
Systolic and diastolic function as related to arterial stiffness
- DOI
- 10.1016/j.artres.2010.10.033How to use a DOI?
- Keywords
- Arterial stiffness; Wave reflections; Pulse wave velocity; Diastolic heart failure; Systolic heart failure
- Copyright
- © 2010 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
The function of the heart is necessarily linked to the function of the arterial system. The heart expels the blood, and the arteries serve as a conduit and a cushion between the heart and the microcirculation. This review aims to answer the questions—from a clinical cardiologist’s point of view—if and how impaired arterial function, particularly increased arterial stiffness (increased pulse wave velocity-PWV) and increased arterial wave reflections (increased pulse pressure-PP, increased augmentation index-AIx, increased pressure augmentation-AP) may impair cardiac function and ultimately lead to heart failure.
The first consideration is that increased arterial stiffness/wave reflections will increase pulsatile external work of the heart. As opposed to steady external work, which is useful for tissue perfusion, pulsatile external work is lost in the large arteries (and comprises normally, i.e. with compliant arteries, only 10 percent). Its increase may lead to “overload cardiomyopathy”.1 Epidemiological data confirmed that increased brachial PP, a crude surrogate for arterial stiffness, is associated with an increased risk for developing heart failure.2 Importantly, these data were obtained in a community-based sample of elderly (mean age 77.9 years) individuals, and the prognostic value of PP was independent of other predictors of HF. These data are particularly relevant to the topic, as both, the risk of heart failure on the one hand,3 and arterial stiffness on the other hand,4 exhibit a steep increase with age.
Next, increased arterial stiffness/wave reflections are associated with various maladaptive changes in structure and function of the left ventricle (LV). All of them may contribute—directly or indirectly—to the development of the clinical syndrome of heart failure (Fig. 1). Indirect contributors are structural changes of the LV and left atrium, namely LV hypertrophy and left atrial enlargement, furthermore the combination of functional (tendency towards ischemia in the setting of increased arterial stiffness/wave reflections) and structural (association of coronary atherosclerosis and increased arterial stiffness/wave reflections) impairments of LV perfusion. In addition, direct links between impaired arterial and LV function—among others a prolongation of relaxation in diastolic heart failure and an abbreviation of systolic ejection in systolic heart failure—have been found.
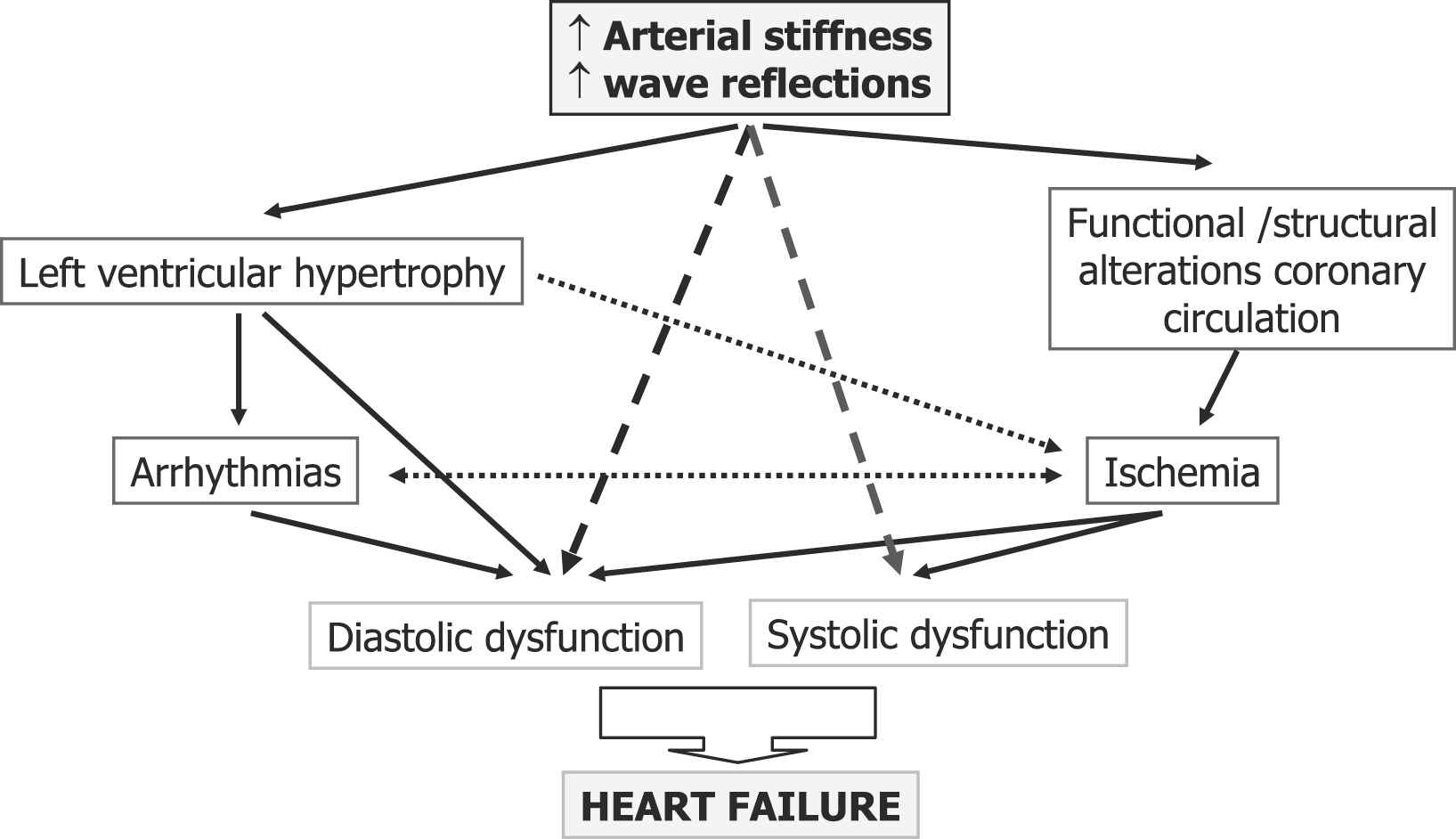
Possible pathways between increased arterial stiffness/pulse wave reflections and development of heart failure.
