
Trends of reported human cases of brucellosis, Kingdom of Saudi Arabia, 2004–2012
- DOI
- 10.1016/j.jegh.2015.09.001How to use a DOI?
- Keywords
- Brucellosis; Saudi Arabia; Global health; Zoonotic; One Health
- Abstract
Human brucellosis is an important zoonotic disease and is especially concerning in the Kingdom of Saudi Arabia (KSA), where livestock importation is significant. We analyzed reported human brucellosis disease trends in KSA over time to help policymakers understand the magnitude of the disease and guide the design of prevention and control measures. By using data from the national registry from 2004 to 2012, we calculated the cumulative numbers by age group and months. Trends of incidence rates (IRs) by gender, nationality, and region were also calculated. We found that there was a greater number of cases (19,130) in the 15–44 years age group than in any other age group. The IRs significantly decreased from 22.9 in 2004 [95% confidence interval (CI) = 22.3, 23.5] to 12.5 in 2012 (95% CI = 12.1, 13). Males had a significantly greater IR than females. Most cases were reported during spring and summer seasons. The IR of Saudi citizens was significantly greater than that of non-Saudis, but this difference reduced over time. The IRs of Al-Qassim, Aseer, and Hail were in the highest 25th percentile. Young, male Saudi citizens living in highly endemic areas were at greatest risk of acquiring brucellosis. We recommend vaccinating susceptible animals against brucellosis and increasing the public’s awareness of preventive measures.
- Copyright
- © 2015 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)
1. Introduction
Brucellosis is a major bacterial zoonotic infectious disease, meaning that infected animals are the source of infection. Annually, there are >500,000 new brucellosis cases worldwide [1]. Since brucellosis affects both humans and animals, it negatively impacts the economic, agricultural, and health sectors. Its effects are influenced by its worldwide distribution; it is rare in most industrialized countries and more common in developing ones. However, the threat exists that brucellosis will expand globally as countries’ borders become more porous. This threat is higher in countries like the Kingdom of Saudi Arabia (KSA), which hosts a myriad of travelers and imports high numbers of livestock. The emergence of brucellosis can be expected in any country that does not apply critical disease prevention protocols. In KSA, which represents a significant focus of human brucellosis, this disease still constitutes a major health problem.
Brucellosis, also known as Malta fever, undulant fever, or Mediterranean fever, is a systemic infectious disease that is transmitted to humans through the ingestion of the unpasteurized or raw milk and cheese of animals infected with Brucella organisms (e.g., sheep, cattle, camels, pigs, and dogs) or via contact with infected animals. Ingestion of the undercooked meat of infected animals is an uncommon route of transmission. Brucellosis is considered one of the most common laboratory-transmitted infectious diseases. Transmission usually occurs when a laboratory technician accidently inhales the bacteria [2].
Although KSA is a country that has undergone rapid modernization over the past 40 years, maintaining traditions remains important. The combination of the modern and the traditional is a hallmark of Saudi Arabian life. Raising camels is an essential part of the history of KSA. Camel owners are proud to have them and take care of their dynasties. Also, they derive many benefits from camels, including the consumption of their milk and meat. Those who own and tend camels usually prefer to drink camel milk in its unpasteurized state, when it is frothy and warm, directly after squeezing it from a mother. Passersby also commonly enjoy camel milk, preferring to get it fresh directly from shepherds. People who live in rural areas often raise sheep and goats and serve their unpasteurized milk to guests.
KSA is the seat of Islam, home of the Two Holy Mosques, Haram Mosque and the Prophet’s Mosque, which are precious to every Muslim. Millions of pilgrims flock to these mosques to perform the Hajj rituals. Part of this ritual is the slaughter of goats, sheep, or other types of cattle. Muslims who are not doing Hajj also have cattle slaughtered, as it is part of the observance of the Hajj Holy days. In 1998 alone, the total number of imported livestock was 3.8 million animals, including goats, sheep, camels, and cows [3]. In 2010, the total value of live animal and animal product importation was more than $2.7 billion [4]. In 2013 during the Hajj season, 3.2 million goats, sheep, camels, and other cattle filled the Saudi markets. Of those livestock, 75% were imported and 25% were raised locally [5].
Although there has been a noticeable decrease in the incidence and prevalence of brucellosis worldwide, it remains a public health concern for local and international health agencies. Most cases occur during the spring and summer seasons among those aged 20–45 years [6]. KSA had the highest incidence of human brucellosis in the Middle East during the late 1990s, but the rate has decreased in recent years due to the implementation of regulations by the Saudi Ministry of Agriculture that make brucellosis vaccinations for cattle compulsory, improved control of imported livestock, and enhanced cooperation between veterinarians and the public health sector [7,8]. Even though its incidence has dropped, brucellosis is still considered endemic in KSA.
