with a different cause (primary mitral regurgitation—PMR) due to the connection between IMR and the insufficiency of the left heart ventricle as this disease is the main cause for the IMR and tends to progress [2]. Patients with mild IMR (also called 1st degree), are usually subjected to isolated revascularization (CABG) [3–5]. Patients with severe IMR (which includes 3th to 4th degree and 4th degree IMR), are traditionally subjected to operation using MV repair performed as a concomitant procedure with surgical revascularization (MVRepair + CABG) [6–11]. The term significant IMR includes mild to moderate IMR (a.k.a. 1st to 2nd degree IMR), moderate IMR (a.k.a 2nd degree or 2nd to 3rd degree IMR) and moderate to severe IMR, (a.k.a. 3rd degree IMR) [12]. For some patients with significant IMR the MVRepair + CABG is selected, while for others the choice is CABG alone. For the sake of simplicity, we shall denote the first group as A, and the second one as group B. The selection of surgical treatment in the case of significant IMR is not trivial, and the same applies to the assessment of the effect of MVRepair. In the rest of the paper, the term IMR will refer to significant chronic IMP.
To evaluate the effect of MVRepair to patients with IMR we will compare the medical status of patients before and after surgical intervention. This approach has three elements of difficulty:
Traditionally the classification of patients is made quantitatively and there is no specific measure of how typical a patient is for a given group
The groups are non-homogenous, and their comparison is significantly complicated
The classification to each group is made based on assessment of the general medical status of every single patient and errors are possible since the task is informatively very complicated.
The second and third difficulty are addressed in Ref. [13], which presents the results from a survey on IHD complicated with IMR among Bulgarian patients. This work proposed a formalized algorithm to define the operative treatment as CABG + MVRepair or CABG alone. Additionally, Ref. [14] presented two stratification algorithms to divide each group into two comparatively more homogenous subgroups depending on the pre-operative medical status of the patients: comparatively preserved status (subgroups A1 and B1) or comparatively damaged status (subgroups A2 and B2). In this way, comparison is possible not only between groups A and B directly, but also between A1 and B1 on one hand and between A2 and B2 on the other hand. So, it is possible to assess the effect of MVRepair much more adequately. Those algorithms, however, treat the groups A and B as crisp sets [15]. Crisp sets are also known as classical sets, where the object either entirely belongs to that set or does not belong to it. As a result, there was no measure of typicality of a patient to its subgroup and subsequently the crisp algorithms cannot identify outliers.
However, the groups A and B are somewhat ambiguously defined and are fuzzy sets rather than crisp sets. For example, the fuzziness of group B may be explained by the fact that each patient may be subjected to CABG, but the procedure is not equally suitable to all patients. The degree of membership [15] of the patient to group B is a quantitative measure of just how much this procedure is suitable to a given patient. Part of the patients are very suitable for this procedure and their degree of membership would be 1. Other patients are not suitable for the procedure and their degree of membership would be 0. For the remaining patients, the degree of membership will be between 0 and 1. Evidently, the boundaries of the set of patients, who will benefit from CABG are not clear, but ambiguous. The same applies to group A, as well as for subgroups A1, A2, B1 and B2. Because of all stated above, to deal with the first element of difficulty, in addition to defining the subgroup, we also need to assess the degree of membership to the respective subgroup for each patient.
There is an important practical benefit to determine the degrees of membership. Let patient Х be assigned to subgroup B1 with a degree of membership 0.6, while patient Y be assigned to the same subgroup with degree of membership 1. It makes no sense to assume that the characteristics of those two patients will have the same influence in the formation of the characteristics of subgroup B1. If we model the problem using crisp sets, then the two patients would have equal weight in the formation of the aggregated characteristics of subgroup B1. If we use fuzzy sets (as defined in Ref. [16]), then the characteristics of patient Y would have a higher weight in the formation of the aggregated characteristics of subgroup B1 than those of patient X.
This motivates the essence of this paper, which is to modify, upgrade and fuzzify the algorithms from Refs. [13,14]. We shall formalize three new classification algorithms:
A fuzzy algorithm to determine the surgical treatment of patients with significant IMR as classification into two groups: MVRepair + CABG (group A) and CABG alone (group B)
A fuzzy algorithm for homogenizing stratification of patients allocated for MVRepair + CABG (group A) as classification into two subgroups: with comparatively preserved status (subgroup A1) and with comparatively damaged status (subgroup A2)
A fuzzy algorithm for homogenizing stratification of patients allocated for CABG alone (group B) as classification into two subgroups: with comparatively preserved status (subgroup B1) and with comparatively damaged status (subgroup B2)
As an output, the three algorithms shall give the degree of membership for each patient to the fuzzy subgroup in which the patient is classified. This will allow to form four fuzzy samples of patient data for each measured parameter (i.e. one for each subgroup). By doing so, we will also address the three above mentioned difficulties in the assessment of the effect of MVRepair.
In what follows, sections 2, 3 and 4 consecutively present the steps and logic of the three fuzzy algorithms for classification of patients to groups and subgroups. The algorithms produce the degrees of membership to the groups as well as the conditional degrees of membership to the subgroups. Section 5 discusses the procedures to calculate the degrees of membership to the subgroups using the product t-norm. Section 6 presents the applications of the three fuzzy classification algorithms in the medical case study from Refs. [13,14] over patients with IHD complicated with IMR and also demonstrates how to form fuzzy samples using the calculated degrees of membership. In section 6, we will also compare the results from the fuzzy algorithms with the results from eight Bayesian classifiers, as well as those of the crisp algorithms from Refs. [13,14]. We shall introduce criteria to facilitate the performance estimation of each classification. Section 7 discusses further on the rationale of our fuzzy algorithms, with concluding remarks given in section 8.
2. MAIN ALGORITHM AND IDENTIFICATION OF THE GROUP DEGREE OF MEMBERSHIP
The purpose of this section is to formalize the process of defining the type of operative treatment of patients with IHD, complicated with IMR, which can be either an isolated revascularization (CABG) or a revascularization combined with MVRepair (MVRepair + CABG).
From an informational stand point, this problem may be defined as fuzzy partition [17] of the patients with IHD, complicated with IMR, into two groups—A (combined treatment) and B (isolated revascularization). During the classification we need to find the degree of membership of the patient to the group she/he is classified to (
The choice of operative treatment is formalized using a 6-step main algorithm (MA):
If patients are with very deteriorated general and medical condition, they need to be subjected to the least invasive operation to improve the status of the heart using revascularization without taking the risks of the combined surgical treatment. That is why for those patients the choice of group B is undoubted. In that sense we can formulate the following primary criteria for exclusion from group A (i.e. for inclusion in group B):
deteriorated medical status with additional medical conditions (lung diseases, peripheral vascular disease, cerebrovascular disease), especially for patients at older age;
subjectively assessed possible life expectancy of not more than 4 years;
significant left ventricular dysfunction with left ventricular ejection fraction (LVEF) under 25% and explicit heart failure;
relative contraindications for operation with cardio-pulmonary bypass, or indications for the least invasive operation possible.
If any of those primary criteria is present, the patient is classified in group B for isolated revascularization with a degree of membership
After concluding that the patient's status is not too deteriorated then the presence of very significant regurgitation through the MV needs to be identified. If present, then the patient is undoubtedly classified in group A, because the lack of MVRepair will be associated with a bad prognosis regarding progression of IMR and left ventricular reverse remodeling [18,19]. In that sense, the following secondary criteria for exclusion from group B can be defined (i.e. for inclusion into group A)
moderate to severe IMR (3rd degree);
moderate IMR (2nd to 3rd degree) with regurgitation volume of over 30 mL;
moderate IMR (2nd to 3rd degree) with regurgitation volume not more than 30 mL, but with vena contracta at least 7 mm.
If any of those secondary criteria is present, the patient is classified in group A for combined operation with a degree of membership
So far, we know that the patient is neither with very deteriorated status nor with very significant regurgitation through the MV. If it turns out that the patient has lower significant regurgitation through the MV, then the classification into group B is undoubted, because the plastic of MV is unmotivated (it would increase the operational risk without improving the post-operative status of the patient). In that case, the presence of mild to moderate IMR (1st to 2nd degree) may be treated as a criterion for exclusion from group A (i.e. for inclusion into group B).
