
Declining trends in injuries and ambulance calls for road traffic crashes in Bahrain post new traffic laws of 2015
- DOI
- 10.1016/j.jegh.2016.02.004How to use a DOI?
- Keywords
- Epidemiology; Injuries; Road traffic crashes
- Abstract
Road traffic crashes (RTC) are of serious global health concern. To identify whether the number of ambulance calls, injuries, and deaths has declined after the implementation of the new traffic law (NTL) 2015 in Bahrain, de-identified administrative RTC data obtained from the tertiary care center, and the General Directorate of Traffic (GDT) of Bahrain were used. A quasi-experimental design was employed to trend the impact of the NTL on RTC and associated healthcare events. Bahrainis and non-Bahrainis who met with RTC, either in a vehicle or as a pedestrian, between February 8 and May 8 in 2013, 2014 (pre NTL), and 2015 (post NTL) were included in the study. Our results show a reduction in the number of ambulance calls from vehicular and pedestrian RTC victims. The ambulance calls from pedestrian RTC victims were <10% compared to the number of ambulance calls from vehicular RTC victims. There was a significant reduction in minor injuries post 2015, whereas no obvious difference was seen for serious injuries and deaths. A longer follow-up study to confirm the sustained decline in RTC, enforcing a zero tolerance policy toward traffic transgressions, and raising public awareness on the “critical four minutes” and “golden hour” is recommended.
- Copyright
- © 2016 Ministry of Health, Saudi Arabia, Production and hosting by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)
1. Introduction
Road traffic crashes (RTC) are a serious public health concern, but a preventable cause of death. To thrust RTC as a priority for prevention, the World Health Organization (WHO) brought out a theme of “Road Safety is No Accidents” in 2004 [1]. However, RTC continue to occur globally, causing serious health problems that have dramatic social implications; the suffering for victims and their families due to RTC-related injuries is inestimable.
By definition, an RTC is a collision or incident that may or may not lead to injury occurring on a public road and involving at least one moving vehicle, and “road traffic injuries” are fatal or nonfatal injuries incurred as a result of an RTC [2]. The burden of RTC is a leading cause of all trauma admissions in hospitals worldwide [3]. RTC injures or disables between 20 million and 50 million people each year. By 2020, road traffic injuries are expected to be the third largest contributor to the global burden of diseases if the current trend continues [4,5]. Three out of four deaths from RTC are among men and RTC is the number one cause of death among those aged between 15 years and 29 years [6].
Among the WHO regions, the Eastern Mediterranean Region (EMR) had the second highest road traffic fatality rate in the world in 2013, with 21.30 per 100,000 population, compared to a global rate of 18.03 per 100,000 population [7]. More than 75% of all road traffic deaths in the EMR occurred among males, while 60% occurred in the productive age group of 15–44-year-olds [8]. Bahrain is categorized as a high income Gulf State in the EMR, with a population of approximately 1.3 million that accommodates a wide variety of multiethnic communities. Expanded networks of roads [9], accompanied by an increased number of motor vehicles are recognized to have increased RTC and are a growing public health problem in Bahrain [10]. For instance, the General Directorate of Traffic (GDT) of Bahrain recorded 402,225 traffic violations in 2014. Of all the recorded traffic violations, 12% were over speeding and 5% were jumping red lights. The other 5% included 17,171 using a mobile phone while driving, 237 were driving while alcohol-impaired, and 1068 were driving without a valid driving license. Over 75% of the violations were of many categories that included the following: driving an unlicensed vehicle, driving a vehicle that makes a noise or exhaust smoke; loading and unloading vehicles on the road in the unauthorized times; damaging traffic signs; parking in residential areas and in the parks of disabled persons; the presence of a child in the vehicle without a single seat and not using a safety belt; using the vehicle for a purpose other than that mentioned in the driver’s license; driving a vehicle without a registration certificate, number plates, or with plates that have been canceled or defaced; and driving a vehicle without brakes or with brakes which are unfit to use. Deliberately blocking or obstructing a road; handing a vehicle to someone who does not hold a license to drive it; racing a vehicle; faking, defacing, or changing the date of registration or number plates; and transferring the number plates from one vehicle to another without permission were other recorded traffic violations. Further, a retrospective review of the data from 2003 to 2010 in Bahrain found that the RTC fatality rates were high among the young, and were 3.5 times more than the general population [11]. The updated as of July 2014 WHO mortality database for Bahrain showed that the number of transport deaths was 96 in 2009, and 50% of them were found in the age groups of 15–24 years and 35–54 years [12].
