
Distribution and determinants of tuberculosis in the Kingdom of Saudi Arabia from 2005 to 2012
- DOI
- 10.1016/j.jegh.2017.08.002How to use a DOI?
- Keywords
- Laboratory-confirmed tuberculosis; Saudi Arabia; Tuberculosis trends
- Abstract
Tuberculosis (TB) remains a public health threat in the Kingdom of Saudi Arabia (KSA) with many challenges that limit its prevention and control. To understand how to meet these challenges, this study calculated the TB incidence rates (IRs) in KSA from 2005 to 2012, which were stratified by nationality, sex, and administrative regions. Furthermore, laboratory capabilities were assessed by determining the proportion of laboratory-confirmed TB cases. The overall TB IRs decreased from 15.80/100,000 population in 2005 [95% confidence interval (CI) = 15.29–16.31] to 13.16/100,000 population in 2012 (95% CI = 12.74–13.58). The IRs were greater for males than for females from 2009 to 2012. The IRs of non-Saudis were approximately two times those of Saudis during the study period. Mecca had greater IR during the study period compared with other regions [25.13/100,000 (95% CI = 24.7–25.56)]. Among non-Saudis, those from Indonesia and Yemen had the greatest proportion of TB cases (15.4% and 12.9%, respectively). Individuals <15 years of age comprised 14.2% of the TB cases. Employed non-Saudis had the greatest proportion of TB (32%), followed by unemployed Saudis (22.38%). The proportion of laboratory-confirmed cases of reported TB was 57% from 2005 to 2012. For effective prevention and control, TB screening should be implemented for non-Saudi workers at ports of entry and laboratory-screening capacity for TB should be evaluated.
- Copyright
- © 2017 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Tuberculosis (TB) is a major public health threat with an estimated 9 million new cases per year and 2 million attributable deaths [1]. In 2014, TB ranked alongside human immunodeficiency virus (HIV) as the single most common cause of death among all other infectious diseases, with the number of deaths from TB surpassing that from HIV in the following years [2]. Reduction of TB infection rates is a Millennium Development Goal, but the infection remains a major public health problem. The World Health Organization (WHO) has recently released a strategy for the post-2015 era, which aims to end the global TB epidemic by 2035 [3].
The Kingdom of Saudi Arabia (KSA) is a fast-developing country that has experienced tremendous changes over the previous decades. By improving its standard of living, KSA has succeeded in minimizing infectious disease-related mortalities. With it rapid development, the country has become a major destination for many immigrants from developing countries who currently make up about one-third of the Saudi population [4]. In addition, 2–3 million pilgrims travel to KSA yearly to perform Hajj, mostly from developing countries. These factors have caused major shifts in the status of many infectious diseases and presented many challenges to KSA in controlling infectious diseases, including TB.
According to the Central Department of Statistics, KSA has a population of around 30 million. One-third of this population is composed of non-Saudi immigrants. The incidence rate (IR) for TB has ranged from 11/100,000/year to 16/100,000/year since 2000 [5]. From 1991 to 2010, 64,345 cases of TB were diagnosed in KSA [6]. Pulmonary TB, the infectious type, accounts for 73% of these cases [6]. Because of factors such as the high number of immigrants and pilgrims, TB is not fully controlled in KSA. The mortality rate among TB patients reached a peak in 2003 when it was reported to be 7.2% among Saudis and 6.2% among non-Saudis [7]. Since then, the incidence and mortality rates have decreased, but the problem persists.
TB remains a public health problem in KSA with many challenges that limit its control and elimination. Furthermore, no previous study has tried to assess the sensitivity of the TB screening program in KSA. In addition, previous studies on the trends of TB have focused only on sex, region, age group, and nationality (Saudi or non-Saudi). This study aims to investigate the trends of the IR of TB in KSA over an 8-year period (2005–2012) stratified by sex, nationality, and the 13 administrative regions. In addition, this study aims to identify the distribution of TB cases among age groups, occupation, and immigrant nationalities.
In this study, the reported laboratory results of TB tests were analyzed to determine which TB cases were confirmed based on WHO guidelines [8]. This helped us identify the capacity of the TB laboratory testing programs overall and by region. The results of this study demonstrated the need to perform a formal evaluation of the TB program in KSA.
2. Methods
TB is an infectious disease requiring mandatory reporting [4]. Surveillance for TB cases is population based and conducted in both primary health centers and hospitals [9]. All suspected TB cases were reported monthly to the Ministry of Health (MoH) from all KSA regions [6]. For suspected cases in health centers, the diagnosis can be confirmed using methods such as mycobacterial culture, sputum smear microscopy, radiography, histopathology, and molecular techniques [9]. However, the reported data contain only results from the laboratory tests of smear and culture, possibly because these options are more commonly available in all laboratories than other laboratory tests.
TB case data were obtained from the Saudi MoH as deidentified, individual-level data collected from 2005 to 2012. KSA has a national disease registry in which all reportable health conditions, including infectious diseases, are reported to the MoH [4]. This study’s data provided results from the culture, smear, and radiography analysis of each reported case.
