
The remarkable adaptability of syndromic surveillance to meet public health needs
- DOI
- 10.1016/j.jegh.2012.12.005How to use a DOI?
- Keywords
- Syndromic surveillance; Outbreaks; International Health Regulations; Infectious diseases; Public health
- Abstract
The goal of syndromic surveillance is the earlier detection of epidemics, allowing a timelier public health response than is possible using traditional surveillance methods. Syndromic surveillance application for public health purposes has changed over time and reflects a dynamic evolution from the collection, interpretation of data with dissemination of data to those who need to act, to a more holistic approach that incorporates response as a core component of the surveillance system. Recent infectious disease threats, such as severe acute respiratory syndrome (SARS), avian influenza (H5N1) and pandemic influenza (H1N1), have all highlighted the need for countries to be rapidly aware of the spread of infectious diseases within a region and across the globe. The International Health Regulations (IHR) obligation to report public health emergencies of international concern has raised the importance of early outbreak detection and response. The emphasis in syndromic surveillance is changing from automated, early alert and detection, to situational awareness and response. Published literature on syndromic surveillance reflects the changing nature of public health threats and responses. Syndromic surveillance has demonstrated a remarkable ability to adapt to rapidly shifting public health needs. This adaptability makes it a highly relevant public health tool.
- Copyright
- © 2013 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Syndromic surveillance provides an indication of disease patterns, a method for detecting aberrations in health data, or a signal that an event of public health concern is occurring. Syndromic surveillance systems have been implemented since the 1990s, initially with a focus on bioterrorism event detection.
Last (2001) [1] defines a syndrome as: “A symptom complex in which the symptoms and/or signs coexist more frequently than would be expected by chance on the assumption of independence.” In surveillance terms, ‘syndromic’ relates to a specific set of symptoms not requiring laboratory confirmation for diagnosis. Common examples of syndromes used for syndromic surveillance include: acute flaccid paralysis (AFP), a syndrome potentially indicative of poliomyelitis; influenza-like-illness (ILI); or acute fever and rash, a syndrome potentially indicative of measles.
Syndromic surveillance captures a spectrum of approaches ranging from fully automated systems, using sophisticated statistical algorithms, to simple manual systems. It includes very specific case definitions for syndromes such as AFP to the generic counting of over-the-counter medications for coughs and colds. As it is based on clinical syndromes rather than laboratory confirmation, it is also potentially useful in settings where there is limited timely access to laboratories, including many developing countries [2]. As an approach, syndromic surveillance incorporates elements of data collection and analysis of specific syndromes or indicators (to detect disease), verification (that disease actually exists), information sharing (to those who need to know in order to respond), feedback to those who collected the data (to confirm that an action is occurring), and, in many recent cases, response and control measures to mitigate global health security threats.
Recent infectious disease threats such as SARS, avian influenza (H5N1) and pandemic influenza (H1N1) have highlighted the need for governments and public health agencies to rapidly learn of potential infectious disease threats to facilitate timely and appropriate public health responses. The requirement for improved early warning and response systems may be ‘reshaping’ global health surveillance [3]. The published literature on syndromic surveillance reflects the changing nature of these threats and responses. Over time, syndromic surveillance has been applied to a remarkable range of public health issues using a wide variety of data sources. Not only has it been used to collect data on particular disease syndromes, but it has also been used to monitor the public’s health following, or during, natural disasters, such as the Icelandic ash cloud, mass gatherings, heat waves, floods or pandemics.
This paper documents the evolution of syndromic surveillance from bioterrorist detection systems to those implemented for outbreak detection and response. By characterising the changing approaches used in syndromic surveillance, and the drivers for this change, it demonstrates the encouraging adaptability of syndromic surveillance and the important role it plays in public health.
2. Methodology
An analysis of published articles on syndromic surveillance was undertaken in published English-language literature to examine the evolution of syndromic surveillance. MEDLINE, EMBASE, Scopus and Web of Science databases were searched using the term “syndromic surveillance” for English language studies published prior to February 2012. After removing duplicates and non-English language articles, 415 records were obtained. Citations were downloaded into Endnote X4. Reference lists were then hand searched to obtain further relevant additional published articles and a total of 769 articles were thus included in the study.