RTC are caused by many factors that include faulty vehicles and poor road design, but the majority are attributed to driver-related factors, especially over speeding [13,14], alcohol-impaired driving [15,16], and distraction of drivers mostly by mobile phone use while driving [17,18]. The decrease in RTC and road traffic injuries can be achieved by following the WHO recommended five road safety pillars, namely road safety management or policy, road infrastructure, safe vehicles, road users’ safe behavior, and post-crash care [19]. The health sector is an important partner in this process. Its roles are to strengthen the evidence base, provide appropriate prehospital and hospital care, rehabilitation, conduct advocacy, and contribute to the implementation and evaluation of interventions [20].
Considering the poor compliance with the existing 35-year-old traffic laws by the road users of Bahrain, a new traffic law (NTL) came into force on the February 8, 2015. The NTL was the result of careful studies and research that lasted over 8 years for reducing traffic accidents in Bahrain, specifically the serious ones. Through the GDT, the ministry of interior established a legal framework in accomplishing the ultimate goal of saving lives and property by imposing tougher penalties to deter offenders and for anyone who commits traffic crimes, especially the serious ones that could cause death or fatal injuries. The NTL was designed by a “demerit point system” that uses a set of points for every traffic fine according to the seriousness of the crime. Each driver should not exceed 20 points, or the driving license will be withdrawn for 3 months for the first time. If the points reach 20, the license will be withdrawn for a year. The license will be withdrawn again for a year if the driver recollects another 20 points. The fourth time, the license will be withdrawn until the driver passes the rehabilitation course. Over speeding (exceeding the speed limit by up to 30%) of the limit will be punished with imprisonment from 1 month to 3 months, or a fine of 50–250 Bahraini Dinar and exceeding the speed limit above 30% of the limit will be punished with imprisonment from 1 month to 6 months, or a fine of 100–500 Bahraini Dinar; using mobile phones while driving (a fine of 20–200 Bahraini Dinar) and violating the traffic lights (imprisonment up to 6 months, and a fine of 100–500 Bahraini Dinar) are considered to be the most significant crimes under the NTL. To step up roadway surveillance, traffic policemen were out in force and more cameras were installed at strategic locations on the roads across Bahrain. The NTL was promoted through public awareness and educational campaigns, with considerable media coverage, to minimize RTC and associated healthcare events [21].
To monitor the impact of the NTL, this study was aimed at identifying whether the number of ambulance calls, injuries, and deaths has declined after the implementation of the NTL 2015 in Bahrain.
2. Materials and methods
We analyzed deidentified administrative RTC data obtained from the accident and emergency department of Salmaniya Medical Complex (SMC), Manama, Bahrain and the GDT of Bahrain. The SMC is the oldest and largest, public tertiary care center that provides free healthcare in Bahrain. With official ethical approval, the data were collected by a group of 4th year students of a BSc Nursing program, College of Health Sciences, University of Bahrain, Salmanya, Bahrain as a data collection exercise in their research course.