If there is mild to moderate IMR (1st to 2nd degree), then the patient is classified in group B with a degree of membership
It has been defined that for the patient, both operations are possible because the patient does not have very deteriorated status and has moderately significant regurgitation through the MV. The classification is made by measuring a series of parameters to test if those form a typical profile for groups A and B, as described below:
The typical profile for group A includes:
moderate IMR (2nd to 3rd degree)
regurgitation volume between 20 mL and 30 mL
vena contracta between 4 mm and 7 mm
tenting area between 1.5 cm2 and 2.5 cm2
tenting height between 10 mm and 20 mm
coaptation line between 1 mm and 4 mm
presence of tethering
subjectively assessed possible life expectancy over 5 years;
The typical profile for group B includes:
moderate IMR (2nd degree)
regurgitation volume between 10 mL and 20 mL
vena contracta between 3 mm and 4 mm
tenting area between 0.8 cm2 and 1.5 cm2
tenting height between 6 mm and 10 mm
coaptation line between 3 mm and 5 mm
lack of tethering
If the pre-operative status of the patient coincides with one of those typical profiles for groups A and B, then the patient is classified into the respective group with a degree of membership
So far, we know that the patient does not have very deteriorated status, has moderately significant regurgitation through the MV and the pre-operative profile does not coincide with either one of the typical profiles for groups A and B. Here again, both operations are possible. Then a decision for classification can be made by the Heart Team [20]. When the echocardiographic criteria for assessment of mitral regurgitation and of left atrium remodelling are very contradicting, the decision for the volume of operation may be based on a “stress echocardiographic test” which should show how the characteristics of the mitral regurgitation change. The general medical status of the patient is also considered, as well as the presence of other medical conditions. During a “stress test” which does not provoke increase of IMR and in the case of expected higher operational risk with no significant improvement of the repair of MV the recommended approach is isolated revascularization, sometimes as open-heart surgical procedure (i.e. classification in group B). In case the degree of IMR increases during the “stress test,” a better effect from the MVRepair is expected, and the risks of the operation are comparatively low, the patient is classified in group A. Group A also accommodates patients in work-active age, who aim to achieve the best possible recovery back to normal physical activity and working capacity.
The Heart Team must assess (using their expert knowledge) which is the typical profile (for groups A and B) that is most similar to the status of the patient. If there is consensus then the patient is classified in the respective group with degree of membership
So far, we know that the patient does not have very deteriorated status, has moderately significant regurgitation through the MV, the pre-operative profile does not coincide with either one of the typical profiles for groups A and B and the Heart Team has not reached a consensus on the choice of operative treatment. In that case, the final decision is made by the operating surgeon (based on her/his own expertise and that of the institution).
The operating surgeon must assess (using her/his expert knowledge) which is the typical profile (for groups A and B) that is most similar to the status of the patient. Then the patient is classified in the respective group with a degree of membership
The block diagram for MA is presented in Figure 1.

Main algorithm (MA) as presented in Ref. [13].
3. AUXILIARY ALGORITHM FOR A AND IDENTIFICATION OF THE CONDITIONAL DEGREE OF MEMBERSHIP
According to MA, the patients with combined operation (CABG + MVRepair) may be classified in group A in four different ways, respectively in steps 2, 4, 5 or 6. It is evident that group A is strongly non-homogenous. For this study, these patients will be further divided (for clarity of information) into two subgroups—A1 and A2. Subgroup A1 will accommodate the patients with better heart condition and general status, but its aim is to achieve the best possible improvement of the heart condition (reverse remodelling of heart chambers) to bring the patient back to normal lifestyle. Subgroup A2 will take the patients with more damaged heart condition and general status, where the purpose is to apply MVRepair strategy to achieve treatment of the heart insufficiency caused by IHD and MR. The expectation for those patients is to stop or slow down the process of remodelling of the left heart chambers rather than achieve its reverse remodelling.
From an information stand point, this task is in fact fuzzy partition into two subgroups—A1 (comparatively preserved status) and A2 (comparatively deteriorated status) of the patients with IHD, complicated with IMR classified for CABG + MVRepair in group A. During the classification, we need to find the degree of membership of the patient to the subgroup he/she was classified provided that the former belongs to group A for sure (
The information task of dividing patients from group A into two subgroups is formalized using a 6-step auxiliary algorithm for A (AAA):
Let the patient be classified in group A according to step 2 of MA, i.e. the patient is not with very severe medical condition and has highly significant regurgitation through the MV. The classification is made by measuring a series of parameters to test if those form a typical primary profile for subgroups A1 and A2, as described below:
The typical primary profile for subgroup A1 includes:
stable angina pectoris
no prior myocardial infarction
ejection fraction (EF) above 45%
good general condition
lack of other medical conditions that worsen the prognosis
left ventricle end-diastolic volume index (LVEDVi) not more than 75 mL/m2 B.S.A.
left ventricle end-systolic volume index (LVESVi) not more than 35 mL/m2 B.S.A.
left atrial volume index (LAVi) not more than 35 mL/m2 B.S.A.
The typical primary profile for A2 includes:
unstable angina pectoris
medical history for prior myocardial infarction
EF below 40%
not very good general condition
presence of other medical conditions that worsen the prognosis (comorbidities)
LVEDVi above 80 mL/m2 B.S.A.
LVESVi above 40 mL/m2 B.S.A.
LAVi over 40 mL/m2 B.S.A.
If the pre-operative profile of the patient coincides with either one of the typical primary profiles for subgroups A1 and A2, then the patient is classified in the respective subgroup with degrees of membership
Assume that the patient is classified in group A according to step 2 of MA, i.e. the patient does not have very deteriorated medical condition and has very high regurgitation through the MV. So far, we know that the pre-operative profile of the patient does not coincide with any of the typical primary profiles for subgroups A1 and A2. Then the decision for classification should be based on the expert assessment of the Heart Team. This assessment depends, on one hand, on the overall echocardiographic profile (which may give indication for stable or compromized function of the left heart chambers, as well as for the stage of progression of the changes in the heart because of the ischemic remodelling), while on the other hand it depends on the overall status of the patient and the presence of other medical conditions.
The Heart Team must assess (using their expert knowledge) which is the typical primary profile (for subgroups A1 and A2) that is most similar to the status of the patient. If there is consensus then the patient is classified in the respective subgroup with a degree of membership
Assume that the patient is classified in group A according to step 2 of MA, i.e. the patient does not have very damaged medical status and has very high regurgitation through the MV. So far, we know that the pre-operative profile of the patient does not coincide with either one of the typical primary profiles for subgroups A1 and A2, and the Heart Team has not reached a consensus on the choice of operative treatment. In that case, the final decision is made by the operating surgeon.
The operating surgeon must assess (using her/his expert knowledge) which is the typical primary profile (for subgroups A1 and A2) that is most similar to the status of the patient. Then the patient is classified in the respective group with a degree of membership
Let the patient be classified in group A according to steps 4, 5 or 6 of MA, i.e. the patient does not have very high regurgitation through the MV. The classification is made by measuring a series of parameters to test if those form a typical secondary profile for subgroups A1 and A2, as described below:
The typical secondary profile for subgroup A1 includes:
no prior myocardial infarction
EF above 40%
good general condition
lack of other medical conditions that worsen the prognosis
LVEDVi not more than 80 mL/m2 B.S.A.
LVESVi not more than 40 mL/m2 B.S.A.
LAVi not more than 40 mL/m2 B.S.A.
The typical secondary profile for subgroup A2 includes:
medical history for prior myocardial infarction
EF below 35%
not very good general condition, presence of other medical conditions (comorbidities) that worsen the prognosis
LVEDVi above 85 mL/m2 B.S.A.
LVESVi above 45 mL/m2 B.S.A.
LAVi over 45 mL/m2 B.S.A.