This study estimated the IR and 95% confidence interval (CI) of TB for the population in KSA from 2005 to 2012 to investigate the trend of the IR over the study period. The IRs were estimated and stratified by nationality, sex, and administrative regions. IRs were estimated using the number of cases per year over the total population per 100,000 individuals.
Two population databases were used. The first was the Saudi Central Department of Statistics, whose data were used to estimate the IR for the total population and by nationality and sex. Because the population data stratified by region were not available in the Central Department of Statistics database, another database from the MoH was used to obtain the region-level data. Nationality was classified as Saudi or non-Saudi, and regions were grouped into the 13 administrative regions.
The proportion of TB cases was also calculated by nationality, age category, and employment status. Age was divided into categorical variables of 5-year duration. Employment status was grouped into four categories, namely, employed, unemployed, student, or prisoner. Because prisoners live in crowded conditions, and are therefore more susceptible to TB transmission, they were categorized separately. Students were also categorized separately because schools are usually crowded and can act as foci to spread the infection to the community.
This study also calculated the proportion of laboratory-confirmed cases of the reported TB cases for each region based on the WHO diagnostic criteria of confirming cases by either positive culture or smear [8]. All calculations and analysis were done using Excel 2013 (Microsoft, Redmond, WA, USA).
2.1. Ethical considerations
This study was determined to be Institutional Review Board exempt because all analyses were performed on secondary data deidentified prior to analysis. Prior to data collection, all portions of the study were reviewed by Emory University’s Institutional Review Board and determined to meet the criteria for exemption.
