
Abdominal aortic size and volume by computed tomography angiography in population of Ukraine: Normal values by age, gender, and body surface area
- DOI
- 10.1016/j.artres.2017.10.197How to use a DOI?
- Keywords
- Infrarenal aortic size; Abdominal aortic aneurism; Aortic diseases; Computed tomography angiography
- Abstract
Background: Computed tomography angiography (CTA) is a standard tool for investigation of the abdominal aorta diseases. Currently, there are only a few published scientific articles devoted to the study of the infrarenal aortic size without pathology. The aim of the current work was to examine the indicators of size and volume of the infrarenal aorta and investigate their dependence on the body surface area, body mass index (BMI) and age in patients without aortic diseases.
Methods: We analyzed 94 patients without the diseases of the abdominal cavity, who underwent computed tomography angiography. There were 36 men (38,3%), the average age of the participants was 52,9 ± 15,4 years. All patients underwent CTA of the aorta with contrast-enhanced arterial phase.
Results: In 94 patients the average diameter of the IA was 18,2 ± 2,7 mm, volume – 21,0 ± 6,65 cm3, and length – 96,6 ± 10,6 mm. This study uncovered a significant strong correlation between the body surface area and the diameter/volume of the IA aorta. There was no relationship between the length of the aorta, and anthropometric data.
Conclusions: We discovered a significant strong correlation between age, body surface area with the diameter and volume of the aorta. In all cases, there was no relationship between the length of the aorta, and anthropometric data. There was a significant difference in infrarenal aorta diameter and volume between men and women. The significant positive correlation between the body surface area, BMI and the diameter/volume of the IA was detected only in women.
- Copyright
- © 2017 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Nowadays Computed Tomography Angiography (CTA) is one of the main noninvasive medical test that provide detailed information about the aorta and its branches, this is due to the fact that the method is highly informative, reliable and safe.
Currently, only a few published articles are devoted to the study of the infrarenal aortic size without pathology.1 The relevance of investigation of these indicators comes from the dependence of changes in aortic measurements on the anthropometric indicators, such as age and other risk factors for the development of aneurysms of the infrarenal aorta (IA).2
The determination of the aneurysmal sac became used recently. The method of determining the volume of the aneurysmal expansion may play a key role in the observation on small abdominal aneurysms and follow-up of endovascular repair of abdominal aortic aneurism.3–5
The aim of this study was to investigate the indicators of size and volume of the IA and their dependence on the body surface area, body mass index and age in patients not suffering from aortic diseases.
Methods
The inclusion criteria for this study was having undergone a CTA of abdominal aorta for diseases not associated with vascular pathology. The exclusion criteria were presence of aortic diseases of any genesis and history of any reconstructive operations on the aorta.
We analyzed data from 94 patients, who underwent CTA with contrast-enhanced arterial phase over the diseases of the abdominal cavity. There were 36 (38,3%) men in the study and the average age of the participants was 52,9 ± 15,4 years (ranging from 14 to 85). Average weight was 74,8 ± 17,0 kg, height – 167,6 ± 8,4 cm, body mass index – 26,5 ± 5,9 kg/m2, body surface area – 1,84 ± 0,22 m2.
All patients underwent CTA of the aorta with contrast-enhanced arterial phase. The study was conducted on a 64-detector – GE Optima 660, equipped with a synchronized injector. These axial sections were processed on the workstation AW Volume Share 5. Automatic bolus tracking system for arterial phase was used. Then, on the workstation 660 GE Optima, with help of the preinstalled software, the indicators of aortic volume in cm3, the maximum diameter of the aorta and its length in millimeters (mm) was calculated. In order to accurately determine the IA volume, kidney artery was chosen as a start point of calculations and the aortic bifurcation was used as the end point (Fig. 1).