If the pre-operative profile of the patient coincides with either one of the typical secondary profiles for subgroups A1 and A2, then the patient is classified in the respective subgroup with a degrees of membership
Let the patient be classified in group A according to steps 4, 5 or 6 of the MA, i.e. the patient does not have very high regurgitation through the MV. So far, we know that the pre-operative profile of the patient does not coincide with any of the typical secondary profiles for subgroups A1 and A2. Then the decision for classification should be based on the expert assessment of the Heart Team. This assessment depends, on one hand, on the overall echocardiographic profile (which may give indication for stable or compromized function of the left heart chambers, as well as for the stage of progression of the changes in the heart because of the ischemic remodelling), while on the other hand it depends on the overall status of the patient and the presence of other medical conditions.
The Heart Team must assess (using their expert knowledge) which is the typical secondary profile (for subgroups A1 and A2) that is most similar to the status of the patient. If there is consensus then the patient is classified in the respective subgroup with a degree of membership
Let the patient be classified in group A according to steps 4, 5 or 6 of the MA, i.e. the patient does not have very high regurgitation through the MV. So far, we know that the pre-operative profile of the patient does not coincide with any of the typical secondary profiles for subgroups A1 and A2 and the Heart Team has not reached a consensus on the choice of operative treatment. In that case, the final decision is made by the operating surgeon.
The operating surgeon must assess (using her/his expert knowledge) which is the typical secondary profile (for subgroups A1 and A2) that is most similar to the status of the patient. Then the patient is classified in the respective group with a degree of membership
The rationale of AAA is based on the following three medical aspects:
If the ischemic remodelling of the heart is at a comparatively early stage, then the classification to subgroup A1 is undoubted.
If the ischemic remodelling of the heart is at a comparatively advanced stage, then the classification into subgroup A2 is also undoubted;
If the patient is classified in group A according to step 2 of MA, then the patient is with comparatively more high-staged IMR as compared to the one she/he might have if classified in group A according to steps 4, 5 or 6 of MA. Therefore, if the ischemic remodelling of the heart is stable, then the patient that was classified in group A according to step 2 of the MA should be allocated to subgroup A2, whereas a patient classified in group A according to steps 4, 5 or 6 of the MA should be allocated to subgroup A1.
The block diagram for AAA is given in Figure 2.
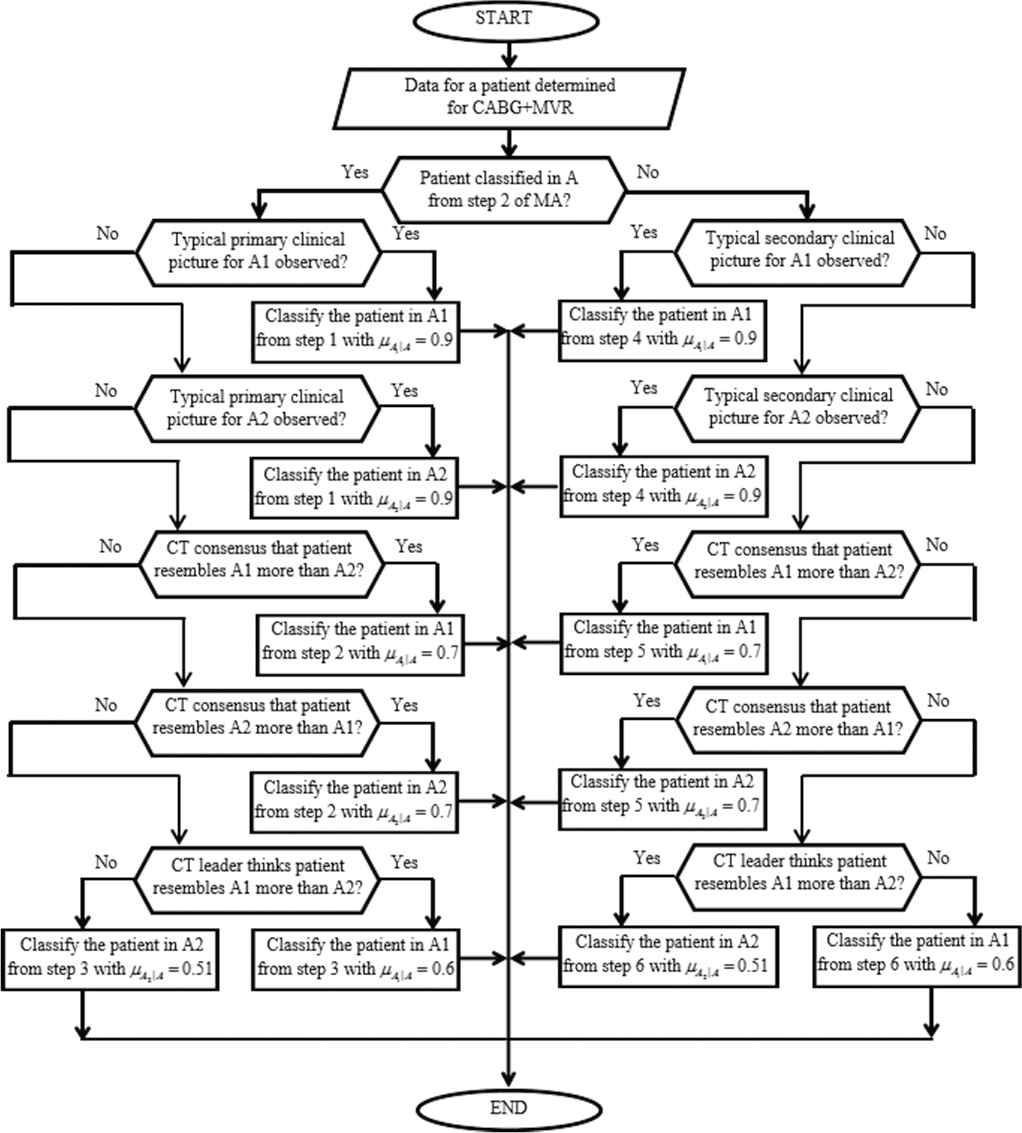
Auxiliary algorithm for A (AAA) as presented in Ref. [13].
4. AUXILIARY ALGORITHM FOR B AND IDENTIFICATION OF THE CONDITIONAL DEGREE OF MEMBERSHIP
According to MA, the patients with isolated revascularization (CABG) may be classified in group B in five different ways, respectively in steps 1, 3, 4, 5 and 6. It is evident that group B is strongly non-homogenous. For this study, these patients will be further divided (for clarity of information) into two subgroups—B1 and B2. Subgroup B1 will accommodate the patients with comparatively preserved heart and general status, where the expectation is that revascularization (with no further risks from a combined operation) will bring significant improvement in the heart condition (with subsequent reversed remodelling of the left heart chambers), which will allow to bring the patient back to normal lifestyle. Subgroup B2 will include the patients with comparatively deteriorated heart condition and general status, with subjectively assessed probable life expectancy under 3 years, where the purpose is to use the most non-invasive operation to treat the IHD and the heart insufficiency that results from the IHD, complicated with IMR. Part of those patients may be subjected to operation without cardio-pulmonary bypass (ОРСАВ) to make the operation as less invasive as possible. For other patients the purpose would be to control the clinical status of unstable angina.
From an informational stand point, this task may be described as fuzzy partition into two subgroups—B1 (comparatively preserved status) and B2 (comparatively damaged status) of patients with IHD, complicated with IMR, classified for CABG, i.e. classified in group B. During the classification, we need to find the degree of membership of the patient to the subgroup she/he was classified provided that the latter belongs to group B for sure (
The information task of dividing patients from group B into two subgroups is formalized using a 7-step auxiliary algorithm for B (AAB):
Let the patient be classified in group B according to step 1 of MA, i.e. the patient is with very severe medical condition. Then the patient is classified in group B2 with degree of membership
Let the patient be classified in group B according to steps 4, 5 or 6 of MA, i.e. the patient is not with very severe medical condition and has significant but not more than moderate mitral regurgitation through the MV. The classification is made by measuring a series of parameters to test if those form a typical primary profile for subgroups B1 and B2.