3. Results
The total number of TB cases included in this study that have been diagnosed between 2005 and 2012 was 32,435. The overall TB IR in KSA decreased from 2005 to 2012. The rate difference between 2005 (IR = 15.8; 95% CI = 15.29–16.31) and 2012 (IR = 13.16; 95% CI = 12.74–13.58) was statistically significant according to the CIs (Table 1).
| Year | N | IRa | 95% Confidence interval |
|---|---|---|---|
| 2005 | 3687 | 15.80 | 15.29–16.31 |
| 2006 | 3875 | 16.06 | 15.55–16.57 |
| 2007 | 4084 | 16.37 | 15.87–16.87 |
| 2008 | 4156 | 16.12 | 15.63–16.61 |
| 2009 | 4149 | 15.56 | 15.09–16.03 |
| 2010 | 4558 | 16.54 | 16.06–17.02 |
| 2011 | 4083 | 14.39 | 13.95–14.83 |
| 2012 | 3843 | 13.16 | 12.74–13.58 |
| Total | 32,435 |
IR = incidence rate per 100,000 population.
Reported cases of tuberculosis and incidence rates, by year, in the Kingdom of Saudi Arabia, from 2005 to 2012.
The TB IRs of both males and females were similar from 2005 to 2008 (Fig. 1); however, from 2009 to 2012, the IRs of males were higher than those of females. The IRs of non-Saudis were about two times those of Saudis during the study period (Fig. 1), although the IRs for both groups remained stable.
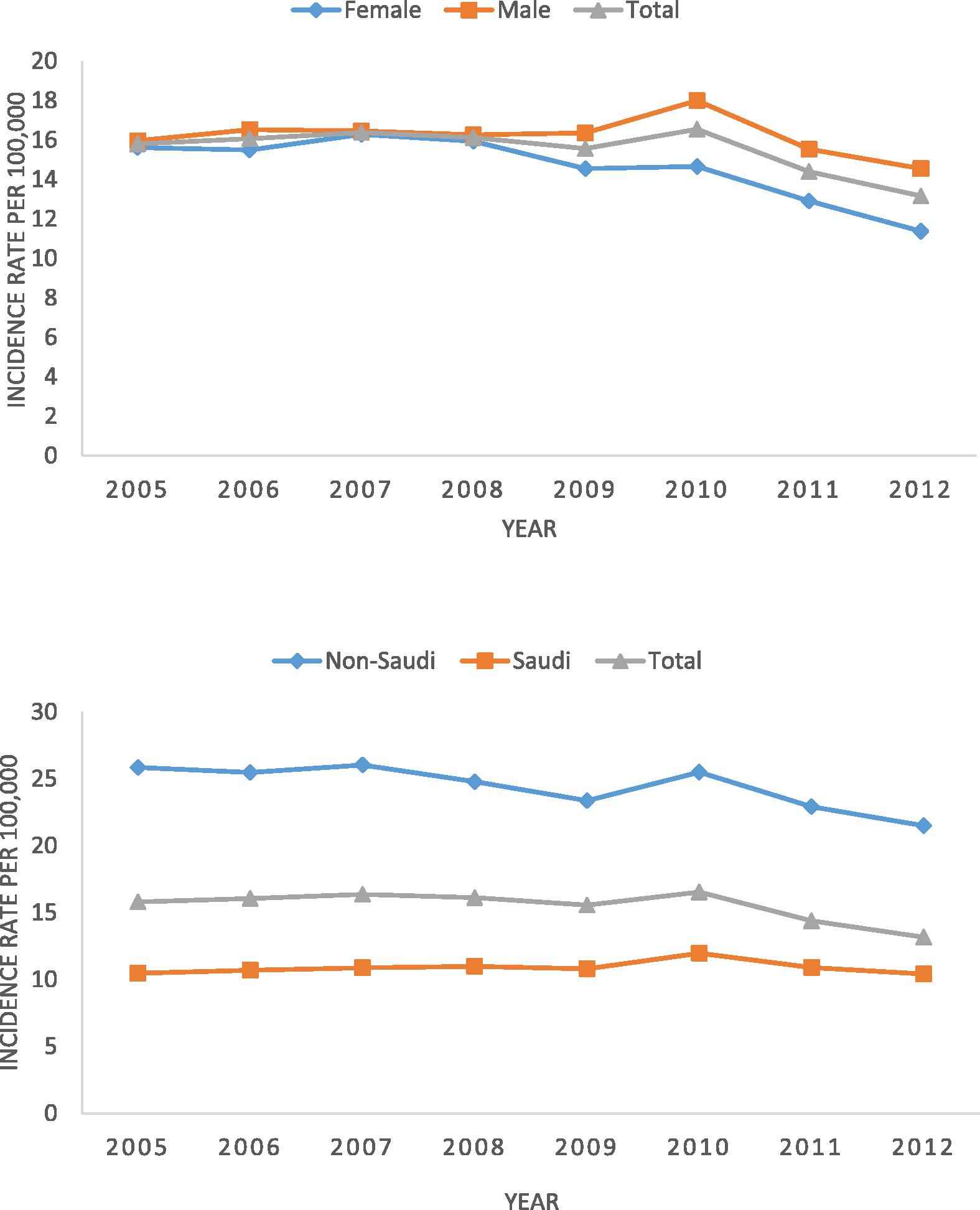
Incidence rates of reported cases of tuberculosis, by sex and nationality, in the Kingdom of Saudi Arabia from 2005 to 2012.
By region, this study observed that Mecca had a consistently greater IR over the study period compared with other regions [25.13/100,000 (95% CI = 24.7–25.56); Fig. 2]. Riyadh was the region with the second highest IR [17.9/100,000 (95% CI = 17.53–18.27)] followed by Jazan [17.1/100,000 (95% CI = 16.31–17.89)]. Hail had the lowest TB IR during the study period [6.1/100,000 (95% CI = 5.4–8.6)].
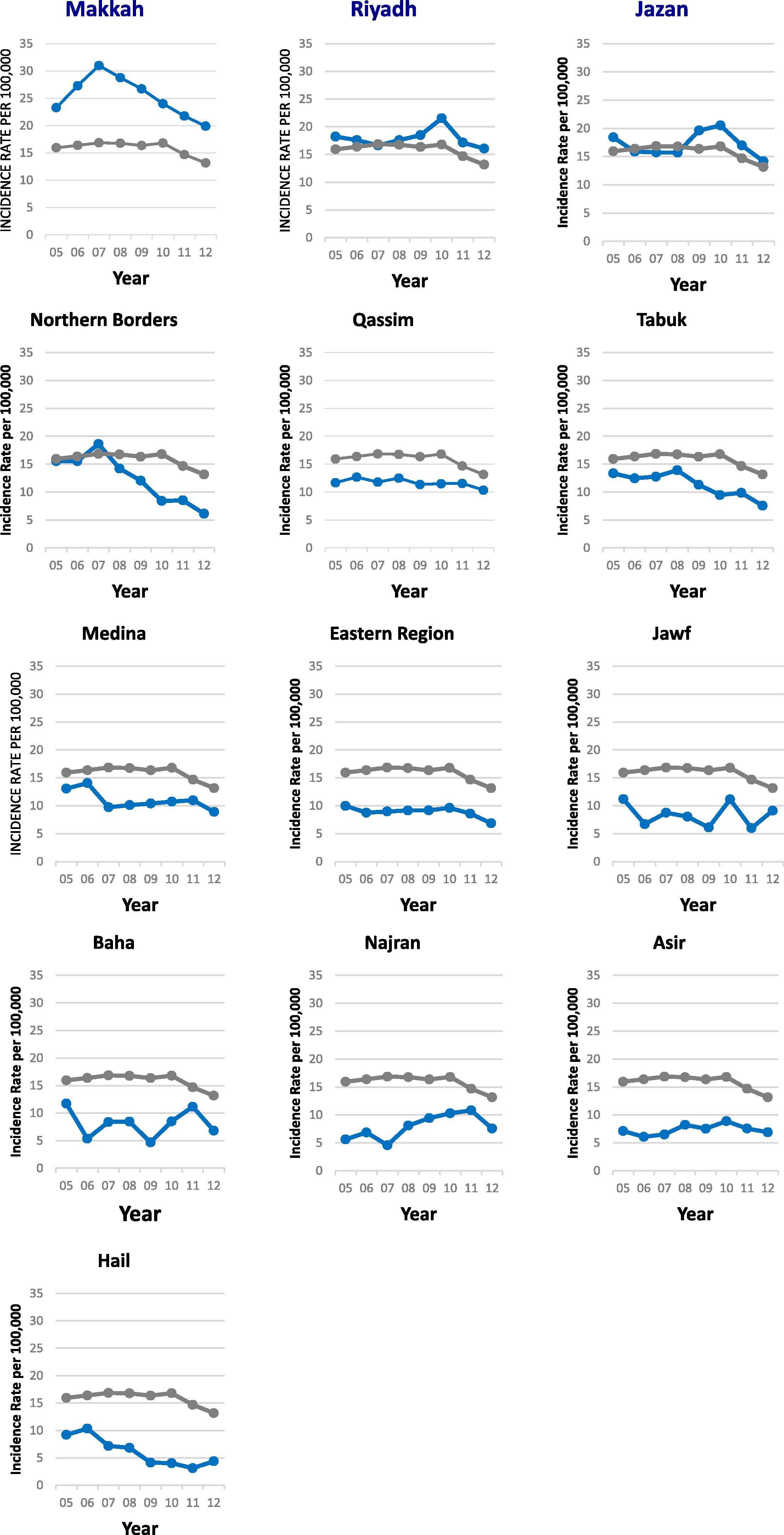
Incidence rates of reported cases of tuberculosis, by region, in the Kingdom of Saudi Arabia from 2005 to 2012.