Because of its endemicity in KSA, the Ministry of Health (MoH) classified brucellosis as a notifiable disease. Local health departments must notify the Infectious Disease Department (IDD) of the MoH when cases are suspected or confirmed. A blood culture test can detect the disease, and this is how 40–70% of the cases are diagnosed; others are mainly diagnosed with a standard agglutination test [9]. Brucellosis cases present mainly with bouts of fever and musculoskeletal pain. Because of the nonspecific manifestation of its presentation, brucellosis diagnosis is challenging, which likely leads to underestimation and underreporting of brucellosis cases [10]. Endemicity varies across the regions of KSA; it is higher in rural areas, where people live in contact with animals [7].
According to the MoH, all brucellosis cases should be reported monthly-including number of cases, nationality, region, gender, and test result diagnosis-to the IDD. Every suspected case is investigated using a standard agglutination test, culture (blood or bone marrow, cerebrospinal fluid), enzyme-linked immunosorbent assay, or other tests if they are available. Along with the laboratory results, every reported case form includes all patient identification and disease data: name, age, sex, occupation, nationality, and contact information; physician in charge; time of reporting; travel history; history of animal contact; state of the ingested milk; and previous attacks of brucellosis [11].
Although brucellosis trends have been studied in KSA among different regions, this research extends the boundaries of these studies and includes brucellosis distribution and determination from 2004 to 2012 among the main regions of KSA, taking into account gender, nationality, and age groups. The distribution of brucellosis cases is studied by month as well.
2. Material and methods
Brucellosis data were collected from the IDD of the KSA MoH, while population data were collected from the Saudi Central Department of Statistics and Information. The estimated population data by region were taken from the Ministry of Finance, because these data were not available from the Saudi Central Department of Statistics and Information. The brucellosis data are reported from its origin at peripheral health centers and hospitals, where brucellosis cases usually discovered?, to its destination at the IDD at the MoH. The information about this process was collected mainly from the IDD at King Fahd Hospital in Al-Madina City, Saudi Arabia for the purpose of reporting qualification.
2.1. Variables
Gender is defined as female and male; nationality is classified as Saudi and non-Saudi; age groups are identified as <1 year old, 1–4 years old, 5–14 years old, 15–44 years old, and >45 years old; and frequency of cases is expressed in months. Population data were used from 2004 to 2012 and classified by gender, region, and nationality.
2.2. Statistical analyses
The incidence rate (IR) was calculated per 100,000 persons for the total population, region, and nationality, and when applicable, by nationality and gender [12]. Microsoft Excel 2011 (Mac, Impressa Systems, Santa Rosa, california, USA, 2010) was used to translate and organize the data sets and for developing graphs, charts, database concatenation, management, and statistical analyses.
3. Results
Brucellosis IR trends showed fluctuations from 2004 to 2012, with a steady decrease in the IR from 2009 on. A significant reduction of IR in the total population from 22.9 (95% CI: 22.3, 23.5) in 2004 to 12.5 (12.1, 13) in 2012 was observed (Table 1). The total number of cases for the period was 37,477, with a low of 3447 cases in 2008 and a high of 5169 cases in 2004.
| Year | No. of cases (IRa) | 95% CI |
|---|---|---|
| 2004 | 5169 (22.9) | 22.3–23.5 |
| 2005 | 3804 (16.3) | 15.8–16.8 |
| 2006 | 3997 (16.6) | 16.1–17.1 |
| 2007 | 4194 (16.8) | 16.3–17.3 |
| 2008 | 3447 (13.4) | 12.9–13.8 |
| 2009 | 4803 (18) | 17.5–18.5 |
| 2010 | 4460 (16.2) | 15.7–16.7 |
| 2011 | 3942 (13.9) | 13.5–14.3 |
| 2012 | 3661 (12.5) | 12.1–13 |
| Total | 37,477 |
CI = confidence interval; IR = incidence rate.
Incidence rate per 100,000 population.
Reported cases and incidence rates of human brucellosis, by year, Kingdom of Saudi Arabia, 2004–2012.