The typical primary profile for subgroup B1 includes:
stable angina pectoris
no medical history for prior myocardial infarction
EF above 45%
good general health
lack of comorbidities that worsen the prognosis
no limitations to conduct operation with cardio-pulmonary bypass
LVEDVi not more than 75 mL/m2 B.S.A.
LVESVi not more than 35 mL/m2 B.S.A.
LAVi not more than 35 mL/m2 B.S.A.
The typical primary profile for subgroup B2 includes:
unstable angina pectoris
medical history for prior myocardial infarction
EF less than 40%
not very good general and medical condition
presence of comorbidities that worsen the prognosis
LVEDVi above 80 mL/m2 B.S.A.
LVESVi above 40 mL/m2 B.S.A.
LAVi above 40 mL/m2 B.S.A.
limitations to perform operation with cardio-pulmonary bypass
If the pre-operative profile of the patient coincides with either one of the typical primary profiles for subgroups B1 and B2, then the patient is classified in the respective subgroup with a degree of membership
Assume that the patient is classified in group B according to steps 4, 5 or 6 of MA, i.e. the patient does not have very deteriorated medical condition and has significant but not severe MV regurgitation. So far, we know that the pre-operative profile of the patient does not coincide with any of the typical primary profiles for subgroups B1 and B2. Then the decision for classification should be based on the expert assessment of the Heart Team. This assessment depends, on one hand, on the overall echocardiographic profile (which may give indication for stable or compromised function of the left heart chambers, as well as for the stage of progression of the changes in the heart as a result of the ischemic remodelling), while on the other hand it depends on the general health status of the patient and the presence of comorbidities.
The Heart Team must assess (using their expert knowledge) which is the typical primary profile (for subgroups B1 and B2) that is most similar to the status of the patient. If there is consensus then the patient is classified in the respective subgroup with a degree of membership
Assume that the patient is classified in group B according to steps 4, 5 or 6 of MA, i.e. the patient does not have very deteriorated medical condition and has significant but not more than moderate MV regurgitation. So far, we know that the pre-operative profile of the patient does not coincide with either one of the typical primary profiles for subgroups B1 and B2, and the Heart Team has not reached a consensus on the choice of operative treatment. In that case, the final decision is made by the operating surgeon.
The operating surgeon must assess (using her/his expert knowledge) which is the typical primary profile (for subgroups B1 and B2) that is most similar to the status of the patient. Then the patient is classified in the respective group with a degree of membership
Let the patient be classified in group B according to steps 3 of the MA, i.e. the patient does not have very deteriorated medical condition and has significant mild to moderate MV regurgitation. The classification is performed by measuring a series of parameters to test if those form a typical secondary profile for subgroups B1 and B2, as described below.
The typical secondary profile for subgroup B1 includes:
no medical history for myocardial infarction
EF above 40%
good general health
lack of comorbidities that worsen the prognosis
no limitations to conduct operation with cardio-pulmonary bypass
LVEDVi not more than 80 mL/m2 B.S.A.
LVESVi not more than 35 mL/m2 B.S.A.
LAVi not more than 40 mL/m2 B.S.A.
The typical secondary profile for subgroup B2 includes:
medical history for prior myocardial infarction
EF below 35%
not very good general and medical condition
presence of comorbidities that worsen the prognosis
LVEDVi above 85 mL/m2 B.S.A.
LVESVi above 45 mL/m2 B.S.A.
LAVi above 45 mL/m2 B.S.A.
no limitations to perform operation with cardio-pulmonary bypass
If the pre-operative profile of the patient coincides with either one of the typical secondary profiles for subgroups B1 and B2, then the patient is classified in the respective subgroup with degrees of membership
Assume that the patient is classified in group B according to step 3 of MA, i.e. the patient does not have very deteriorated medical condition and has significant mild to moderate MV regurgitation. So far, we know that the pre-operative profile of the patient does not coincide with any of the typical secondary profiles for subgroups B1 and B2. Then the decision for classification should be based on the expert assessment of the Heart Team. This assessment depends, on one hand, on the overall echocardiographic profile (which may give indication for stable or compromized function of the left heart chambers, as well as for the stage of progression of the changes in the heart because of the ischemic remodelling), while on the other hand it depends on the overall status of the patient and the presence of comorbidities.
The Heart Team must assess (using their expert knowledge) which is the typical secondary profile (for subgroups B1 and B2) that is most similar to the status of the patient. If there is consensus then the patient is classified in the respective subgroup with a degree of membership
Assume that the patient is classified in group B according to step 3 of MA, i.e. the patient does not have very deteriorated medical status and has significant mild to moderate MV regurgitation. So far, we know that the pre-operative profile of the patient does not coincide with either one of the typical secondary profiles for subgroups B1 and B2, and the Heart Team has not reached a consensus on the choice of operative treatment. In that case, the final decision is made by the operating surgeon.
The operating surgeon must assess (using her/his expert knowledge) which is the typical secondary profile (for subgroups B1 and B2) that is most similar to the status of the patient. Then the patient is classified in the respective group with a degree of membership
The rationale of AAB is based on the following six medical aspects:
If the patient is classified in group B according to step 1 of MA then the patient has severely deteriorated medical status and the classification in subgroup B2 is undoubted;
If the ischemic remodelling of the heart is at an early stage, then the classification in subgroup B1 is undoubted for a patient classified in group B according to steps 3, 4, 5 or 6 of MA;
If the ischemic remodelling of the heart is in comparatively advanced stage, then the classification in subgroup B2 is also undoubted for patients classified in group B according to steps 3, 4, 5 or 6 of MA;
If the patient is classified in group B according to steps 4, 5 or 6 of MA, then the she/he has significantly more severe MR than if she/he was classified in group B according to step 3 of MA. Therefore, if the ischemic remodelling of the heart is stable then a patient, classified in group B, according to steps 4, 5 or 6 of MA should be classified in subgroup B2, whereas a patient classified in group B according to step 3 of MA should be classified in subgroup B1;
The MR of a patient classified in group B according to steps 4, 5 or 6 of MA is significantly lower than that of a patient classified in group A according to step 2 of MA. In the second case, however, the decrease of MR is one of the objectives of the operative treatment, whereas in the first case the MR will be treated as complication during the isolated revascularization. Because of all those considerations, the typical primary profiles for subgroups B1 and B2 are similar to the typical primary profiles for subgroups A1 and A2.
The MR of a patient classified in group B according to step 3 of MA is significantly lower than that of a patient classified in group A according to steps 4, 5 or 6 of MA. In the second case, however, the decrease of MR is one of the objectives of the operative treatment, whereas in the first case the MR will be treated as complication during the isolated revascularization. Because of all those considerations, the typical secondary profiles for subgroups B1 and B2 are similar to the typical secondary profiles for subgroups A1 and A2.
The block diagram for the AAB is given in Figure 3.