Investigating the proportion of TB cases by nationality, non-Saudis from the following countries had the highest proportion of TB cases (Fig. 3): Indonesia (15.73%), Yemen (12.91%), India (9.71%), and Pakistan (8.36%). By age category, individuals <15 years of age constituted 14.21% of the TB cases, those aged 21–30 constituted 27.73% of the cases, and those aged ≥65 constituted 7.41% of the cases (Fig. 4). By employment status, the employed non-Saudis had the highest proportion of TB (56.42%), followed by unemployed Saudis (39.46%) (Fig. 5). Students comprised 15.33% of all TB cases, whereas prisoners comprised 11.22% of all cases.
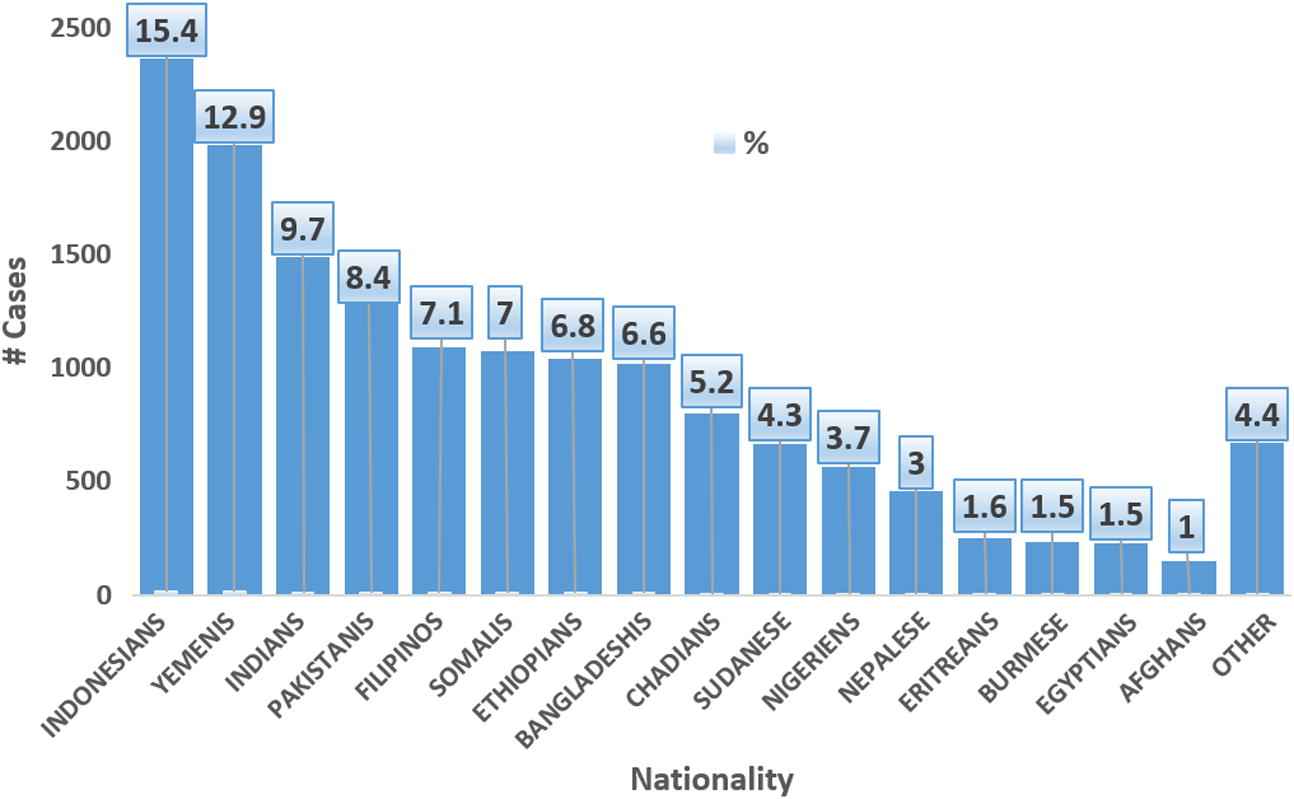
Number and proportion of reported cases of tuberculosis, by nationality, in the Kingdom of Saudi Arabia from 2005 to 2012.