To identify trends in the publication of syndromic surveillance articles, PubMed was searched for all articles with the term ‘syndromic surveillance’ in the title or abstract, as published in PubMed prior to 20 February, 2012; 214 articles were obtained and were downloaded into Endnote X4. This database was then searched to identify publication year for each article and the number of articles published each year. The database was further searched using the terms ‘bioterrorism’ and ‘influenza’ to identify articles published each year on these topics. Keywords assigned to these articles were extracted for the periods 2001–2004, 2005–2008, and 2009–2011, based on visual changes in the data, and these were imported into NVivo 9. Each of these time-periods was queried and a tag cloud created. Tag clouds represent by size the frequency of a particular word in a document, or in this case the frequency of keywords used in syndromic surveillance publications. The tag cloud used a Word search for the 100 most frequent words with the following characteristics: a minimum length of six characters; matching set to include stemmed words; and used the following Stop words – epidemiology, methods, statistics, and numerical – to reduce visual confusion in the tag cloud results.
3. Results and discussion
In this study, published literature was examined to assess the evolving usage of syndromic surveillance for public health purposes.
While generally acknowledged as a simplified view of the many approaches used in syndromic surveillance, predominantly two different approaches were commonly reported in the literature. The first is based on networked systems and encompasses the timely, automated extraction, using syndromic algorithms from an individual or multiple data sources, with alerts generated when there is an exceedance of a baseline threshold using statistical methods. The emphasis in this approach is on the timely, automated collection of data; the application of a syndromic algorithm to clinical or non-clinical data; the use of statistical methods to recognise that the data are exceeding a defined threshold or to monitor trends; and the generation of alerts to those who need to know so that a response can be implemented. This form of syndromic surveillance is traditionally associated with systems designed to rapidly detect bioterrorism events. An example is the Essence (Electronic Surveillance System for the Early Notification of Community-Based Epidemics), a bio-surveillance system used in the United States which uses aberration detection algorithms of syndrome groups, extracted from ICD-9 classification groups, to detect whether the observed count is above or below the expected count [4].
The second approach involved the regular, timely reporting of syndromic activity, based on agreed case definitions, at sentinel sites; detection of outbreaks, either based on an exceedance of historical data, or the reporting of syndromic cases in excess of the number clinicians would usually expect (which may include the reporting of unusual medical events); proportionate investigation and response; and regular feedback to concerned parties. The emphasis here was on both detection and response, with low technological requirements making it suitable for use in developing regions. An example of this is the syndromic surveillance system established in the Pacific Island Countries and Territories (PICT) [5].
3.1. Early application of syndromic surveillance in public health
The different approaches reflect the flexibility of syndromic surveillance to adapt to changing public health requirements and, while not truly linear in time, noticeable trends or themes are apparent in the literature. An exploration of the literature revealed that while public health surveillance was being discussed and implemented from the early 1960s, based on the visionary work of Langmuir [6] and Raska [7], with many of the principles developed then still applicable, the term syndromic surveillance only regularly entered peer-reviewed literature at the beginning of the twentieth century.
In the 1980s, the goal of global eradication of polio resulted in acute flaccid paralysis (AFP) surveillance being implemented globally as the key surveillance measure for the eradication of polio [8]. T. Jacob John also established a novel, district-level disease surveillance system in Southern India [9], which sought to control and limit disease outbreaks through early detection (described by a standardised set of symptoms); regular reporting and response; and would be termed a syndromic surveillance system if implemented today. This model included elements of data collection, analysis, confirmation, feedback and response – all key elements of modern-day syndromic surveillance. This approach was later further adapted in a rural African setting with a focus on rural hospitals reporting presentations of nine core clinical syndromes, including cholera and meningitis-like disease [10].