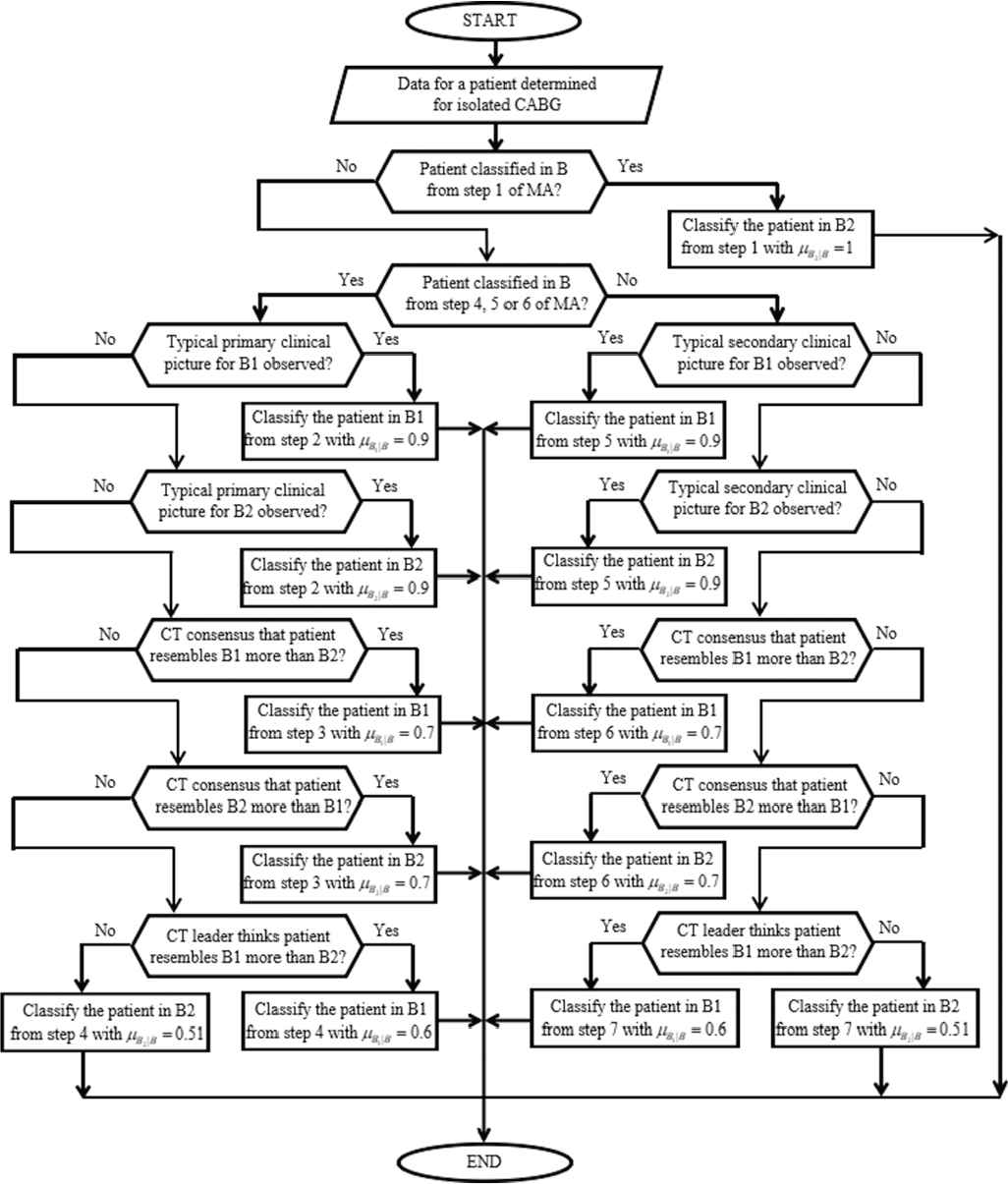
Auxiliary algorithm for B (AAB) as presented in Ref. [13].
5. CALCULATION OF THE DEGREE OF MEMBERSHIP TO THE SUBGROUP
Assume that we have determined the subgroup of a patient using MA and either AAA or AAB. If the patient is classified in A1, then
For example, if a patient is to be classified in the fuzzy subgroup B1, then the former needs to be a member of the fuzzy group B and simultaneously to be a member of the fuzzy subgroup B1, if she/he belongs to the group B with certainty. That is why we should use a fuzzy intersection, a.k.a. t-norm (which is the short for triangular norm) to calculate the degree of membership to this intersection using the degrees of membership to the two abovementioned fuzzy sets [15]. The t-norm is some generalization of the intersection operation over two crisp sets, in the same way the degree of membership is a generalization of the indicator function of the crisp set. The latter is 1 for any element of the crisp set, and 0 for any non-element of the crisp set. There are uncountable many t-norms [21]. However, four t-norms are considered basic and are broadly accepted by the fuzzy-theory community: standard t-norm (a.k.a. minimum t-norm), drastic t-norm, Lukasiewicz t-norm, and product t-norm [22,23]. We have selected to use the product t-norm to calculate the degree of membership
Then the degrees of membership of a given patient to the subgroup to which she/he is classified can be calculated using the respective formula from the four given below:
We have selected the product t-norm (1) because of three reasons.
The first reason relates to the required properties of the t-norm in this case. It is obvious, that the t-norm should be defined for any
The second reason is that using the product t-norm we can obtain results, which apply equally well to membership functions and to subjective probabilities. By doing so we can bypass the problem for interpretation of
The third reason is that the absence of idempotence is irrelevant in our context. The idempotence property of a t-norm deals with a situation, where X and Y coincide and obviously Z, as their intersection, also coincides with them. So
6. EXPERIMENTAL RESULTS
6.1. Medical Data
The above discussed algorithms are tested over data for patients with IHD complicated with IMR, collected over 4 years at the Department of Cardiac Surgery, St. Marina University Hospital in Varna, Bulgaria.
The criteria to include patients in the survey are:
Patients with IHD, proven through coronary angiography (interventional or computer-assisted) that have indications for operative revascularization [25];
Information for post-myocardial infarction scar at the area of postero-medial and/or antero-lateral papillary muscle;
Not less than 7 days after onset of acute myocardial infarction;
Echocardiographic evaluation of the morphology and function of the MV, which shows IMR (mild to moderate, moderate, or moderate to severe IMR – 1st to 2nd, 2nd, 2nd to 3rd, or 3rd degree) without morphological changes in the MV apparatus (secondary MV regurgitation);
Age between 18 and 80 years;
Subjectively assessed probable life expectancy over 3 years [2,26];
No prior heart surgeries;
No contraindications for open-heart surgery.
A total of 140 patients complied with those criteria. For every patient, the following parameters are recorded and archived: 16 identificators, 14 anamnesis parameters, 2 treatment cost parameters and 12 tripled parameters. The latter 12 tripled parameters were measured first before the operation, then shortly after the operation (5 to 10 days post-operatively), and finally - late after operation (6 to 54 months post-operatively). Therefore, every tripled parameter is in fact three different values in different time points. So, every patient is described by a 68-dimensional record of the following parameters:
Identificators: identification number, subgroup, local subgroup index, step in MA for classification in A or B, step in AAA for classification in A1 и A2, step in AAB for classification in B1 or B2,
Anamnesis parameters: age, gender, emergency of operation, diabetes, cerebrovascular incidents, renal failure, type of angina pectoris, pre-operative arrhythmia, New York Heart Association (NYHA) functional class, myocardial infarction, previous percutaneous coronary intervention, left main coronary artery stenosis, SYNTAX score, pre-operative tethering of the MV.
Treatment cost parameters: hours spent in intensive care unit, days spent in hospital.
Tripled parameters: LVEDVi, LVESVi, LAVi, degree of mitral regurgitation, regurgitation volume, vena contracta, coaptation height, tenting area, tenting height, proximal isovelocity surface area radius, EF, modified EF.
The data are collected from medical history of each patient, trans-thoracic 2D echocardiography (TTE) including colour and pulse Doppler, and in most of the cases with intraoperative trans-oesophageal echocardiography (TEE).
The leading medical experts at the Department of Cardiac Surgery analysed all 68-dimensional records and divided the patients into 4 groups—A1, A2, B1, B2. Additionally, some of the classified patients were defined as outliers if their clinical status was contradictory and the parameters were not consistent. During this classification, the leading medical experts used pre-operative and post-operative data and in fact the classification was performed in hindsight. In that way, the reliability of this classification is beyond doubt. Let's denote this as “absolute” classification.
6.2. Fuzzy Classification by the Heart Team
The pre-operative data was subjected to MA, AAA and AAB, executed by the Heart Team, led by the Operating Surgeon. The degrees of membership, utilized in MA, AAA and AAB are optimized to achieve minimal discrepancy from the “absolute” classification. The patients with degrees of membership to their subgroup less than 0.5 were declared outliers. A low threshold would produce larger, but less homogenous subgroups of patients. A high threshold would produce more homogenous, but smaller subgroups. The threshold of 0.5 is a suitable compromise between the objectives to have homogenous subgroups and have large subgroups. In a similar study, investigators may very well select a different threshold.