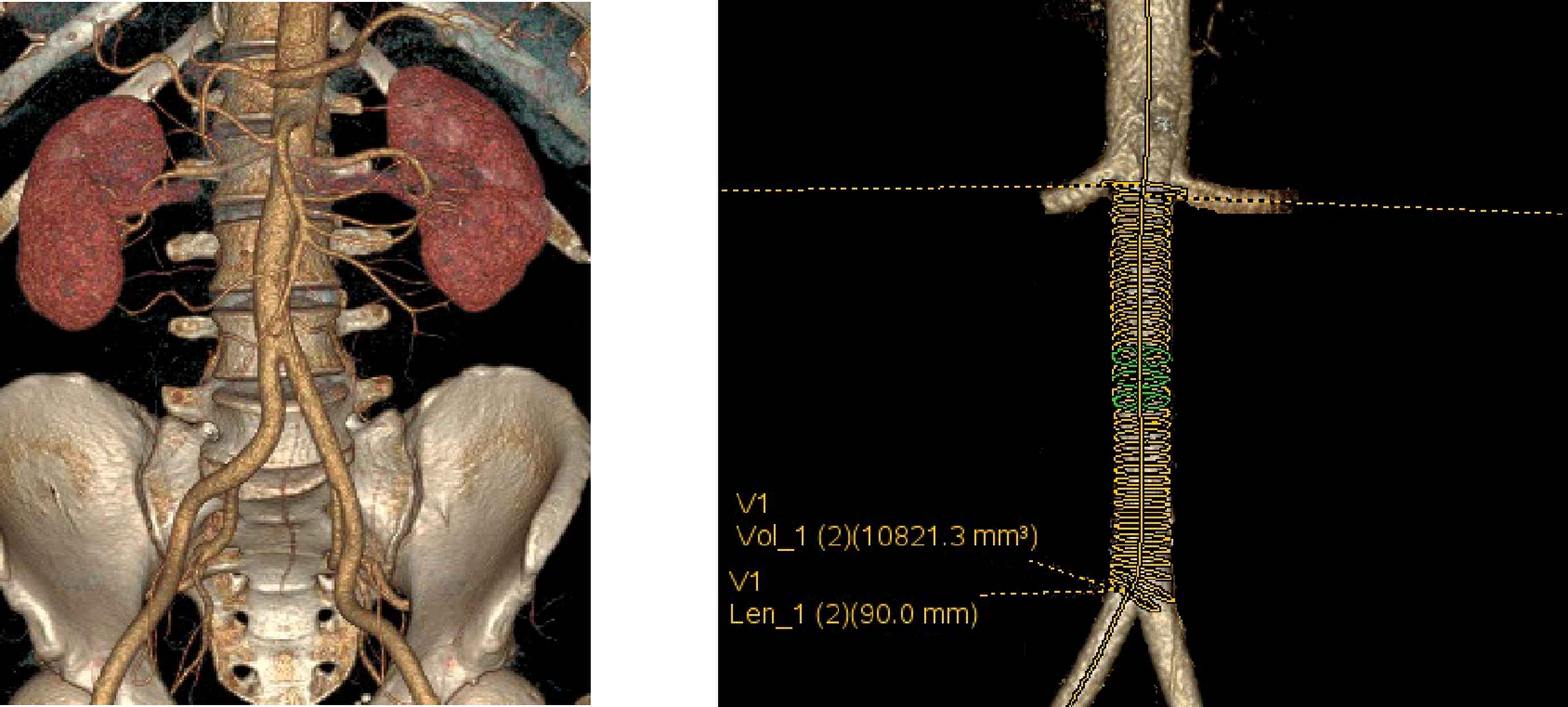
CTA, 3D reconstruction of the aorta. Technique of measuring the length and volume of the infrarenal aorta.