Over the total period of the study, the IRs among Saudi citizens were consistently higher than those among non-Saudis, but the difference between the IRs diminished over the study period: the IR among non-Saudis remained stable but the IR among Saudis gradually decreased, except in 2009. Saudi citizens had an IR of 27.1 (95% CI: 26.4, 28) and non-Saudis had an IR of 11.5 (10.7, 12.4) in 2004, while in 2012, Saudi citizens had an IR of 13.2 (95% CI: 12.7, 13.7) and non-Saudis had an IR of 11.2 (95% CI: 0.5, 11.9). Males had a consistently higher IR than females, and the overall IRs from 2004 to 2012 fell for both males and females, with the exception of 2009 (Fig. 1).
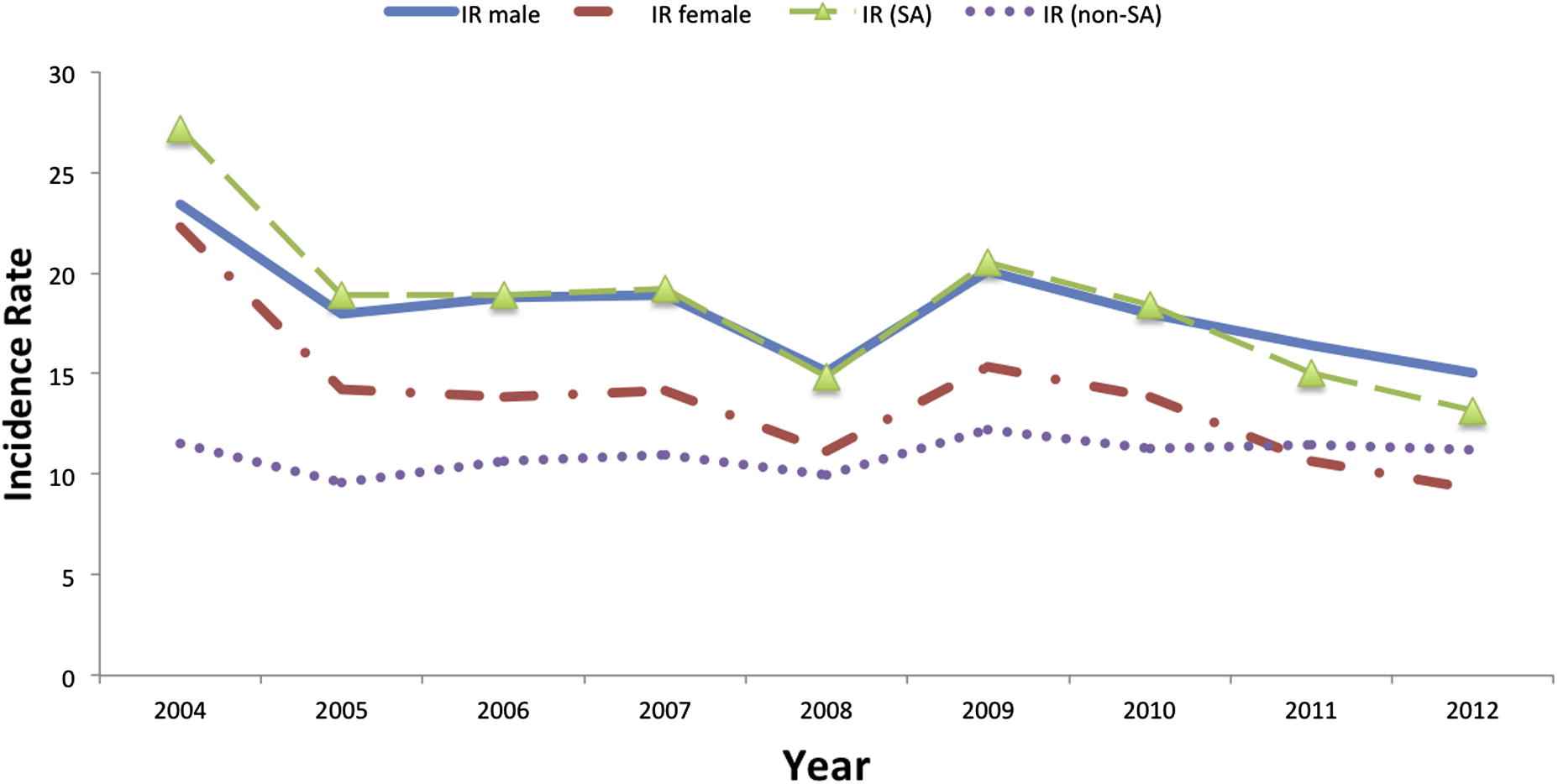
Incidence ratesa of reported cases of human brucellosis, by gender and nationality, Kingdom of Saudi Arabia, 2004–2012. aPer 100,000 population.
This trend was similarly reflected when gender was paired with nationality. There was a downward trend for both male and female Saudi citizens, but the IR among non-Saudi males and females remained stable during the study period (Fig. 2).