In the 1990s, the STD and HIV literature documented the value of syndrome-based diagnosis and treatment for case management purposes [11,12]. There were also some early examples of outbreak surveillance systems based on syndromes in developed countries. Among other examples, New York City implemented a syndromic surveillance system to detect outbreaks of waterborne illness using surveillance for diarrhoeal illness, stool submissions in laboratories and over-the-counter (OTC) pharmacy sales [13]; and public health officials in England compared data collected through a call centre (NHS Direct), using an algorithm for influenza-like symptoms, to routinely available surveillance data to assess the usefulness of syndromic surveillance for influenza surveillance [14].
3.2. Syndromic surveillance application in response to the bioterrorism threat
In the literature there was an apparent surge in interest in syndromic surveillance following the terrorist events in the United States of America, the United Kingdom and Spain, as well as the 2001 anthrax outbreak [15]. The word syndromic was applied because the majority of such systems monitored syndromes which might herald the early stages of epidemics [16]. Fig. 1 presents a graphic representation of the adaptability of syndromic surveillance as public health requirements for information have changed. A review of the published literature on syndromic surveillance shows the rapid growth in publications following the terrorist attacks, with the number of publications published each year peaking in 2004, after the emergence of SARS. These events appear to have accelerated the development of syndromic surveillance as a tool for the early identification of unexpected biological events [17].
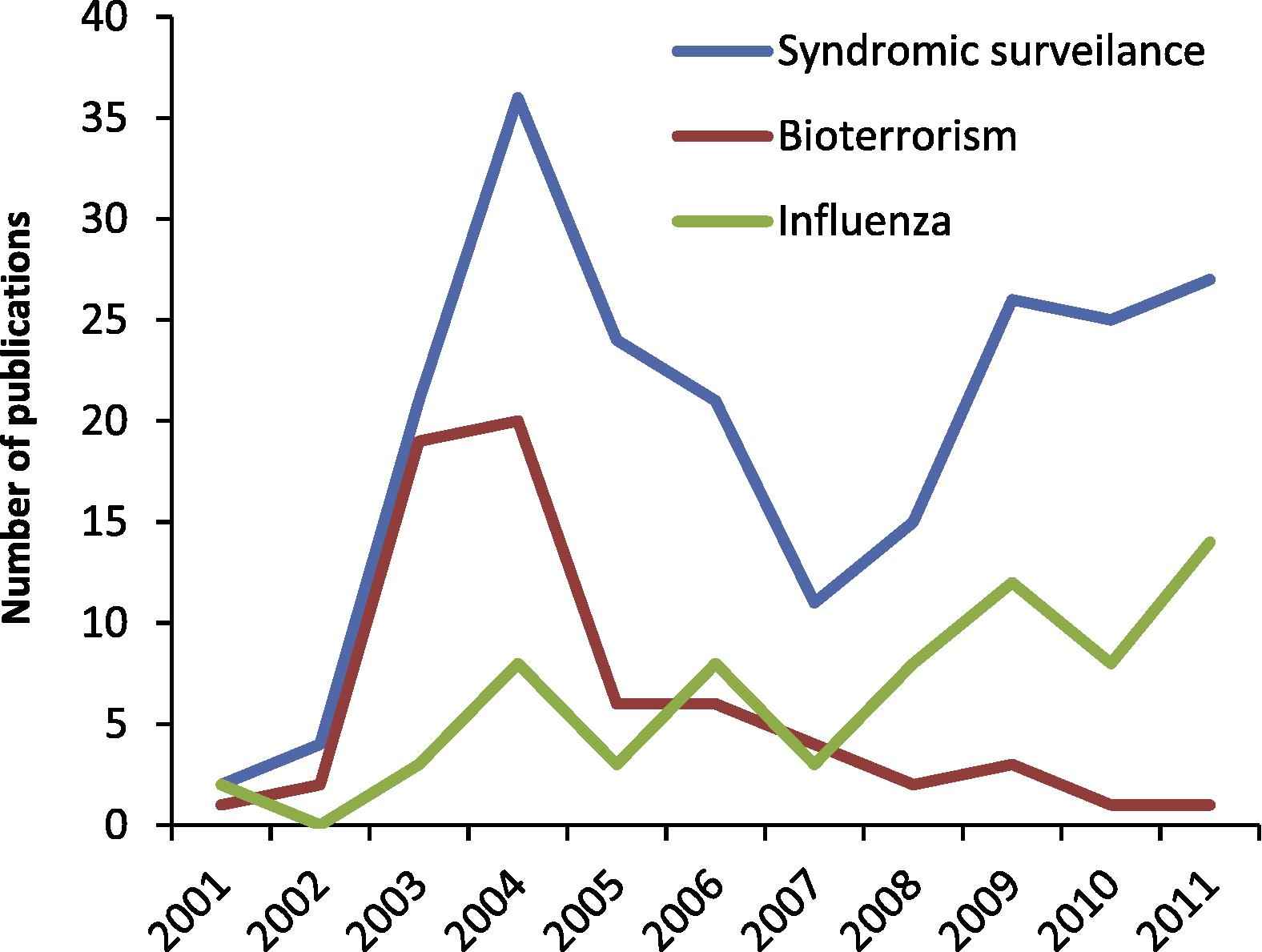
Trends in syndromic surveillance publications, 2001–2011.