Dial 999 is a common telephone code in Bahrain for police, ambulance, and fire emergencies. When a caller requests an ambulance for a medical emergency, the Accident and Emergency Department of SMC responds by dispatching an ambulance. Rarely, patients are directed to the Bahrain Defence Forces (BDF) hospital (with one third of the bed capacity compared to SMC), depending on the proximity of the RTC site to the hospital. In cases of certain injuries where the ambulance has not been requested, the patients may have sought medical care at other hospitals and clinics. Data from the BDF hospital, other hospitals, and clinics were not available to us. Nonetheless, RTC victims visiting other hospitals or clinics, and ambulance dispatches other than from SMC are negligible, since SMC is the first responder to 999 telephone call requests for medical emergencies and ambulance, and SMC data can be reckoned to fairly represent the national data. The data were cleaned by omitting non-RTC ambulance calls and related injuries.
Bahrainis and non-Bahrainis residing or who were residents of Bahrain in 2013–2015 formed the population for this study. The population data were obtained from Bahrain Open Data Portal for 2013 and 2014 [22]. The population projection for 2015 was made to 2014 data with a projected growth rate of 2.81% as provided in the Bahrain population history [23]. A quasi-experimental design (before and after intervention without a control group) was used to trend the impact of the NTL on RTC and associated healthcare events. All Bahrainis and non-Bahrainis who met with RTC, either in a vehicle or as a pedestrian, between February 8 and May 8 (90 days) in 2013, 2014 (pre NTL), and 2015 (post NTL) were included in the study. We chose the time points a priori to accommodate the post NTL data collection, assuming the season, traffic, and the flow of tourists to be widely similar across the chosen time range. Data of pre NTL independently and pooled were compared to post NTL.
We defined “RTC admissions” using the International Classification of Diseases, 10th Revision (ICD-10) [24]. A 30-day definition of RTC deaths [2] complemented by GDT data and reconciled with the births and deaths registration office of the Public Health Directorate of the Ministry of Health, Bahrain, was used in the study. We used the record linkage between GDT and health sectors to improve data quality and harmonize across data sources as recommended in the global status report on road safety of the WHO [6]. Linkage and reconciliation of data were achieved completely by using the national identity number.
The classifications of injuries were based on the Abbreviated Injury Scale (AIS) of 2008. The AIS is the most commonly used, anatomically based, consensus derived, global severity scoring system that classifies each injury by body region according to its relative importance. For example a “minor injury” is a superficial laceration and the probability of death is nil; a “serious injury” is an open fracture of the humerus and the probability of death is between 8% and 10% [25]. Following the AIS criteria, the SMC and GDT data were classified as either minor (slight) or serious injuries and deaths.
Other than pedestrian RTC victims, vehicular RTC victims included the following: pedal cyclists, motorcycle riders, occupants of three-wheeled motor vehicle, car occupants, occupants of a pick-up truck or van, occupants of a heavy transport vehicle, and bus occupants.
2.1. Statistical data analysis
Frequency was obtained for categorical variables. We estimated the incidence rate of ambulance calls, injuries and deaths during 2013–2015. A version of the Chi-square test (Fisher’s exact test) was used to test the hypothesis whether the NTL enforcement has significantly reduced the incidence rate of ambulance calls, injuries, and deaths during 2015 compared to 2014 and 2013. The level of significance was set to 5%. In addition, we carried out a sensitivity analysis to the pooled data for 2013 and 2014 (pre NTL) and compared it to data of 2015 (post NTL). We performed subgroup analyses to identify the differences between Bahrainis and non-Bahrainis, vehicular and pedestrian, and gender for the number of ambulance calls, injuries and deaths.
All statistical analyses were carried out using Stata13 (Stata Corp. 2013. Stata Statistical Software: Release 13. Stata Corp LP, College Station, TX, USA).
3. Results
The number of ambulance calls received at SMC for vehicular and pedestrian RTC victims in 2013–2015 is presented in Fig. 1. The incidence rate for ambulance calls in the year 2014 (pre NTL) and 2015 (post NTL) was <1%. The relative estimate of the incidence rate ratio was 67% [95% confidence intervals (CI): 59–75%] indicating that there was a 33% reduction in the number of ambulance calls after the enforcement of the NTL. The two sided p value of the Fisher’s exact test was <0.05, which proved a statistically significant decrease in the number of ambulance call post NTL. Similarly, on comparing the data between 2013 (pre NTL) and 2015 (post NTL) the relative estimate of the incidence rate ratio was 72% (95% CI: 64–82%) with a significant p value of Fisher’s exact test <0.05; there was a 28% reduction in the number of ambulance calls in 2015 (post NTL) as compared to 2013 (pre NTL).