All analyses were performed using the Statistica program “STATISTICA 7,0” for Windows (StatSoft. Inc., USA). Values are expressed as means ± standard deviation (SD). Pearson test was performed to evaluate associations between the selected variables. The estimated parameters were considered significant at p < 0,05. Significant correlation was evaluated as ‘strong’ from ±0,7 up to ±1; ‘average’ from ±0,3 up to ±0,699; and ‘weak’ 0 to ±0,299.
Results
In 94 patients the average diameter of the IA was 18,2 ± 2,7 mm, volume – 21,0 ± 6,65 cm3, and length – 96,6 ± 10,6 mm. On the basis of this measurement, aortic size analysis regarding gender, age and other selected factors was performed (Table 1). There were significant differences in the body surface area, the diameter of the IA and its volume among men and women.
| Men (n = 36) | Women (n = 58) | |
|---|---|---|
| Age (years) | 59,4 ± 13,2 | 55,1 ± 10,7 |
| Weight (kg) | 86,5 ± 24,9 | 74,6 ± 16,6 |
| Body surface area (m2) | 1,97 ± 0,21a | 1,83 ± 0,2a |
| BMI (kg/m2) | 26,2 ± 5,4 | 27,5 ± 6,5 |
| Volume of the IA (sm3) | 25,7 ± 6,4a | 19,6 ± 4,9a |
| Length of the IA (mm) | 99,4 ± 11,2 | 95,8 ± 9,8 |
| Diameter of the IA (mm) | 19,7 ± 2,2a | 17,9 ± 2,3a |