3.3. Syndromic surveillance and emerging infectious disease threats
Fig. 1 demonstrates that from 2005 there was a decrease in the number of publications addressing bioterrorism and a shift in focus to emergent diseases and pandemics (with ‘influenza’ used here as a proxy indicator). A second wave of interest in syndromic surveillance is apparent from 2008 after the emergence of avian influenza and the 2009 influenza pandemic. Tag clouds, as shown in Fig. 2, highlight the predominance of bioterrorism as a keyword in syndromic surveillance publications from 2001 to 2004, and its lessening importance over time. In contrast, influenza and outbreaks increase in importance reflecting increasing public health activities in these two areas from 2005 to 2011.
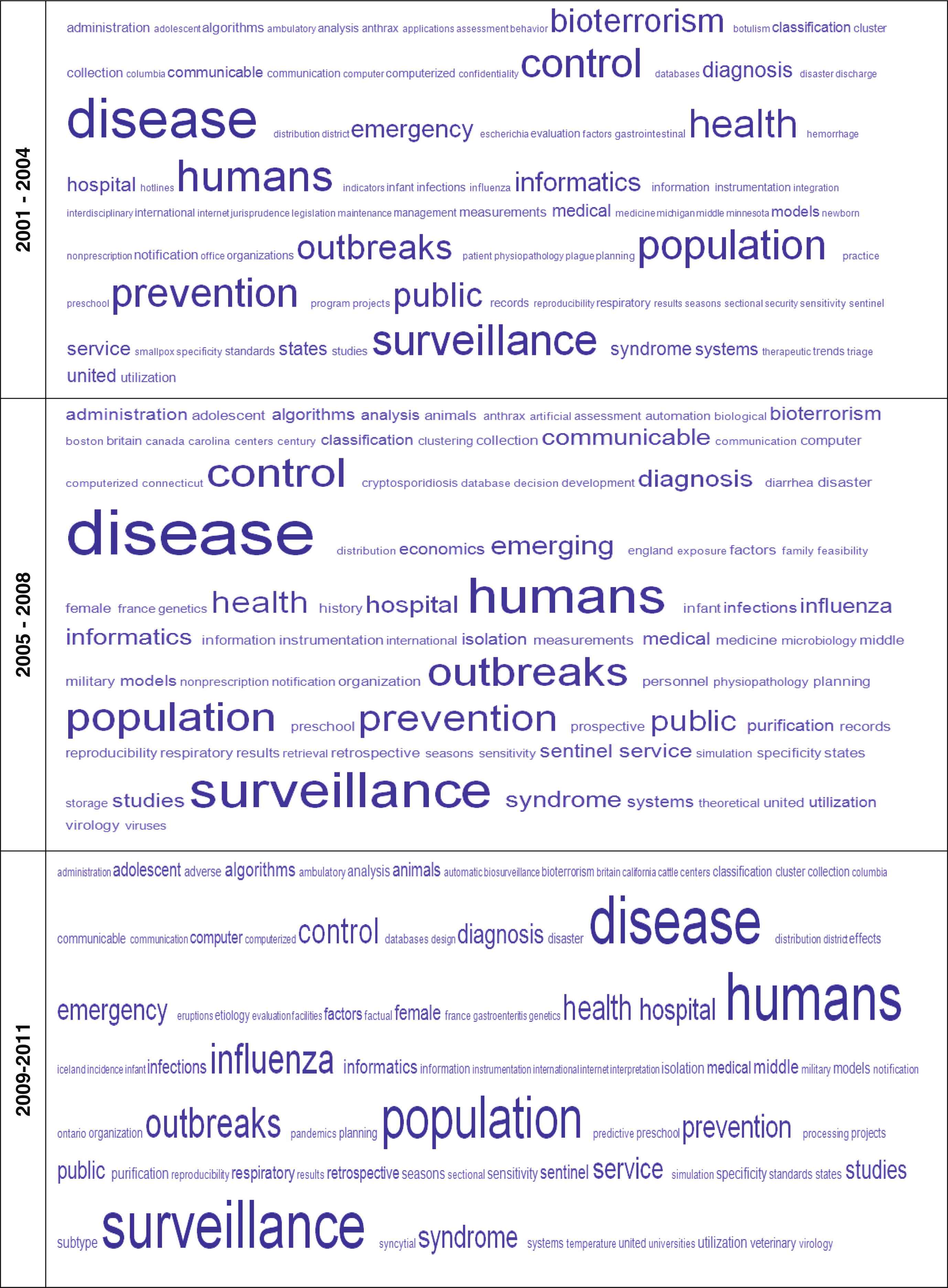
Tag clouds for keywords extracted from published literature on syndromic surveillance, 2001–2011.
Many recent emergent pathogenic infectious diseases have signalled their emergence through cases presenting with particular syndromes, such as encephalitis, influenza-like-illness (ILI) or severe acute respiratory syndrome (SARS), emphasising the importance of surveillance for syndromes as a method of detecting emergent diseases. The highly pathogenic Nipah and Hendra viruses presented as an encephalitic syndrome with a high case fatality rate [18,19]. The arrival of SARS in 2003 focused the world’s attention on emerging infectious diseases (EID) [16], the potential for an EID to cause “significant social and economic disruption,” and the need for early identification to limit further spread [20]. SARS was the first infectious disease event in modern times that confirmed how rapidly a deadly disease could spread across the globe and the subsequent cost to infected individuals and affected countries’ economies [21]. More recently, a syndromic approach first signalled a disturbing, unusual event occurring in Jordan when an apparent cluster of cases and fatalities from an unknown disease