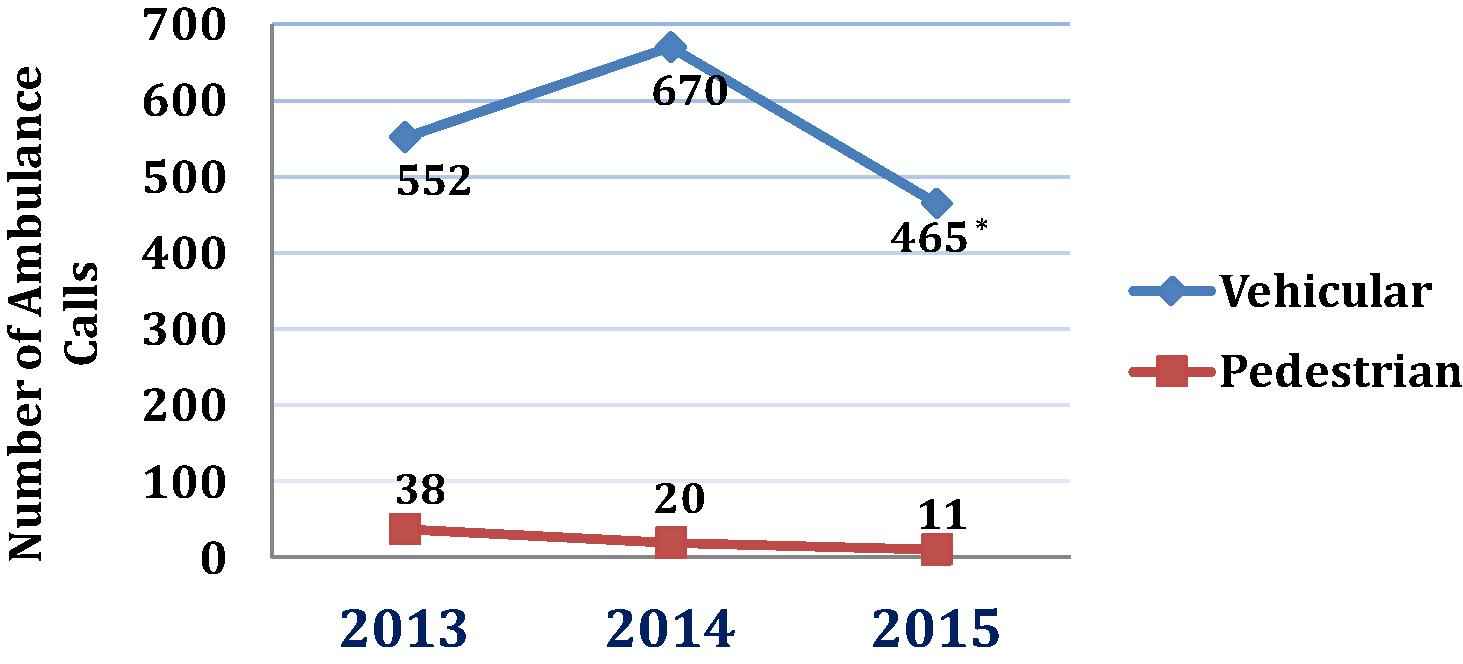
Number of ambulance calls received at Salmaniya Medical Complex (SMC) from vehicular and pedestrian road traffic crash (RTC) victims between 2013 and 2015 (February–May). The sensitivity analysis of the pooled data of 2013 and 2014 (pooled pre NTL) compared with the 2015 (post NTL), shows an incidence rate ratio of 69% [95% confidence interval (CI): 61–78%] corresponding to a reduction of 31%. *p value of Fisher exact test <0.05.