Indirect relationship between increased arterial stiffness/wave reflections and heart failure
a) Structural changes of the heart
Based on data from Framingham, it has been estimated that the presence of LV hypertrophy increases the risk of heart failure about 14-fould.5 An increase in pulsatile load may lead to LV hypertrophy. Accordingly, a positive relationship between AIx/PWV and LV mass has been demonstrated repeatedly.6,7 LV relative wall thickness and mass index is more strongly related to central than to peripheral blood pressures.8 The most unfavourable—concentric—phenotype of LV hypertrophy is associated with PWV,9 particularly in elderly patients. In newly treated hypertensive patients, the treatment-induced change in LV mass was closely correlated with measures of wave reflection (AIx, AP, Amplification), but not with brachial blood pressures.10 Similarly, the change in LV mass between two different antihypertensive drug regimes was significantly linked to central, but not to brachial blood pressures.11
But also the left atrium is of importance: in subjects ≥ 65 years with additional risk factors for atrial fibrillation (but in sinus rhythm at the time of investigation), 1 standard deviation (SD) increases in aortic PP, brachial PP, PWV, and AP were associated with 6%, 6%, 4%, and 4% increases in indexed left atrial volume, respectively, even after adjustment for age, gender, and clinical and echocardiographic covariates.12 This enlargement of the left atrium may serve as the substrate for the increased risk of atrial fibrillation. Indeed, brachial PP was associated with increased risk for atrial fibrillation (adjusted hazard ratio1.26 per 20-mm Hg increment) in models adjusted for age, sex, baseline and time-dependent change in mean arterial pressure, and clinical risk factors for atrial fibrillation (body mass index, smoking, valvular disease, diabetes, electro-cardiographic LV hypertrophy, hypertension treatment, and prevalent myocardial infarction or heart failure) in the Framingham Heart Study.13 In contrast, mean arterial pressure was unrelated to incident atrial fibrillation. With respect to potential therapeutic implications it should be noted that in a placebo-controlled study in patients with isolated diastolic dysfunction, a reduction in AIx was associated with a decrease in indexed left atrial volume, independent of changes in systolic blood pressure.14 Clinically, the ill effects of the development of atrial fibrillation in patients with systolic as well as diastolic heart failure are well known. With regard to the latter, even the diagnosis of the condition can rely heavily on the presence of the arrhythmia.15
b) Ischemia
In a stable clinical situation, the link between ischemia and cardiac function is well described by the ischemic cascade16: initiated by an imbalance between myocardial oxygen demand and supply, firstly metabolic changes develop, followed by diminished left ventricular compliance (diastolic dysfunction), decreased myocardial contractility (systolic dysfunction), electro-cardiographic changes and finally symptoms. Hence, the impact of ischemia on LV function always has to be considered, and, within the context of this review, the relationship between arterial stiffness/wave reflection and ischemia, which may be seen as an interplay between anatomical and functional factors:
Although traditionally, arteriosclerosis (arterial stiffening, a disease primarily of the arteries media) and atherosclerosis (a disease primarily characterized by intimal plaque development and progression) have been considered as being two different entities, possibly linked by association,17 in the last years more than 15 cross-sectional studies have been published, showing consistently a significant association between PWV and coronary atherosclerosis and/or coronary artery calcium.18–20 Invasive21 as well as non-invasive22 studies have confirmed the relationship between increased/premature wave reflections, quantified as AIx/AP, and the presence as well as the extent of coronary atherosclerosis as well, although this may be closer in patients up to the age of 60 years. Moreover, an association between extracoronary atherosclerosis and increased wave reflection has been shown.23
In addition to these anatomical factors, the functional component is of importance as well: an increase in aortic stiffness leads to increase in pressure throughout systole, both from stiffening of the proximal aorta and early return of wave reflection, and to decrease in diastolic blood pressure. Increase in pressure throughout systole increases tension time index, LV load and, thus, LV oxygen requirements. Decrease in diastolic pressure decreases the driving pressure gradient for coronary perfusion (diastolic aortic pressure minus right atrial pressure). The net result is a tendency towards ischemia, that can be worsened in the presence of diastolic dysfunction with corresponding elevated LV filling pressures, further compromising the diastolic pressure gradient for coronary perfusion,24 ending up in a vicious cycle, as ischemia may further deteriorate diastolic