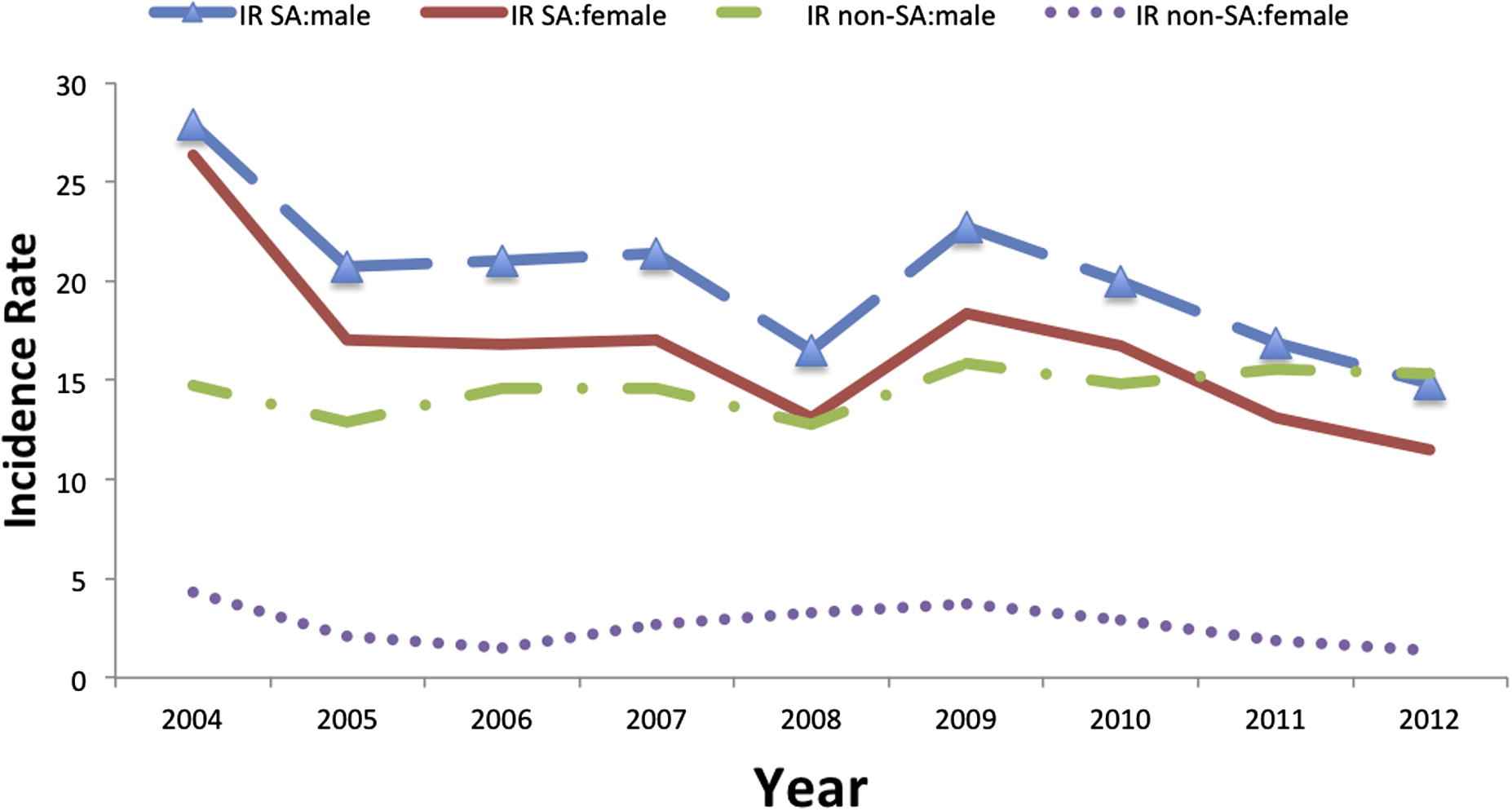
Incidence ratesa of reported cases of human brucellosis, by Saudi gender and non-Saudi gender, Kingdom of Saudi Arabia, 2004–2012. aPer 100,000 population.
By age group, those aged 15–44 years old had the highest prevalence, and those aged <1 year had the lowest prevalence. Among those aged <1 year, the average number of cases was 27.8 and the median was 29, while among those aged 1–4 years, the average was 406.6 cases and the median was 441. Among those aged 15–44 years, the average was 2155.1 cases and the median was 2193, and among those aged >45 years, the average was 784.4 cases and the median was 779.5 (Fig. 3).