The sensitivity analysis of the pooled data of 2013 and 2014 (pooled pre NTL) compared with the 2015 (post NTL), showed the incidence rate ratio of 69% (95% CI: 61–78%) corresponding to a reduction of 31% with a significant p value of Fisher’s exact test <0.05.
Throughout our study period, the number of ambulance calls from vehicular and pedestrian RTC victims has reduced, and the number of ambulance calls from pedestrian RTC victims was <10% as compared to the number of ambulance calls from vehicular RTC victims. There were more Bahraini vehicular RTC victims than non-Bahrainis, whereas the number of Bahraini pedestrian RTC victims was less than the non- Bahrainis, except for the year 2014 (Table 1). There were more males than females in both categories of vehicular and pedestrian RTC victims. Adults far outnumbered child RTC victims (data not shown).
| Vehicular | 2013 | 2014 | 2015a |
|---|---|---|---|
| Bahraini | 349 | 452 | 307 |
| Non-Bahraini | 203 | 218 | 158 |
| Total | 552 | 670 | 465* |
| Pedestrian | |||
| Bahraini | 21 | 10 | 1 |
| Non-Bahraini | 17 | 10 | 10 |
| Total | 38 | 20 | 11 |
Number of ambulance calls in 2015 was significantly less than that in each preceding year-2014 and 2013.
p value of Fisher’s exact test <0.05.
Number of ambulance calls received at Salmaniya Medical Complex (SMC) from road traffic crash (RTC) victims categorized by residential status between 2013 and 2015 (February–May).
During the observed time periods, there was a significant reduction in minor injuries post 2015, whereas no obvious difference was seen for serious injuries (Fig. 2). The incidence rates for minor injuries between 2013 and 2015 and between 2014 and 2015 were similar and <1%. The incidence rate ratio was 71% (95% CI: 59–85%), indicating a 29% reduction in the number of minor injuries in the year 2015 with a significant p value of Fisher’s exact test <0.05. The number of deaths was <20 for each of the observed years, with no significant differences.
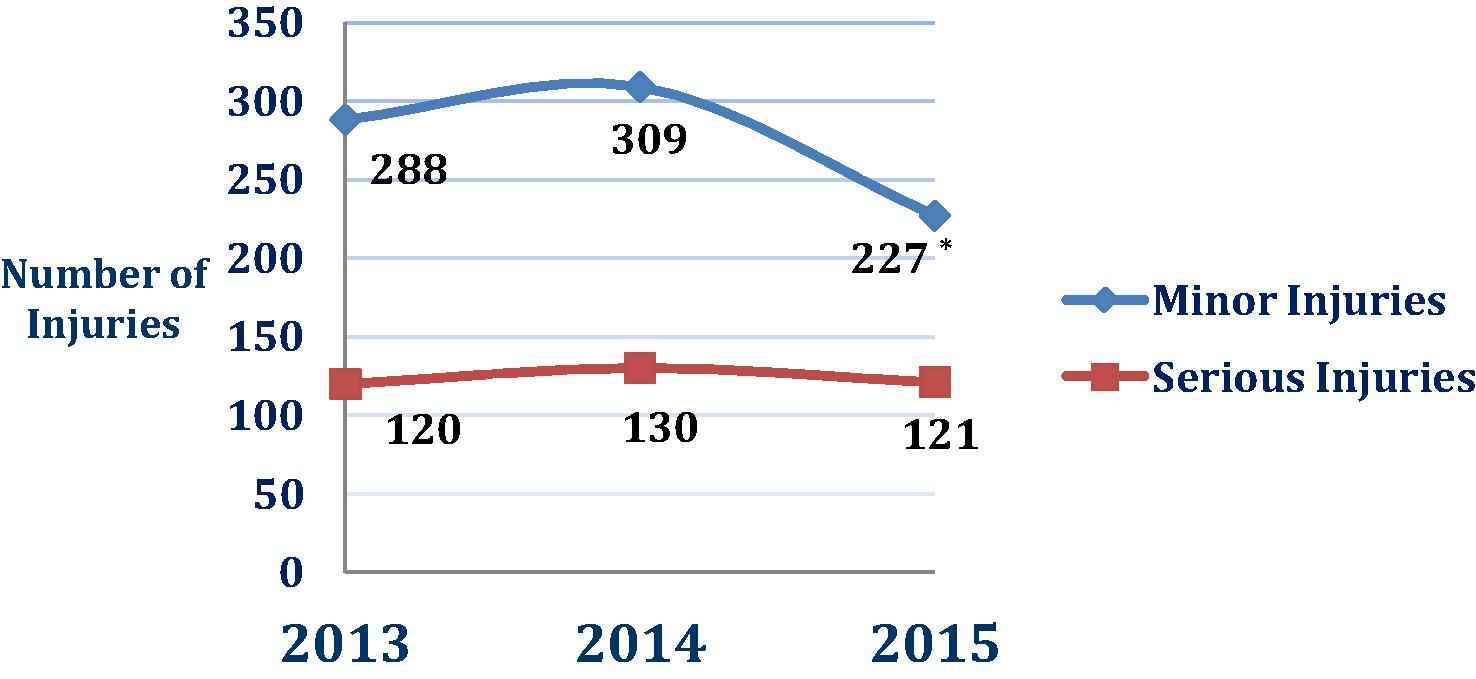
Number of minor and serious injuries suffered by road traffic crash (RTC) victims between 2013 and 2015 (February–May). The incidence rate for minor injuries between 2013 and 2015 and between 2014 and 2015 was similar and <1%. The incidence rate ratio was 71% [95% confidence interval (CI): 59–85%] indicating a 29% reduction in the number of minor injuries in the year 2015. *p value of Fisher exact test <0.05.
4. Discussion