Any patient, classified by either step 6 of MA, or step 3 and 6 in AAA, or steps 4 and 7 in AAB turned out to be an outlier. This is an excellent result since even the Heart Team could not reach consensus on the classification of such patients. Such patients are 13 in total in the study. The algorithms defined a total of 18 additional outliers. There was no discrepancy between the fuzzy algorithm results and the “absolute” classification.
The MA was applied on the overall sample of 140 patients. Of those, 71 were classified in A, and 69 were classified in B. The degrees of membership to A or B (
The AAA was applied on the sample of 71 patients classified in A. Of those, 29 were classified in A1 and 42 in A2. The conditional degrees of membership to A1 or A2 (
The AAB was applied on the sample of 69 patients classified in B. Of those, 36 were classified in B1 and 33 in B2. The conditional degrees of membership to B1 or B2 (
The 29 patients classified in group A1 were additionally denoted with local subgroup indices—(A1,1), (A1,2), …, (A1,29). AAA classified the 29 patients in subgroup A1 as follows: 4 were classified in step 1, 1 in step 2, none in step 3, 14 in step 4, 9 in step 5 and 1 in step 6. The mean degree of membership to subgroup A1 was 0.653. Of those patients, 5 belong to subgroup A1 with degree of membership lower than 0.5 (
The remaining data forms a fuzzy sample for A1 of 24 patients with mean degree of membership:
The mean degree of membership to subgroup A1 is:
The 42 patients classified in group A2 were additionally denoted with local subgroup indices—(A2,1), (A2,2), …, (A2,42). AAA classified the 42 patients in subgroup A2 as follows: 8 were classified in step 1, 12 in step 2, none in step 3, 9 in step 4, 10 in step 5 and 3 in step 6. Of those patients, 10 belong to subgroup A2 with degree of membership lower than 0.5
The remaining data forms a fuzzy sample for A2 of 32 patients with mean degree of membership:
The mean degree of membership to subgroup A2 is:
The 36 patients classified in subgroup B1 were additionally denoted with local subgroup indices—(B1,1), (B1,2), …, (B1,36). AAB classified the 36 patients in subgroup B1 as follows: 11 were classified in step 2, 10 in step 3, none in step 4, 15 in step 5, none in step 6 and none in step 7. Of those patients, 5 belong to subgroup B1 with degree of membership lower than 0.5
The remaining data forms a fuzzy sample for B1 of 31 patients with mean degree of membership:
The mean degree of membership to subgroup B1 is:
The 33 patients classified in subgroup B2 were additionally denoted with local subgroup indices—(B2,1), (B2,2), …, (B2,33). AAB classified the 33 patients in subgroup B2 as follows: 8 were classified in step 1, 2 in step 2, 13 in step 3, 3 in step 4, none in step 5, 7 in step 6 and none in step 7. Of those patients, 11 belong to subgroup B2 with degree of membership lower than 0.5
The remaining data forms a fuzzy sample for B2 of 22 patients with mean degree of membership:
The mean degree of membership to subgroup B2 is:
The MA has classified the 71 patients from group A as follows: 25 were classified in step 2, 16 in step 4, 26 in step 5 and 4 in step 6. The mean degree of membership to their subgroup is:
Of those patients, 15 (5 from subgroup A1 and 10 from subgroup A2) were declared outliers since the respective degree of membership to their subgroups was lower than 0.5
The remaining data forms a fuzzy sample for A of 56 patients with mean degree of membership calculated as:
The MA has classified the 69 patients from group B as follows: 8 were classified in step 1, 22 in step 3, 21 in step 4, 14 in step 5 and 4 in step 6. The mean degree of membership to their subgroup is:
Of those patients, 16 (5 from subgroup B1 and 11 from subgroup B2) were declared outliers since the respective degree of membership to their subgroups was lower than 0.5
The remaining data forms a fuzzy sample for B of 53 patients with mean degree of membership:
For example, a patient with identification number 34 was classified in group A by step 4 of MA. Hence, the degree of membership to group A is
As another example, a patient with identification number 110 was classified in group B by step 5 of MA. Hence, the degree of membership to group B is
6.3. Forming Fuzzy Samples
The degrees of membership discussed in section 6.2 are a characteristic of the patient hence they can be assigned to the values of any of the 68 parameters measured for each patient. So, once the degrees of membership are identified, we can form various fuzzy samples for any of the 68 parameters, recorded for each patient in the database (see section 6.1).
For example, let's analyse the LVEDVi measured before operation (pre-operative) for all patients classified in subgroup B2. We shall form two fuzzy samples—one for the 22 non-outlier patients whose
To assess the impact of the MVRepair we need to compare the following pairs of fuzzy samples: a) for each medical parameter (the original 68 excluding the identificators) for subgroups A1 and B1; b) for each medical parameter for subgroups A2 and B2; c) for each tripled parameter measured before and late after operation for a given subgroup; d) for each tripled parameter measured before and early after operation for a given subgroup.
All these fuzzy samples can be constructed as demonstrated above. The same approach is valid for any of the medical parameters, regardless of whether the parameter is discrete or continuous. A discussion on fuzzy samples as utilized here can be found in Ref. [16].
6.4. Comparison with Other Classifiers
To demonstrate the advantages of the proposed techniques, in this section we subject our data to other known classification techniques.
We constructed 8 classifiers, denoted from C1 to C8. All classifiers are Bayesian [27] with equal priors and they classify patients into one of four classes—A1, A2, B1 or B2. When the maximum posterior probability is under 50%, the patient is considered an outlier from either A or B depending on the class with maximum posterior probability.
The resubstitution errors [28] of those classifiers are derived using a testing sample of 140 patients, distributed as follows—24 in A1, 32 in A2, 31 in B1 and 22 in B2, with 15 outliers from group A and 16 outliers from group B (see section 6.1 for reference on those allocations). We use the resubstitution error as it is the easiest to calculate, it has excellent variance and slight optimistic bias, which is a good basis for comparison with better algorithms.
Classifiers C1 and C2 work with 14 discrete features (see Refs. [29,30]) and 12 independent continuous features (see Refs. [30,31]). Classifiers from C3 to C8 use 14 discrete features and 12 multinormal continuous features. The latter six classifiers reject classification of any patient in the test sample that has missing data in the multinormal continuous features. Let us denote such patients as rejected patients.
The learning samples of C1, C3, C4 and C5 consist of both typical and outlier patients distributed into A1, A2, B1 and B2 respectively as 29, 42, 36 and 33. The learning samples of C2, C6, C7 and C8 consist only of typical patients in each class, respectively 24, 32, 31 and 22 in A1, A2, B1 and B2.
Classifiers C3 and C6 are quadratic and use separate covariance matrix for each class. Classifiers C4, C5, C7 and C8 are linear and use a unified covariance matrix for all classes. For C4 and C7, the unified covariance matrix is calculated as the mean from the four covariance matrices of the classes weighted by the number of observations in each class in the learning sample. For C5 and C8, the unified covariance matrix is calculated as the mean from the four covariance matrices of the classes.