presented as a SARS with renal complications. It was only when this disease was finally identified, in a later case, as a novel coronavirus that the mystery behind the unusual cluster was solved [22]. Enhanced syndromic surveillance for further SARS presentation due to this novel coronavirus has currently been recommended at the global level by the World Health Organization [23].
The advent of SARS in 2003 led public health officials in developed economies to appreciate the potential benefits of syndromic surveillance to public health beyond bioterrorism and the possibility that it could be used to detect unusual disease clusters [24,25]. The influenza pandemic (H1N1) in 2009 also highlighted the need for surveillance systems able to provide early detection of first cases through the identification of patients with an ILI syndrome [26]. It also had value later during the pandemic; Elliott (2009) noted that when countries changed phase to ‘containment’, and were no longer able to laboratory confirm each case, then “syndromic surveillance takes precedence as the primary means of estimating the community burden of pandemic influenza infections [27].” As a result of the pandemic, and in an effort to improve public health surveillance, the CDC stated that it was “expanding and automating syndromic surveillance [28].”
3.4. Syndromic surveillance and the International Health Regulations
The 2005 IHR revision required all countries to develop certain minimum core public health capacities, including the ability to detect and respond to communicable disease outbreaks, and the rapid reporting of public health emergencies of international concern to the World Health Organization (WHO) [29]. Included in the IHR core capacity requirements are: “surveillance, reporting, notification, verification, response and collaboration activities [29].” The IHR obligation to report public health emergencies of international concern have raised the importance of early outbreak detection and response.