Road safety is a multisectoral and multidimensional issue that plays an important integrated role in sustainable road transportation. RTC tend to be under recognized as a major health problem in many countries, and the success of road safety and the prevention of RTC hinge on gathering and analyzing the reliable RTC data. Over the years, public health interventions that alter population-level risk exposure have yielded a number of improvements. To ascertain the positive impact of the NTL in Bahrain, we collected the data from authentic sources of the GDT and the accident and emergency department of SMC in Bahrain.
This foremost study of the successful implementation of NTL in Bahrain has shown that there is a significant reduction in the number of RTC associated ambulance calls (31%) and minor injuries (29%) between February 8 and May 8 (90 days) when compared with pre NTL (2013, 2014) and post NTL (2015). Similar to our findings, a Canadian report on the benefits of implementation of the NTL in British Columbia showed significant decreases in hospital admissions (8%) and ambulance calls (7.2%) for road trauma. By contrast, a 21% reduction in fatal crashes was observed in the Canadian report as compared to our findings [26]. Although our results indicate that the number of ambulance calls received from vehicular and pedestrian RTC victims reduced, the number of ambulance calls received from vehicular RTC victims was >90% compared to pedestrian RTC victims. Most vehicular RTC victims were Bahrainis. In some measure, this can be explained by vehicle ownerships, having a license to drive, the roads being used more often by the Bahrainis than non-Bahrainis, who are generally temporary residents with less ownership of vehicles and possession of the license, and dependence on employers for transport or public transport. We found more male and adult RTC victims than females and children, which was obvious, due to the prevailing practice that females are less likely to drive than their male counterparts. Notably, the NTL has not had a significant impact among the non-Bahraini pedestrian RTC victims so far; the trend in reduction has not occurred, presumably because most non-Bahraini pedestrians are expatriate laborers from the Asian subcontinent who possibly had different road use patterns before arriving in Bahrain and are yet to take cognizance of the traffic laws of Bahrain. A greater awareness about traffic rules with important safety tips will go a long way in curbing the incidence of pedestrian accidents.