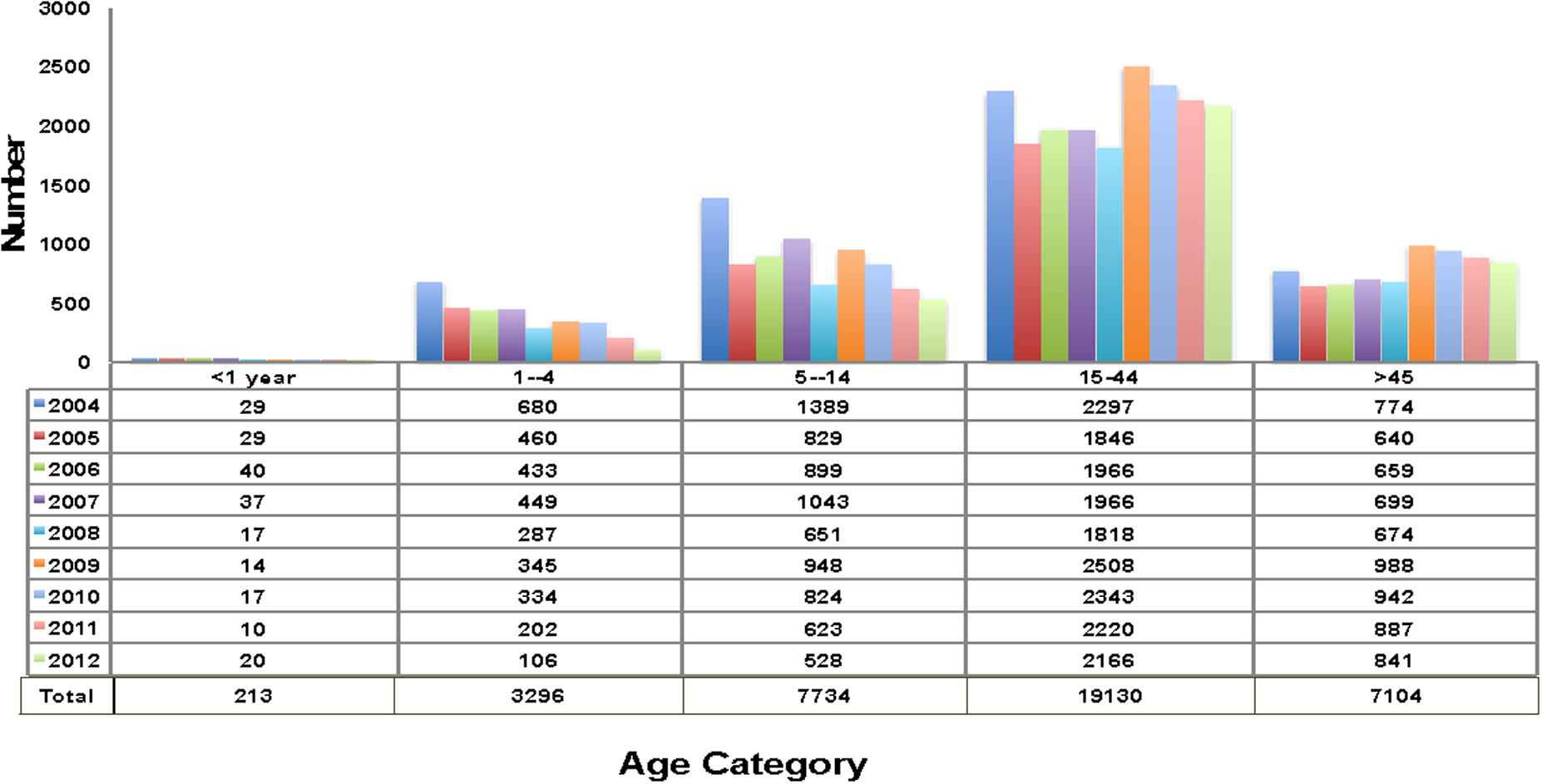
Reported cases of human brucellosis, by age category, Kingdom of Saudi Arabia, 2004–2012.
Most brucellosis cases were reported from March to August each year. Overall, April was the month with the highest number of reported cases; there were 4252 cases reported across the study period, where the peak of reported cases (579 cases) was in 2009. Across the study period, the average was 468.1 cases and the median was 486 cases in May. By contrast, November had the lowest number of reported cases, with 236 cases in 2004 and 263 cases in 2012. Across the study period, the average was 247.7 cases and the median was 263 cases in November (Fig. 4).