If any patient is classified as an outlier, her/his characteristics would not influence those of the subgroup. Therefore, the classification in A1/A2, and B1/B2 is not an issue. However, for such a patient it is important to define the classification to either A or B (as it defines the type of operation and hence it is of great importance for the patient). That is why the performance estimation of each classifier is formalized in a modified confusion matrix [28] given in Table 1 through Table 8.
| Classified |
||||||||
|---|---|---|---|---|---|---|---|---|
| A1 | A2 | B1 | B2 | Outliers in A | Outliers in B | Rejected | ||
| True (No.) | A1 (24) | 18 | 5 | 1 | 0 | 0 | 0 | 0 |
| A2 (32) | 3 | 29 | 0 | 0 | 0 | 0 | 0 | |
| B1 (31) | 1 | 0 | 29 | 1 | 0 | 0 | 0 | |
| B2 (22) | 1 | 0 | 4 | 17 | 0 | 0 | 0 | |
| Outliers A (15) | 10 | 4 | 0 | 1 | 0 | 0 | 0 | |
| Outliers B (16) | 1 | 0 | 2 | 12 | 0 | 1 | 0 | |
Modified confusion matrix for C1.
| Classified |
||||||||
|---|---|---|---|---|---|---|---|---|
| A1 | A2 | B1 | B2 | Outliers in A | Outliers in B | Rejected | ||
| True (No.) | A1 (24) | 20 | 4 | 0 | 0 | 0 | 0 | 0 |
| A2 (32) | 4 | 28 | 0 | 0 | 0 | 0 | 0 | |
| B1 (31) | 1 | 0 | 27 | 3 | 0 | 0 | 0 | |
| B2 (22) | 1 | 0 | 1 | 20 | 0 | 0 | 0 | |
| Outliers A (15) | 11 | 3 | 0 | 1 | 0 | 0 | 0 | |
| Outliers B (16) | 6 | 1 | 4 | 4 | 0 | 1 | 0 | |
Modified confusion matrix for C2.
| Classified |
||||||||
|---|---|---|---|---|---|---|---|---|
| A1 | A2 | B1 | B2 | Outliers in A | Outliers in B | Rejected | ||
| True (No.) | A1 (24) | 21 | 2 | 0 | 0 | 0 | 0 | 1 |
| A2 (32) | 1 | 30 | 0 | 0 | 0 | 0 | 1 | |
| B1 (31) | 0 | 0 | 27 | 3 | 0 | 0 | 1 | |
| B2 (22) | 1 | 1 | 0 | 19 | 0 | 0 | 1 | |
| Outliers A (15) | 3 | 9 | 0 | 0 | 0 | 0 | 3 | |
| Outliers B (16) | 2 | 2 | 2 | 7 | 0 | 0 | 3 | |
Modified confusion matrix for C3.
| Classified |
||||||||
|---|---|---|---|---|---|---|---|---|
| A1 | A2 | B1 | B2 | Outliers in A | Outliers in B | Rejected | ||
| True (No.) | A1 (24) | 22 | 1 | 0 | 0 | 0 | 0 | 1 |
| A2 (32) | 2 | 27 | 0 | 1 | 1 | 0 | 1 | |
| B1 (31) | 0 | 0 | 27 | 2 | 1 | 0 | 1 | |
| B2 (22) | 1 | 0 | 1 | 19 | 0 | 0 | 1 | |
| Outliers A (15) | 6 | 6 | 0 | 0 | 0 | 0 | 3 | |
| Outliers B (16) | 1 | 0 | 5 | 6 | 0 | 1 | 3 | |
Modified confusion matrix for C4.
| Classified |
||||||||
|---|---|---|---|---|---|---|---|---|
| A1 | A2 | B1 | B2 | Outliers in A | Outliers in B | Rejected | ||
| True (No.) | A1 (24) | 22 | 1 | 0 | 0 | 0 | 0 | 1 |
| A2 (32) | 2 | 26 | 0 | 1 | 2 | 0 | 1 | |
| B1 (31) | 0 | 0 | 27 | 2 | 1 | 0 | 1 | |
| B2 (22) | 1 | 0 | 1 | 19 | 0 | 0 | 1 | |
| Outliers A (15) | 6 | 6 | 0 | 0 | 0 | 0 | 3 | |
| Outliers B (16) | 1 | 0 | 5 | 6 | 0 | 1 | 3 | |
Modified confusion matrix for C5.
| Classified |
||||||||
|---|---|---|---|---|---|---|---|---|
| A1 | A2 | B1 | B2 | Outliers in A | Outliers in B | Rejected | ||
| True (No.) | A1 (24) | 22 | 1 | 0 | 0 | 0 | 0 | 1 |
| A2 (32) | 1 | 30 | 0 | 0 | 0 | 0 | 1 | |
| B1 (31) | 0 | 0 | 27 | 3 | 0 | 0 | 1 | |
| B2 (22) | 1 | 0 | 0 | 20 | 0 | 0 | 1 | |
| Outliers A (15) | 6 | 6 | 0 | 0 | 0 | 0 | 3 | |
| Outliers B (16) | 4 | 2 | 4 | 3 | 0 | 0 | 3 | |
Modified confusion matrix for C6.
| Classified |
||||||||
|---|---|---|---|---|---|---|---|---|
| A1 | A2 | B1 | B2 | Outliers in A | Outliers in B | Rejected | ||
| True (No.) | A1 (24) | 22 | 0 | 1 | 0 | 0 | 0 | 1 |
| A2 (32) | 3 | 27 | 0 | 0 | 0 | 1 | 1 | |
| B1 (31) | 0 | 0 | 28 | 2 | 0 | 0 | 1 | |
| B2 (22) | 1 | 0 | 0 | 20 | 0 | 0 | 1 | |
| Outliers A (15) | 9 | 3 | 0 | 0 | 0 | 0 | 3 | |
| Outliers B (16) | 2 | 1 | 4 | 5 | 0 | 1 | 3 | |
Modified confusion matrix for C7.
| Classified |
||||||||
|---|---|---|---|---|---|---|---|---|
| A1 | A2 | B1 | B2 | Outliers in A | Outliers in B | Rejected | ||
| True (No.) | A1 (24) | 22 | 0 | 1 | 0 | 0 | 0 | 1 |
| A2 (32) | 2 | 28 | 0 | 0 | 0 | 1 | 1 | |
| B1 (31) | 0 | 0 | 28 | 2 | 0 | 0 | 1 | |
| B2 (22) | 1 | 0 | 0 | 20 | 0 | 0 | 1 | |
| Outliers A (15) | 9 | 3 | 0 | 0 | 0 | 0 | 3 | |
| Outliers B (16) | 2 | 1 | 4 | 5 | 0 | 1 | 3 | |
Modified confusion matrix for C8.
In Table 9 we give the modified confusion matrix for the crisp algorithm, advised in Refs. [13,14]. Table 10 gives the modified confusion matrix for the fuzzy algorithms presented in this paper.
| Classified |
||||||||
|---|---|---|---|---|---|---|---|---|
| A1 | A2 | B1 | B2 | Outliers in A | Outliers in B | Rejected | ||
| True (No.) | A1 (24) | 24 | 0 | 0 | 0 | 0 | 0 | 0 |
| A2 (32) | 0 | 32 | 0 | 0 | 0 | 0 | 0 | |
| B1 (31) | 0 | 0 | 31 | 0 | 0 | 0 | 0 | |
| B2 (22) | 0 | 0 | 0 | 22 | 0 | 0 | 0 | |
| Outliers A (15) | 7 | 7 | 1 | 0 | 0 | 0 | 0 | |
| Outliers B (16) | 0 | 2 | 6 | 8 | 0 | 0 | 0 | |
Modified confusion matrix for the crisp algorithms.
| Classified |
||||||||
|---|---|---|---|---|---|---|---|---|
| A1 | A2 | B1 | B2 | Outliers in A | Outliers in B | Rejected | ||
| True (No.) | A1 (24) | 24 | 0 | 0 | 0 | 0 | 0 | 0 |
| A2 (32) | 0 | 32 | 0 | 0 | 0 | 0 | 0 | |
| B1 (31) | 0 | 0 | 31 | 0 | 0 | 0 | 0 | |
| B2 (22) | 0 | 0 | 0 | 22 | 0 | 0 | 0 | |
| Outliers A (15) | 0 | 0 | 0 | 0 | 15 | 0 | 0 | |
| Outliers B (16) | 0 | 0 | 0 | 0 | 0 | 16 | 0 | |
Modified confusion matrix for the fuzzy algorithms.
To summarize the information from the modified confusion matrices, we introduce four criteria: 1) K1—the percentage of the non-rejected patients; 2) K2 —the percentage of the correctly classified patients out of all non-rejected typical patients; 3) K3—the percentage of the patients correctly classified as outliers from group A or outliers from group B out of the non-rejected outlier patients; 4) K4—the percentage of the patients correctly classified (either as typical or outlier patients) in group A or in group B out of the non-rejected outlier patients.