p < 0,05 (t-test).
The results of patient examination.
It is worth noting the length of the IA. This index not change and was not affected by patient’s gender, age (r = 0,12, p = 0,25), body mass index (r = −0,02, p = 0,84) or body surface area (r = 0,07, p = 0,57). However, there was a weak correlation with the volume and diameter of the IA.
Analysis of the data has established a significant strong correlation between the age and the diameter/volume of the aorta. It was noted that with the increase in age, there was an increase in the diameter of the IA and IA volume (Fig. 2). Moreover, the increase in diameter of the aorta was identified in both men (r = 0,56, p < 0,05) and women (r = 0,54, p < 0,05).
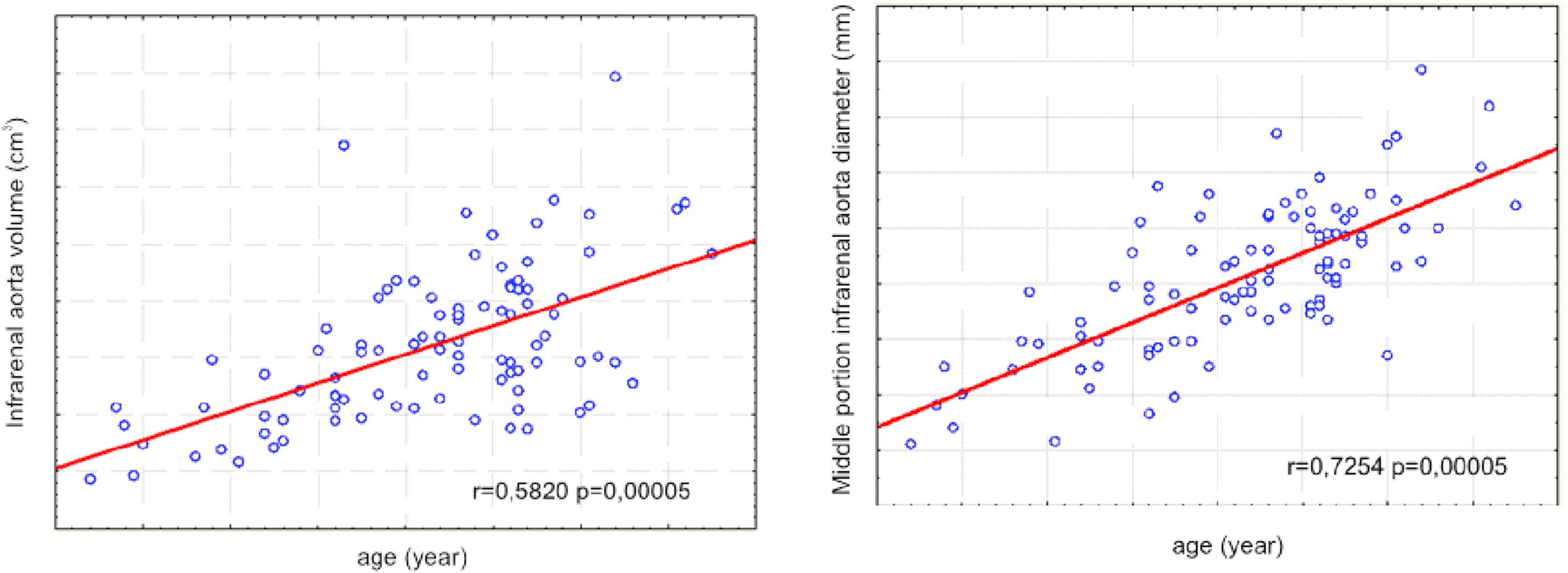
Graph of scattering (IA volume, IA diameter and age of patients, n = 94).
We analyzed BMI with respect to the diameter and volume of the aorta (Fig. 3). There was a significant correlation of the medium strength, which showed that with the increase in BMI there was an increase in the diameter (r = 0,4, p = 0,0007) and volume of IA (r = 0,3, p = 0,004).
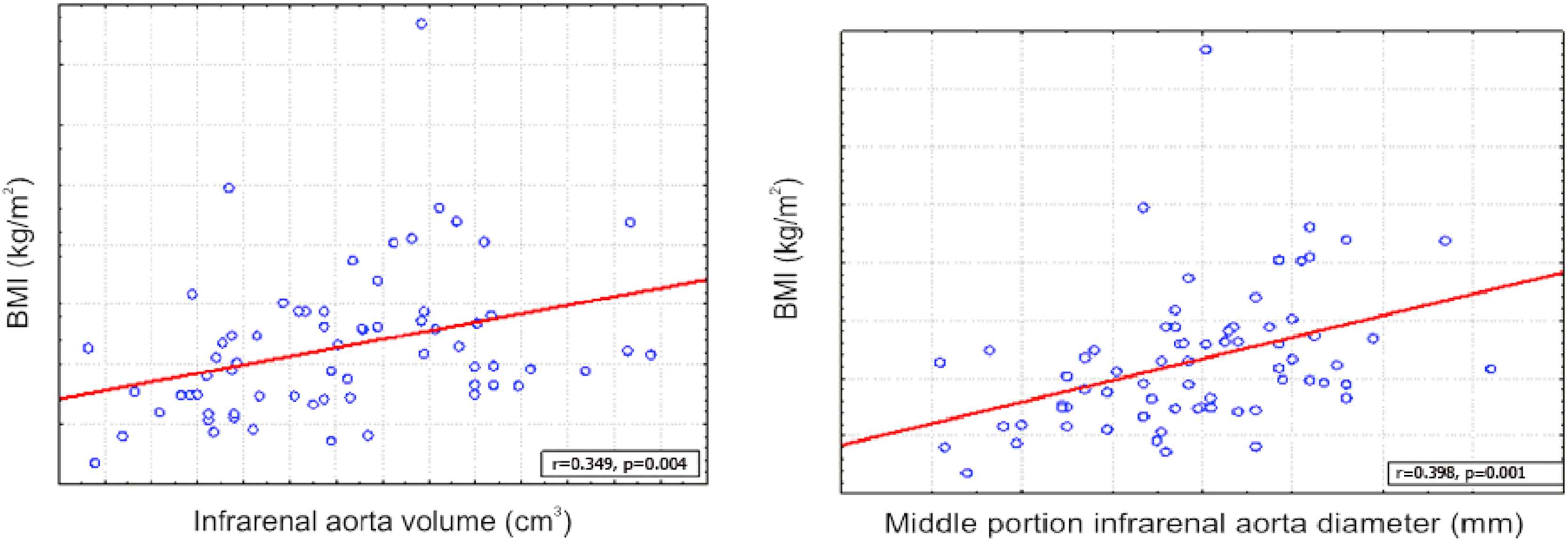
Graph of scattering (IA volume diameter and diameter of IA and BMI of patients, n = 94).