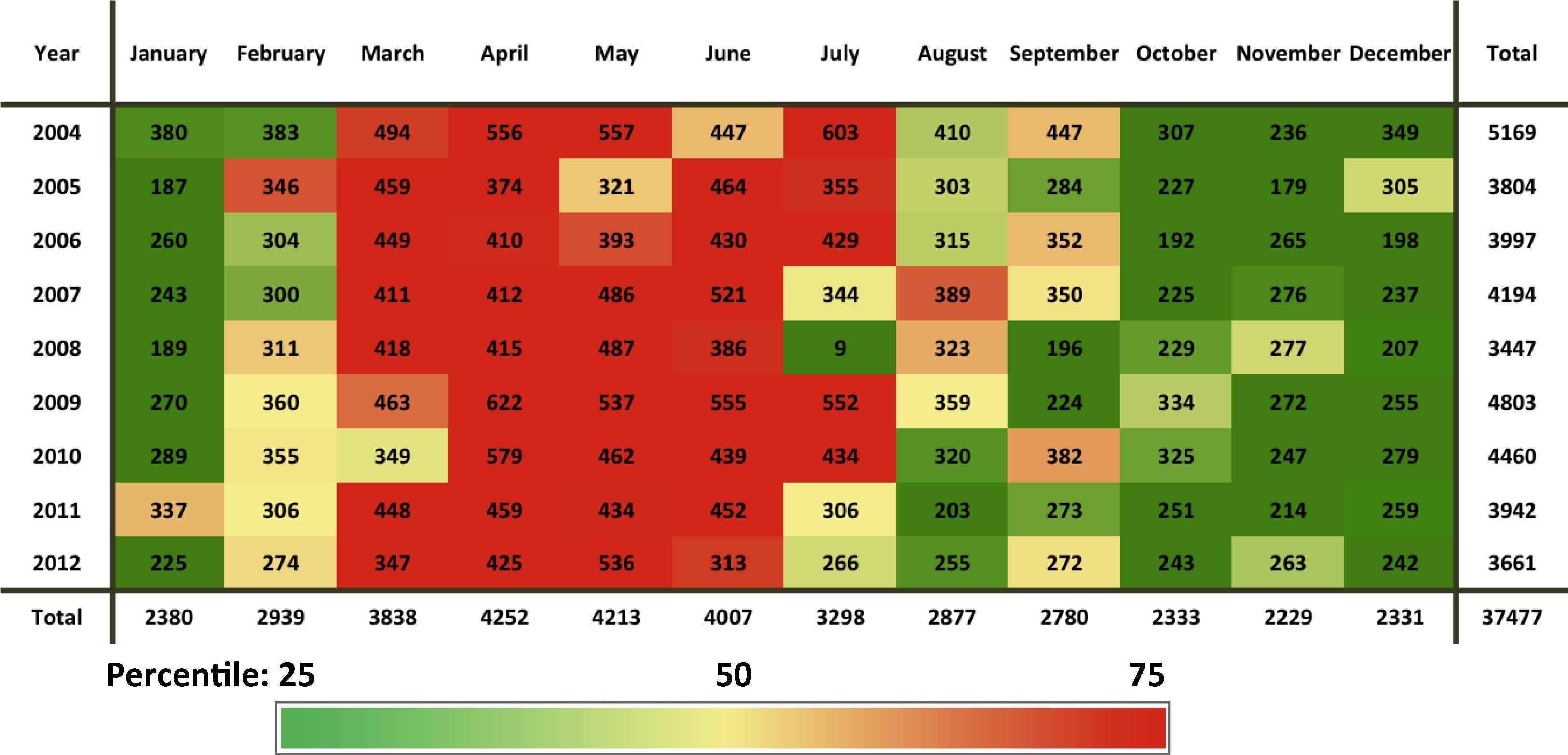
Reported cases of human brucellosis, by month of the year, Kingdom of Saudi Arabia, 2004–2012.
In Fig. 5, across the study period, the IR was higher in Al-Qassim, Aseer, Hail, Northern Borders, and Najran, with IRs >22. Although there was a relative decease in IR across the total period of study in the aforementioned regions, they still had the highest IR. IRs were relatively low in Al-Jouf, Jazan, Tabouk, Makkah, and Al-Riyadh, with IR <10, compared to other regions.