The resulting values of those criteria for C1 through C8, the crisp and the fuzzy algorithms are given in Table 11.
| C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | crisp | fuzzy | |
|---|---|---|---|---|---|---|---|---|---|---|
| K1 | 100 | 100 | 93 | 93 | 93 | 93 | 93 | 93 | 100 | 100 |
| K2 | 86 | 87 | 92 | 90 | 90 | 94 | 92 | 93 | 100 | 100 |
| K3 | 3 | 3 | 0 | 4 | 4 | 0 | 4 | 4 | 0 | 100 |
| K4 | 94 | 74 | 84 | 96 | 96 | 76 | 88 | 88 | 90 | 100 |
Values (in %) of the performance criteria for classifiers C1 to C8, the crisp and the fuzzy algorithms.
A serious drawback of six of the Bayesian classifiers is the 7% of rejected patients that are not classified (see first row of Table 11). Another drawback of all Bayesian classifiers is that between 6% and 14% of typical patients are not correctly classified (see K2 in second row of Table 11). A third drawback of the Bayesian classifiers and the crisp algorithm is that between 4% and 26% of outlier patients are not assigned the right treatment (see K4 in fourth row of Table 11). However, the main problem of all Bayesian classifiers as well as the crisp algorithm is their extremely poor outlier detection (K3 is between 0% and 4% in the third row of Table 11). This creates difficulties when assessing the characteristics of the subgroups. The fuzzy algorithms (last column of Table 11) show excellent differentiation of typical patients and outliers. On top, the fuzzy algorithms are the only approach that provides a measure of how typical a patient is to its subgroup. Hence, this measure should be used as weight coefficient when obtaining the subgroup characteristics.
The Bayesian classifiers as a whole differ from both the crisp and the fuzzy algorithms in another important, though non-numerical, aspect. The Heart Team has an explicit role in the application of the algorithms and no role at all in the Bayesian classifiers. Evidently the Heart Team will be much more comfortable with the results they engaged with, especially having in mind that those results provide at least partial explanation as to why patients were classified in a given subgroup.
7. DISCUSSION
As mentioned earlier, the degrees of membership used for the fuzzy algorithms were optimized to reach minimum discrepancy with the “absolute” classification. Other research teams may decide to use a different approach when identifying the degrees of membership. The proposed procedures will still be valid and based on the different degrees of membership they will produce different stratification of patients to groups and subgroups hence a different recommendation for treatment.
When stratification is concerned, other practitioners may decide to stratify patients into three or more subgroups to improve the homogeneity of the subgroup samples. This approach would be adequate when a larger initial sample is available. For the sake of the current study, the research team has decided that four subgroups are a proper balance between the achieved homogeneity in the subgroups and the size of the resulting subgroup samples (which in turn influences the precision of further statistical inferences made based on the data).
Strictly speaking, every patient belongs to the four fuzzy subgroups and theoretically speaking all those four degrees of membership could be calculated, and their sum would be one. By calculating the four degrees of membership we would complete a fuzzy partition of the patients into the four subgroups [22]. This is not the approach chosen in this paper. Instead, the algorithms proposed here calculate only the maximal of those four coefficients, which pre-defines the classification of the patient to a given subgroup. Furthermore—if the maximum is less than 0.5, then the patient is considered an outlier and does not participate in subsequent calculations. The objective is to assess more adequately the characteristics of the subgroup. For example, if a patient has a degree of membership to a given subgroup of 35%, then the influence of her/his characteristics over the characteristics of the subgroup is noise rather than an actual contribution to improve adequacy of the subgroup description. Other approaches are also possible, for example to analyse all patients classified in a given subgroup regardless of how low their degree of membership is, if it is the maximum possible.
Alternatively, all patients (regardless of where they are classified into) may take part in the formation of the characteristics of all four groups. It is known that
A fuzzy algorithm for homogenizing stratification of patients from group A, if they were classified in group B into two subgroups: with comparatively preserved status (subgroup B1) and with comparatively damaged status (subgroup B2)
A fuzzy algorithm for homogenizing stratification of patients from group B, if they were classified in group A into two subgroups: with comparatively preserved status (subgroup A1) and with comparatively damaged status (subgroup A2)
Developing those algorithms will be a real challenge since there is no medical practice to apply such algorithms.
In our context, we consider the groups A and B, and the subgroups A1, A2, B1 and B2 as fuzzy, so we find the degrees of membership. By doing so, we used the physical interpretation of fuzzy data in experiments with uncertain outcome [32]. Another epistemic interpretation of our fuzzy data is also possible [33], where those groups are considered crisp sets. Then the values of
In our paper, the concept of classical fuzzy sets was suitable enough to stratify patients into subgroups and identify outliers. However, other similar studies may require the use of more complex tools. When the available medical information is not complete or is uncertain, the intuitionistic fuzzy sets [39] can improve the way patients are classified into suitable subgroups. On the other hand, if the data is indeterminate and inconsistent, then the Pythagorean fuzzy sets [40] and the neutrosophic sets [41] provide a promising alternative to model the classification process more adequately.
8. CONCLUSIONS
This paper applied intelligent methods to solve medical treatment problems. Intelligent systems, as part of artificial intelligence, are long overdue in this subject area, but lately their implementation in medical practice has increased [42,43]. We used fuzzy set theory to a traditional medical uncertainty problem for selection of surgical treatment and for homogenizing stratification of patients with IMR, which traditionally was solved with non-fuzzy data. This is in line with the fourth purpose to use fuzzy techniques [44].
We presented the structure and medical justification of three fuzzy algorithms for selection of surgical treatment and for homogenizing stratification of patients with IMR. The first one (MA) classified a patient into the fuzzy groups A or B by identification of the respective degree of membership
To calculate the degree of membership to the subgroup for each patient, we utilized the product t-norm to find the membership degree to the fuzzy subgroups as an intersection of two fuzzy sets. As claimed in Ref. [15], since fuzzy intersection is not a unique operation, contrary to its crisp counterpart, different functions may be appropriate to represent this operation in different context. That is why our choice to use the product t-norm to calculate
All described procedures were implemented over the data for 140 patients with IHD complicated with IMR [13,14]. We also demonstrated how to form fuzzy samples for any of the medical parameters recorded for the 140 patients. Further in our experimental findings, we constructed eight classifiers and applied them over the same data. The performance estimation of the classifiers (allocations to groups, subgroups and typical/outlier patients) was made using four new criteria. Our fuzzy algorithms performed best in terms of their ability to identify outliers and the ability to allocate patients into their true group.
CONFLICT OF INTEREST
The authors have no affiliation with any organization with a direct or indirect financial interest in the subject matter discussed in the manuscript
The authors have no perceived or potential conflict of interest to declare with regards to the research and content of the above mentioned manuscript
AUTHORS' CONTRIBUTIONS
The medical component of this manuscript has been developed by the co-authors Plamen Panayotov and Daniela Panayotova, who contributed equally to this component
The computational and informatics component of this manuscript have been developed by the co-authors Natalia Nikolova, Snejana Ivanova and Kiril Tenekedjiev, who contributed equally to this component
All authors have participated in: (a) drafting the article or revising it critically for important intellectual content; (b) approval of the final version.
Funding Statement
The authors declare that the above-mentioned manuscript has not received or utilized any research or other funding.
REFERENCES
Cite this article
TY - JOUR AU - Natalia Nikolova AU - Plamen Panayotov AU - Daniela Panayotova AU - Snejana Ivanova AU - Kiril Tenekedjiev PY - 2019 DA - 2019/10/01 TI - Using Fuzzy Sets in Surgical Treatment Selection and Homogenizing Stratification of Patients with Significant Chronic Ischemic Mitral Regurgitation JO - International Journal of Computational Intelligence Systems SP - 1075 EP - 1090 VL - 12 IS - 2 SN - 1875-6883 UR - https://doi.org/10.2991/ijcis.d.190923.002 DO - 10.2991/ijcis.d.190923.002 ID - Nikolova2019 ER -