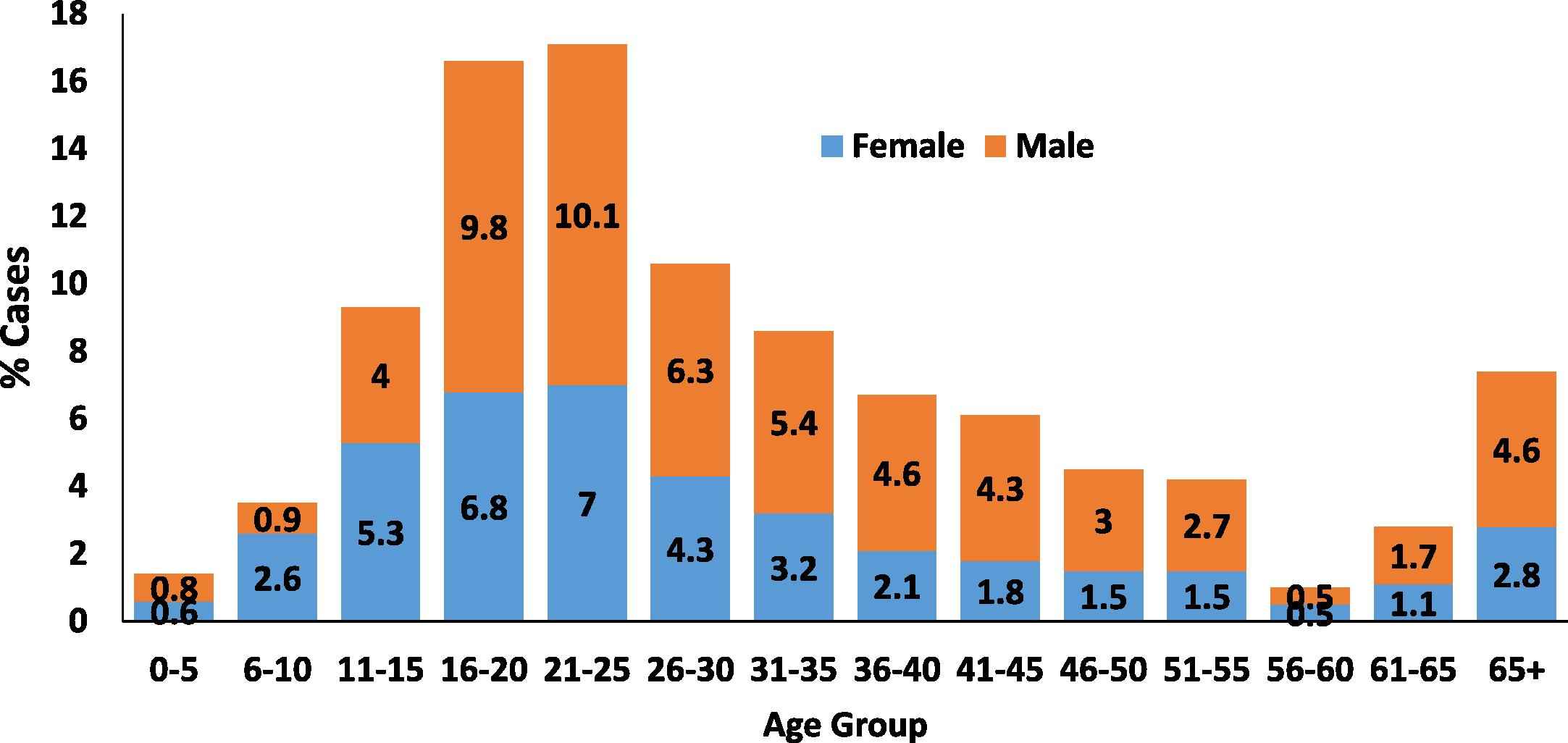
Proportion of reported cases of tuberculosis, by age group and sex, in the Kingdom of Saudi Arabia from 2005 to 2012.