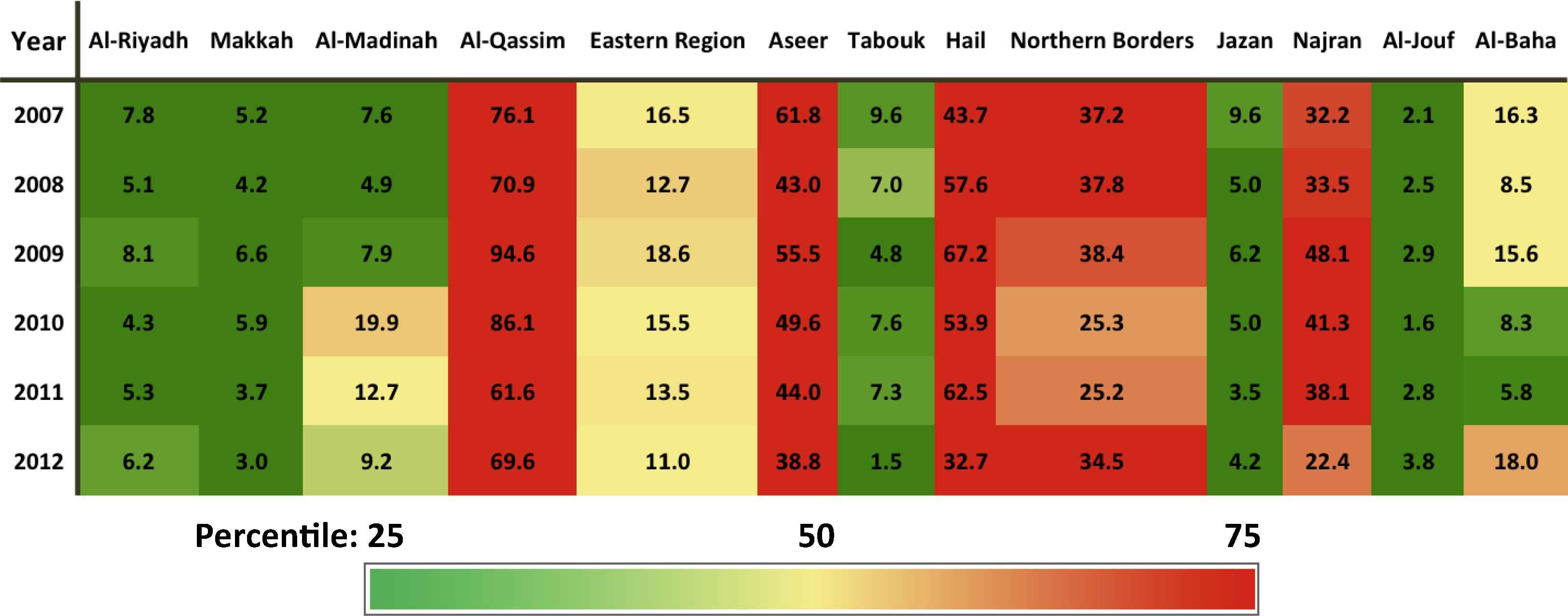
Incidence ratesa of reported cases of human brucellosis, by region, Kingdom of Saudi Arabia, 2007–2012. aPer 100,000 population.
4. Discussion
The results of this study show that brucellosis is a major health problem in KSA. From 2004 to 2012, the IR of brucellosis fell, but it was still higher than that of developed countries and most other developing countries. In KSA, male Saudi citizens aged 15–44 years were at the highest risk of acquiring this disease. This group may be more likely to come into contact with infected animals, as they travel more than women do and have more opportunities to drink raw milk during the spring and summer seasons.
The western part of KSA has the fewest number of cases compared to other areas, and Al-Qassim in the central part has the greatest number of cases, followed by Aseer in the south and Hail and Northern Borders in the north. Brucellosis is not confined to any one region; in other words, when a region is endemic for brucellosis, the disease can easily spread to neighboring regions. Enforcing livestock importation protocols is highly recommended to decrease the brucellosis IR among imported animals [8,13]. Regional variations could also be attributable to certain illness patterns. Entire families can be infected by a single source of infected milk, and young males often bring home fresh milk to their families.
Lifestyle differences among population subgroups can account for variable IRs of brucellosis. Generally, those infected with brucellosis have come into contact with infected animals or ingested unpasteurized or raw milk; also, laboratory workers are at risk when they deal with brucellosis samples, so it is considered an occupational disease.
We observed higher rates of brucellosis among males than females. Young Saudi males usually have more opportunities to drink unpasteurized or raw milk than females do. Men often go camping for days in the desert, and while doing so, they enjoy fresh milk provided to them by local shepherds. The fact that brucellosis is mainly an occupational disease (abattoirs and veterinarians) may be another reason why the prevalence is higher among males than females. The prevalence of brucellosis among those aged <14 years is lower than among other groups, most likely because children come into contact with infected animals less often than adults.