This study uncovered a significant strong correlation between the body surface area and the diameter/volume of the IA aorta (r = 0,54, p < 0,05). That meant that increasing the body surface area caused a significant increase in the diameter and volume of the IA (Fig. 4), however the correlation between BMI and diameter/volume of the aorta was weak (r = 0,3, p < 0,05). This may indicate that an increase in aortic diameter depends on body surface area, but not BMI.
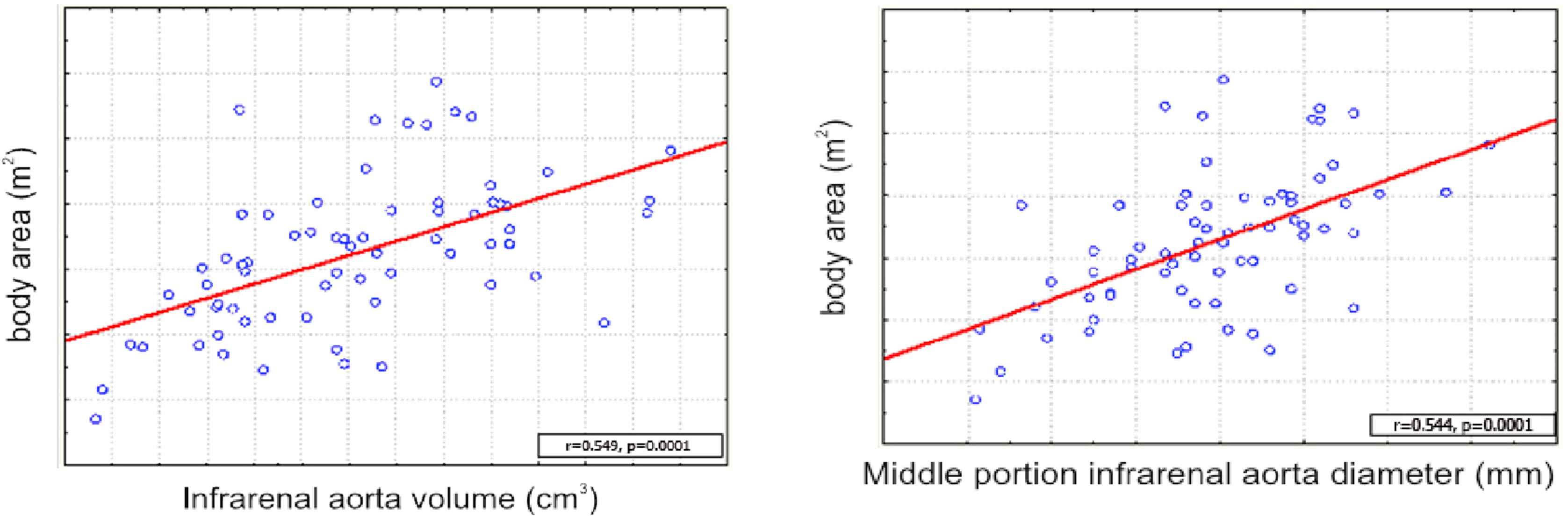
Graph of scattering (body surface area and volume/diameter of the IA, n = 94).