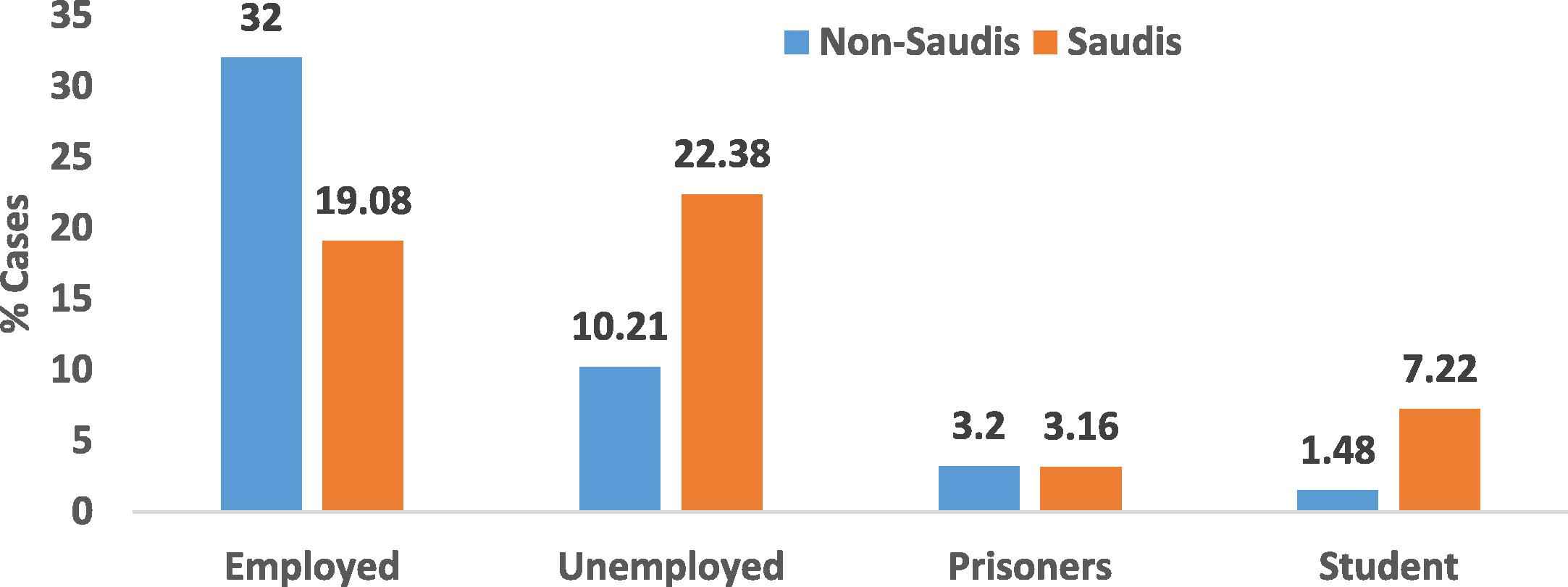
Proportion of reported cases of tuberculosis, by Employment status and stratified by nationality, in the Kingdom of Saudi Arabia from 2005 to 2012.
Of the 32,435 suspected TB cases in this study, 18,429 were laboratory confirmed by either culture or smear using the WHO guidelines, with the culture test suggested to be more conclusive than a smear test [8] (Table 2). Of the remaining suspected cases, 8474 tested negative for TB via culture or smear, whereas 5505 cases were not tested for TB using culture or smear (Table 3).
| Culture | Smear test | N | Diagnosis tests final outcome |
|---|---|---|---|
| Positive | Positive | 874 | Positive |
| Negative | 627 | Positive | |
| Not done | 82 | Positive | |
| Negative | Positive | 93 | Positive |
| Negative | 253 | Negative | |
| Not done | 26 | Negative | |
| Not done | Positive | 16,753 | Positive |
| Negative | 8195 | Negative | |
| Not done | 5505 | Not done |
Culture and smear test results for reported cases of tuberculosis, in the Kingdom of Saudi Arabia, from 2005 to 2012.
| Final outcome of diagnostic tests | N | (%) |
|---|---|---|
| Positive | 18,429 | 57 |
| Negative | 8474 | 26 |
| Not done | 5505 | 17 |
| Total | 32,435 | 100 |
Laboratory outcomes of reported cases of tuberculosis, in the Kingdom of Saudi Arabia, from 2005 to 2012.
Based on confirmed TB cases by either positive culture or smear, the overall proportion of laboratory testing for TB in KSA was 56.77% from 2005 to 2012. The region with the greatest proportion of laboratory-confirmed cases was Medina (64.18%), followed by the Eastern Region (63.71%) and Mecca (59.78%). The regions with the lowest proportion of laboratory testing were Hail and Northern Borders (39.93% each; Table 4).