There was a significant reduction in minor injuries, post NTL, whereas no obvious differences were seen for serious injuries-a threat to life associated with the injury-and deaths, suggesting that the impact of the RTC in causing serious injuries and subsequent deaths remains the same and is highly correlated as described in AIS. Evidence has been shown that the most common causes of an RTC death are due to loss of oxygen supply, often caused by a blocked airway, which normally takes<4 minutes (critical 4 minutes) to cause death and the 1st hour after the trauma – the “golden hour” [27]. Proper first aid given to RTC victims during the “critical 4 minutes” and “golden hour” can significantly reduce serious injuries and deaths, and the cogent role of the community is imperative in this regard.
Our findings are highly unlikely to be explained by changes in the reporting practice for pre NTL and post NTL periods of observations. The early trend indicates that there is a real decline in minor injuries and ambulances calls post NTL, due to road users taking cognizance of the NTL and being positive to comply with it. Nevertheless, our study had a few limitations. First, due to paucity of time, the data were gathered beginning on the day (February 8, 2015) the law was enacted and over only a course of 90 days in 2015. This was compared to the same time points of two preceding years. Moreover, this was a data gathering exercise for the students enrolled in a research course to be completed within a semester. Second, the data were limited to the GDT and SMC and no other healthcare providers. The data from other healthcare providers were not available to us, but the role of others in managing RTC victims is negligible. Third, the categorization of data by the time and location of RTC, age of the RTC victims, and type of vehicle involved in RTC were not available to us.
The public health approaches of surveillance and risk factor identification are required with categorization of data by the time and location of RTC, age of the RTC victims, and types of vehicle involved in the RTC. Therefore, we recommend a longer follow-up study incorporating the abovementioned approaches to explore the sustained number of serious injuries and deaths due to RTC post NTL, and also trend the seasonal patterns of RTC. This longer follow-up study should include a cost-benefit analysis component to ascertain the savings to the exchequer as well.
The benefits of NTL can be further harnessed by advocating a zero tolerance policy toward traffic transgressions. Further, RTC prevention must be embedded into a broad range of activities with the NTL, such as raising public awareness on the importance of compliance with legislation and application of individual protective measures for the personal safety of vulnerable road users. In this way, both individual and population based strategies of preventive medicine can prove quite successful while confronting public health challenges of RTC.
5. Conclusion
An NTL implemented in Bahrain in February 2015 has started to produce a decline in ambulance calls and minor injuries, as evidenced by our study results. However, no palpable changes could be observed in the serious injuries and deaths post NTL. Therefore, a longer follow-up study is required to confirm the sustained decline in RTC in total. To reduce serious injuries and deaths, enforcing a zero tolerance policy toward traffic transgressions and raising public awareness on the “critical four minutes” and “golden hour” are recommended.
Conflicts of interest
All contributing authors declare no conflicts of interest.
Acknowledgments
We thank the following: Dr. Aneesa Al-Sindi, Dean, College of Health Sciences, University of Bahrain for support and encouragement; Accident and Emergency Department, Salmanya Medical Complex, Ministry of Health, Bahrain; General Directorate of Traffic, Ministry of Interior, Bahrain; and Amani Mohamed, DuaaJaffar, Fatima Ali, Fatima Mohamed, Mariam Yousef, Noor Mansoor, and Zainab Abbas-4th year BSN students, College of Health Sciences, University of Bahrain.
References
Cite this article
TY - JOUR AU - Muyssar Sabri Awadhalla AU - Govindaraj Vaithinathan Asokan AU - Amina Matooq AU - Richard Kirubakaran PY - 2016 DA - 2016/03/16 TI - Declining trends in injuries and ambulance calls for road traffic crashes in Bahrain post new traffic laws of 2015 JO - Journal of Epidemiology and Global Health SP - 59 EP - 65 VL - 6 IS - 2 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2016.02.004 DO - 10.1016/j.jegh.2016.02.004 ID - Awadhalla2016 ER -