Our study has limitations that warrant discussion. First, the IR of age groups could not be calculated because the population data by age group was not available. Brucellosis cases are reported at the regional level and not by cities or governorates; therefore, determining the major foci of brucellosis was not possible. Second, the age spans of the groups were not equal, and the age span for adults was wide (15–44 years). We were not able to specify which people in this age group were affected the most.
Third, although we used the best available estimated population data, there were some inconsistencies in the published records. The main official source is the Saudi Central Department of Statistics and Information. Regional population data were not publically available, so the researcher used that which was found through the Saudi Department of Finance. Although yearly population growth was not taken into account by the Ministry of Finance from 2004 to 2012, growth was overestimated by the Saudi Central Department of Statistics and Information, which has a negligible effect on the yearly IR (to the 100th decimal place). The percentage difference in total population by gender across regions per year between the Ministry of Finance and the Saudi Central Department of Statistics and Information ranged from −5% to 0%.
Other important variables that play a role in brucellosis or could confound other variables were not available for inclusion in our analysis. Data such as brucellosis prevalence among shepherds, abattoirs, and laboratory workers are not kept by the KSA MoH. Other information such as an affect person’s location (urban or rural), occupation, level of education, social status, and income should also be included. Behavioral variables such as the role of milk collection, contact with animals, and how laboratory workers deal with samples should be included in future studies. Also, an assessment of how well animal importation protocols have been applied should be included, especially in areas where high numbers of animals are imported annually, such as Makkah.
5. Conclusion
Brucellosis still affects people’s health in KSA and causes economic losses. Our recommendations point mainly toward decreasing the brucellosis IR to zero. However, brucellosis is difficult to control in KSA, where high numbers of animals are imported each year, especially during the Hajj season. Also, there are many livestock owners living in rural areas who may not be aware of the risks attendant to their behavior. In addition, there is a large amount of uncontrolled livestock movement across the neighboring countries’ borders [13].
The main goal is to decrease brucellosis prevalence among humans and infection sources. Prevention measures should include: (1) implementing a governmental surveillance program for brucellosis prevention that: (i) creates a clearer case definition to capture all cases. This case definition should be more sensitive to make sure that health providers capture all suspected cases of brucellosis; (ii) organizes the flow of reported data from health centers, laboratories, and the IDD at the MoH so that it is smooth and fast; (iii) provides all health centers with the qualified laboratory personnel and equipment to capture all brucellosis samples; and (iv) takes samples frequently from susceptible livestock, especially those in potentially epidemic areas; (2) enforcing animal importation protocols; (3) enforcing compulsory vaccinations of all susceptible animals at veterinary clinics and agricultural offices; (4) increasing the level of education and awareness among people, especially people who are at risk, such as shepherds, those at abattoirs, and laboratory workers. Also, rural health centers should increase health awareness among people. Brucellosis cases were found mostly among uneducated people or those who had not completed secondary school [14]; (5) increasing the biosafety level in laboratories to level 3, as laboratory workers are at risk. Brucellosis is considered one of the most common laboratory-acquired infections. Even the centers not located in potentially epidemic areas should increase their biosafety level because laboratory personnel are usually not familiar with brucellosis samples and the disease’s clinical manifestations [15,16]; and (6) motivating researchers to do more studies of brucellosis in KSA, as most published papers do not cover the main distribution and determinant factors of brucellosis transmission in KSA in recent years. Also, the majority of published papers rely on the serology of the disease in humans and animals, which could lead to the disease’s underestimation.
The One Health approach is a concept connecting human health with that of animals and the environment, with the goal of building a healthy and safe environment for all. Building collaborations between medical personnel, veterinarians, and other environmental disciplines is also one of the aims of the One Health approach, as well as the prevention of potential disease outbreaks. The vaccinations of susceptible animals against brucellosis have resulted in a notable decline of brucellosis cases among humans and have lessened economic and livestock losses [17], but the disease still deserves attention and resources so it can be fully eradicated.
Conflicts of interest
All contributing authors declare no conflicts of interest.
References
Cite this article
TY - JOUR AU - Abdulaziz D. Aloufi AU - Ziad A. Memish AU - Abdullah M. Assiri AU - Scott J.N. McNabb PY - 2015 DA - 2015/10/01 TI - Trends of reported human cases of brucellosis, Kingdom of Saudi Arabia, 2004–2012 JO - Journal of Epidemiology and Global Health SP - 11 EP - 18 VL - 6 IS - 1 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2015.09.001 DO - 10.1016/j.jegh.2015.09.001 ID - Aloufi2015 ER -