| Year | Asir | Baha | Eastern Region | Hail | Jawf | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | LCC | % | N | LCC | % | N | LCC | % | N | LCC | % | N | LCC | % | |
| 2005 | 129 | 72 | 56 | 62 | 32 | 52 | 333 | 206 | 62 | 53 | 16 | 30 | 44 | 36 | 82 |
| 2006 | 113 | 80 | 71 | 29 | 15 | 52 | 299 | 171 | 57 | 61 | 22 | 36 | 27 | 12 | 44 |
| 2007 | 116 | 65 | 56 | 33 | 18 | 55 | 320 | 194 | 61 | 40 | 12 | 30 | 34 | 19 | 56 |
| 2008 | 150 | 80 | 53 | 34 | 17 | 50 | 334 | 198 | 59 | 39 | 15 | 38 | 32 | 18 | 56 |
| 2009 | 140 | 89 | 64 | 19 | 14 | 74 | 341 | 219 | 64 | 24 | 15 | 63 | 25 | 16 | 64 |
| 2010 | 170 | 87 | 51 | 35 | 20 | 57 | 395 | 233 | 59 | 24 | 12 | 50 | 49 | 23 | 47 |
| 2011 | 148 | 83 | 56 | 47 | 31 | 66 | 362 | 259 | 72 | 19 | 5 | 26 | 27 | 11 | 41 |
| 2012 | 141 | 85 | 60 | 30 | 14 | 47 | 303 | 232 | 77 | 28 | 18 | 64 | 43 | 25 | 58 |
| Total | 1107 | 641 | 58 | 289 | 161 | 56 | 2687 | 1712 | 64 | 288 | 115 | 40 | 281 | 160 | 57 |
| Year | Jazan | Medina | Mecca | Najran | Northern Borders | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | LCC | % | N | LCC | % | N | LCC | % | N | LCC | % | N | LCC | % | |
| 2005 | 221 | 115 | 52 | 200 | 137 | 69 | 1407 | 697 | 50 | 24 | 9 | 38 | 43 | 14 | 33 |
| 2006 | 195 | 116 | 59 | 220 | 130 | 59 | 1688 | 975 | 58 | 30 | 14 | 47 | 44 | 14 | 32 |
| 2007 | 203 | 123 | 61 | 159 | 85 | 53 | 1894 | 1058 | 56 | 21 | 6 | 29 | 55 | 17 | 31 |
| 2008 | 207 | 124 | 60 | 169 | 111 | 66 | 1799 | 1123 | 62 | 38 | 16 | 42 | 43 | 17 | 40 |
| 2009 | 268 | 168 | 63 | 179 | 124 | 69 | 1696 | 1067 | 63 | 46 | 29 | 63 | 37 | 14 | 38 |
| 2010 | 280 | 180 | 64 | 191 | 134 | 70 | 1660 | 1078 | 65 | 52 | 26 | 50 | 27 | 12 | 44 |
| 2011 | 237 | 140 | 59 | 200 | 121 | 61 | 1544 | 932 | 60 | 56 | 23 | 41 | 28 | 18 | 64 |
| 2012 | 207 | 105 | 51 | 170 | 113 | 66 | 1486 | 946 | 64 | 41 | 21 | 51 | 21 | 13 | 62 |
| Total | 1818 | 1071 | 59 | 1488 | 955 | 64 | 13,174 | 7876 | 60 | 308 | 144 | 47 | 298 | 119 | 40 |
| Year | Qassim | Riyadh | Tabuk | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N | LCC | % | N | LCC | % | N | LCC | % | |
| 2005 | 127 | 60 | 47 | 956 | 498 | 52 | 88 | 41 | 47 |
| 2006 | 141 | 61 | 43 | 944 | 508 | 54 | 84 | 34 | 40 |
| 2007 | 128 | 45 | 35 | 985 | 541 | 55 | 96 | 42 | 44 |
| 2008 | 139 | 66 | 47 | 1065 | 564 | 53 | 107 | 40 | 37 |
| 2009 | 129 | 68 | 53 | 1155 | 608 | 53 | 90 | 35 | 39 |
| 2010 | 140 | 59 | 42 | 1460 | 722 | 49 | 75 | 32 | 43 |
| 2011 | 144 | 77 | 53 | 1191 | 580 | 49 | 80 | 45 | 56 |
| 2012 | 135 | 68 | 50 | 1174 | 634 | 54 | 64 | 31 | 48 |
| Total | 1083 | 504 | 47 | 8930 | 4655 | 52 | 684 | 300 | 44 |
LCC = laboratory-confirmed cases.
Number and proportion of laboratory-confirmed cases of reported tuberculosis, by region, in the Kingdom of Saudi Arabia, from 2005 to 2012.
4. Discussion
The overall IR of TB in KSA showed a statistically significant decrease from 2005 to 2012. The TB IR was generally higher among males compared with females over the last 4 years of the study period (2009–2012). Non-Saudis had about two times the TB IR of Saudis. The TB IR was highest in Mecca compared with other regions, followed by Riyadh and Jazan. When stratified by age group, TB was found in 1.4% of those aged <5, 12.81% in those aged 6–15, and 7.41% of those aged >65. Regarding TB laboratory testing, there was a 15% difference between the regions with the greatest and lowest laboratory-testing proportion. The findings from this study regarding TB IR trend are agreeable with the findings from previous studies that overlap with the study period [4,6,9].
This decrease in TB IR from 2005 to 2012 can potentially be attributed to the positive impact of directly observed treatment (DOTS), which was implemented in 2000 by the National TB Program [6]. It could also be attributed to the policy change that has enabled non-Saudis to seek diagnosis and treatment for TB without the fear of deportation, which encourages them to seek medical services; however, this does not eliminate the possibility to be dismissed by their employer for having TB, which might prevent some to seek diagnosis and treatment [9]. In addition, the higher IR in males compared with females could be explained by the fact that males in KSA are more engaged in public events than females [9]. Many of these events occur in crowded places conducive to airborne transmission.