Standardised approaches to data collection, analysis, reporting, outbreak investigation and response are necessary for a surveillance system to effectively serve as an early warning system for biological, chemical or radiological threats. Evaluations of syndromic surveillance systems are necessary to confirm that they are able to meet public health requirements and obligations by adequately identifying outbreaks when they are occurring and, when an outbreak is detected, that there is an appropriate public health response [30,31].
For developing countries, where there are often long delays in laboratory confirmation, the implementation of simple syndromic surveillance systems may provide the opportunity to ensure a country’s early warning and response capacity [32]. The Pacific Island Countries and Territories (PICT) have developed a syndromic surveillance system to respond to an identified need for a functional surveillance system, capable of identifying and responding to outbreaks in a systematic manner, while taking account of limited local resources. In 2010, all PICTs agreed to implement a syndromic surveillance system to facilitate early warning and response, to meet these IHR obligations [33]. A further refinement was the development of ‘response protocols’ to standardise responses to outbreaks [34,35].
An evolving purpose of syndromic surveillance is to improve real-time ‘situational awareness’ which follows an outbreak from detection to response. Buehler et al. (2008) describe situational awareness as “the ability to monitor the course of outbreaks regardless of how they are detected,” and to “track, characterise and monitor trends [36].” The Centers for Disease Control and Prevention (CDC) (2010) describe the use of situational awareness for surveillance purposes as “public health professionals processing innumerable bits of data, assigning meaning, ascertaining significance, determining implications, and acting and adjusting accordingly.” Situational awareness reflects the notion that information for incremental decision-making does not just come from a single source and that syndromic surveillance can help to make sense of the “epidemiological puzzle [37].”
4. Conclusions
Syndromic surveillance has many applications in the public health field particularly, in recent times, for health security and the early detection of emerging health threats. Syndromic surveillance application for public health purposes has changed over time and reflects a dynamic evolution from the collection, interpretation of data, and dissemination of data to those who need to act; to a more holistic approach that incorporates response as a core component of the surveillance system.
The IHR obligation to report public health emergencies of international concern have accentuated the importance of early outbreak detection and response. Syndromic surveillance evolution has not been completely linear, but rather approaches have co-existed and evolved over time. The use of a syndromic surveillance approach to detect outbreaks and unusual patterns is not without its critics. Henning (2004) suggested cautious use of syndromic surveillance, noting that it should not replace traditional systems or the reporting by clinicians of unusual events [17]. Other challenges include the availability of resources for follow-up, movement of persons after exposure and the difficulty of detecting unusual events during seasonal increases in disease [15].
Using published literature to demonstrate the evolution of syndromic surveillance has some limitations, as the literature may not be representative of what is actually being implemented in public health programs. Publication bias and a lack of publications from the developing countries may also limit the validity of this approach.
Syndromic surveillance as applied to infectious diseases serves a wide number of purposes, including: early detection of threats and hazards, and a timelier public health response, identifying changes in severity of a particular disease, identifying emergent diseases, developing baselines or thresholds so that unusual occurrences can be detected, and demonstrating the effectiveness and progress of interventions. A number of authors have suggested that syndromic surveillance is appropriate for developing regions [32,38,39] particularly in view of the difficulties these areas have in receiving laboratory confirmations in a timely manner. The recognition that decision-making and public health responses are based on information from a range of sources has highlighted the value of syndromic surveillance to improve situational awareness.
Syndromic surveillance has demonstrated a remarkable ability to adapt to rapidly shifting public health needs and the flexibility to utilise different approaches depending on the situation. This adaptability makes it a highly relevant public health tool. Central to this is the public health requirement for credible, rapidly available surveillance information to allow informed decisions on responding to and controlling emerging threats.
References
Cite this article
TY - JOUR AU - Beverley J. Paterson AU - David N. Durrheim PY - 2013 DA - 2013/01/20 TI - The remarkable adaptability of syndromic surveillance to meet public health needs JO - Journal of Epidemiology and Global Health SP - 41 EP - 47 VL - 3 IS - 1 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2012.12.005 DO - 10.1016/j.jegh.2012.12.005 ID - Paterson2013 ER -