There was no relationship between the length of the aorta, and anthropometric data (height, BMI, body surface area), in all cases r < 0,01, p > 0,05 (see Table 2).
| Diameter of the IA | Volume of the IA | Length of the IA | |
|---|---|---|---|
| Age | strong | strong | NC |
| Body surface area | strong | strong | NC |
| BMI | average | average | NC |
The correlations between anthropometric data and aortic CTA measurements (NC: no correlation).
According to the goal of the study, we analyzed the correlation between anthropometric data (height, BMI, body surface area) and indicators of size and volume of the IA in men and women separately (Table 3).
| Men | Women | p | |
|---|---|---|---|
| Age/IA volume | Strong | Average | 0,334 |
| Age/length of the IA | NC | NC | |
| Age/diameter of IA | Strong | Strong | 0,888 |
| Weight/IA volume | NC | Strong | 0,000 |
| Weight/length of the IA | NC | NC | |
| Weight/diameter of IA | NC | Average | 0,000 |
| Height/IA volume | Average | NC | 0,000 |
| Height/length of the IA | NC | NC | |
| Height/diameter of IA | NC | NC | |
| Body surface area/IA volume | Average | Average | 0,656 |
| Body surface area/length of the IA | NC | NC | |
| Body surface area/diameter of IA | Strong | Average | 0,097 |
| BMI/IA volume | NC | Average | 0,000 |
| BMI/length of the IA | NC | NC | |
| BMI/diameter of IA | NC | Average | 0,000 |
The correlations between anthropometric data and aortic CTA measurements in groups. (NC: no correlation).
Discussion
The result showed a significant difference in the body surface area among men and women (p < 0,05), where the men had higher body surface area. Table 1 shows that for the same length of the aorta in both men and women (p = 0,17, no difference in length), there was a significant difference in the diameter and volume of the IA in men (p < 0,05), and an increase in body surface area had a direct correlation with an increase in diameter aortic (r = 0,54, p < 0,05). This fact may confirm the tendency of higher occurrence of aneurysms in men. It is necessary to focus on the length of the aorta, which, as it has been shown, was not significantly different in the two groups and did not change and correlate with age and anthropometric measures. That leads to the conclusion that the IA has a length of 96,6 ± 2,2 mm and does not depend on gender, age, and height. The same significant differences were identified in the course of the studies in other countries.6,7 Weak correlation of BMI and the volume of the aorta or its diameter suggests an absence of connection between the obesity increase and the increasing of diameter and volume of the aorta, which also was mentioned in the works of other authors.8,10
The differences in correlation of men and women showed in Table 3. It was founded that the age is positively correlated with volume and diameter of the IA in both groups. However, the significant positive correlation between the body surface area, BMI and the diameter/volume of the IA was detected only in women. In our opinion weight gain in women can lead to an increase in the diameter and volume of the IA.
The analysis of total data shows that the most significant increase in the diameter of the aorta is associated with age (r = 0,72, p = 0,00005), a relationship that has been identified in other studies,9 and which suggests that the risk of aneurysms is increased in higher age categories. The difference in correlation uncovered from the aortic diameter measurements and its volume for age (Fig. 2), r = 0,72 and r = 0,58, respectively, appear to demonstrate the advantage of calculating the degree of “expansion” of the aorta by determining its volume, not the diameter, which may be a very important moment in the follow-up of small aneurysms or changes in the dynamics of the aneurysmal sac after the endovascular repair of abdominal aortic aneurism.
Conflicts of interest
None.
References
Cite this article
TY - JOUR AU - Andriy Nykonenko AU - Andrei Balyuta AU - Yevhen Haidarzhi AU - Yevgen Yermolayev AU - Ivan Pertsov AU - Olexandr Nykonenko PY - 2017 DA - 2017/11/01 TI - Abdominal aortic size and volume by computed tomography angiography in population of Ukraine: Normal values by age, gender, and body surface area JO - Artery Research SP - 22 EP - 26 VL - 20 IS - C SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2017.10.197 DO - 10.1016/j.artres.2017.10.197 ID - Nykonenko2017 ER -