The high TB IR in non-Saudis compared with Saudis could be attributed to multiple factors. First, most of the immigrants in KSA come from countries with high TB IRs such as Pakistan, India, Bangladesh, Yemen, and Indonesia [6]. Second, many immigrants live in crowded conditions conducive to TB transmission, have poor diets, and engage in physically stressful manual labor, rendering them more susceptible to the disease [6]. Furthermore, although the government stopped deporting non-Saudis diagnosed with TB, many are still afraid to seek medical services because they fear being dismissed by their employer(s) [6].
The high TB IR in Mecca could be explained by the presence of a high proportion of immigrants and by the 2.5 million pilgrims who visit the holy city each year. Many of the pilgrims and immigrants come from countries with a high IR of TB. The high IR in Riyadh could be attributed to a higher frequency of reporting due to the presence of a large number of tertiary hospitals that treat patients from all over KSA. In addition, it is a major employment destination for non-Saudis. The high IR in Jazan could be attributed to its proximity to Yemen, which has a high overall TB IR.
The presence of TB cases among children aged <5 indicates ongoing active transmission. This was also indicated by the fact that those in the 6–15-year-old category comprised 12.81% of the cases; the immune system is thought to be more resistant to TB during this age range than any other age [1]. The high proportion of TB cases in the ≥65-year age group could reflect a high prevalence of latent TB among young persons, whose TB may have been activated after their immune systems weakened.
The difference between regions in TB laboratory testing could be attributed to the presence of a larger number of tertiary hospitals in certain regions that engage in a high proportion of laboratory testing; these facilities are better equipped to perform laboratory investigations than other health centers.
A limitation encountered was the lack of population statistics stratified by age, employment status, and non-Saudi nationality. This prevented further calculation and analysis of the IRs. In addition, there was a lack of population statistics for Mecca city that prevented further analysis. Another limitation of this study is that most of the suspected cases of TB were laboratory confirmed using the smear test, which is less conclusive than a culture [8]. This resulted in having approximately 43% of TB cases with no laboratory confirmation, which does not eliminate the possibility of overdiagnosing the cases based on clinical symptoms and radiological investigations alone. A key strength of this study is that it used case-based data instead of aggregated data. This type of data provided the culture, smear, and radiography results for each patient and made it possible to filter out confirmed cases based on the smear and culture laboratory results in accordance with the WHO guidelines [8].
Continued support for the DOTS approach can have a positive impact on TB control in KSA. In addition, special attention needs to be paid to the high IR among non-Saudis. A screening program needs to be implemented to test all non-Saudi workers for TB at their ports of entry. Furthermore, once TB patients are diagnosed inside KSA, their contacts should be screened, including family members, roommates, and co-workers.
Special attention needs to be given to the Mecca region for better control of TB. Pilgrims should be screened for TB before they are granted a Hajj visa. In addition, health authorities should encourage the use of facemasks by pilgrims and workers around the holy areas during the Hajj season. All vulnerable residents of Mecca should be encouraged to get the anti-TB vaccine. Further studies need to be performed to identify the precise impact of Hajj on Mecca region’s TB IR. All vulnerable residents of Jazan should be also encouraged to receive the anti-TB vaccine due to its proximity to Yemen.
To improve the laboratory confirmation of TB screening programs throughout KSA, access to culture or smear testing should be available to all health centers. In addition, assessments should be conducted regarding the ability of laboratories to detect and diagnose TB cases, and training should be provided if necessary. Furthermore, TB testing should be performed by a central laboratory located in each region that receives specimens from health centers that are not equipped to conduct the testing themselves.
Conflicts of interest
All authors have no conflicts of interest to declare.
Acknowledgments
I wish to express my sincere gratitude to my supervisor Dr. Scott McNabb, my friend and fellowship team member Ms. Natalie Schulhofer, and the other team members Mr. Suman Kundu and Mr. Prabhjyot Saini for their support and contribution to my thesis.
I would also like to thank Dr. Abdullah Assiri, Dr. Raffat Alhakeem, and Dr. Tamara Tayeb for their help in supplying the data for this study.
I am also very grateful to my colleagues and family, especially my wife Razan, for their continuous support through my years of study.
References
Cite this article
TY - JOUR AU - Fahad M. Almutairi AU - Tamara Tayeb AU - Raffat Alhakeem AU - Abdulaziz bin Saeed AU - Abdullah Assiri AU - Scott J.N. McNabb PY - 2017 DA - 2017/11/02 TI - Distribution and determinants of tuberculosis in the Kingdom of Saudi Arabia from 2005 to 2012 JO - Journal of Epidemiology and Global Health SP - S23 EP - S28 VL - 7 IS - Supplement 1 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2017.08.002 DO - 10.1016/j.jegh.2017.08.002 ID - Almutairi2017 ER -