function. In hypertensive patients, transient myocardial ischemia, as detected by ST-segment depression during ambulatory monitoring, was associated with increased PWV.25 Still, the situation may be compensated until coronary artery disease develops. It has been shown in a group of patients with moderate (1 and 2 vessel disease, mean stenosis grade 84%) coronary artery disease that PWV as well as AIx were inversely correlated with the time until ischemia developed during exercise testing, and the inverse relationship for AIx was true even after adjustment for cardiovascular risk factors and the severity of coronary artery stenosis.26 In an invasive study in 18 patients undergoing elective percutaneous coronary interventions, resting and adenosine-induced hyperaemic coronary blood flow was measured before and after stent implantation using a Doppler velocity guide wires, and compared with aortic stiffness (PWV and central pulse pressure). The investigators observed a highly significant, inverse association between resting and hyperaemic coronary blood flow and aortic stiffness and concluded that a stiff aorta is associated with a reduction in coronary blood flow, a lower hyperaemic coronary blood flow response, and may reduce the improvement in hyperaemic blood flow after successful coronary intervention.27
Direct relationship between arterial stiffness/wave reflection
a) Diastolic heart failure
Epidemiologically, diastolic heart failure is most prevalent among elderly women, most of them have hypertension, diabetes, or both and often coronary artery disease.28 These comorbidities exactly resemble conditions with increased arterial stiffness/wave reflections, raising the question how unfavourable changes of the mechanical properties of the arterial system may be involved in the pathophysiology of the disease, given the obvious argument that the heart is coupled to the arterial circulation and the increased pulsatile load only when the aortic valve is open, i.e. during systole. However, it has been observed first by physiologists that the time of onset of diastole29 and the duration of relaxation30 depends on systolic load. In open-chest dogs, the influence of the systolic LV pressure waveform on the rate of isovolumetric LV pressure fall, as assessed by the time constant tau, was examined.31 By inflating an intra-aortic balloon, increases in LV pressure of 2–20 mm Hg could be produced, which led to a prolongation of tau. Importantly, the rate of LV pressure fall slowed significantly more when LV pressure was increased in late than in early systole. The authors explained the findings with delayed cross-bridge inactivation due to late systolic loads. Similar results could be obtained in patients during heart catheterization32: Compression of both femoral arteries led to a measurable increase of wave reflection in these patients. In younger patients, the reflected wave arrived at the ascending aorta after aortic valve closure, and relaxation shortened. In contrast, in elderly patients, the increased reflected wave arrived in late systole, and relaxation was prolonged.
In untreated patients with essential hypertension, wave reflections (AIx) were independent and additive determinants of LV diastolic dysfunction, as diagnosed by Doppler-echocardiography.33 In a series of 235 consecutive patients with normal systolic function undergoing coronary angiography, patients were categorized as having normal diastolic function or diastolic dysfunction, based on invasively measured filling pressures and natriuretic peptides.34 Patients with diastolic dysfunction had higher wave reflections (AP), as compared to controls. In addition, a prolongation of ejection time, indexed to heart rate (LVETI), was noted in diastolic dysfunction. LVETI was able to differentiate diastolic dysfunction patients from controls as good as echocardio-graphically determined filling pressures (E/E′), which—according to the latest recommendations15—constitute the mainstay of the diagnosis of diastolic heart failure in clinical routine. In a study in 48 patients, the impact of arterial load and loading sequence on left ventricular tissue Doppler velocities was assessed.35 All measures of pulsatile load, including PWV, characteristic impedance, total arterial compliance, and AIx were inversely related to early diastolic velocity, but late systolic load (AIx) had the strongest relationship. In multivariable analysis, only AIx and characteristic impedance significantly predicted E′, even after adjustment for age. These data were corroborated in 336 middle-aged and elderly patients.36 Moreover, filling pressures, either measured invasively or estimated using the E/E′ ratio, were significantly associated with increased wave reflections and PWV. All associations were independent of age and gender. In that study, patients suffering from exertional dyspnea had increased AIx, AP, and PWV. The clinical consequences were further evaluated in detail in a study that used magnetic resonance imaging for estimation of aortic stiffness: in the proximal ascending aorta, area changes between end-diastole and end-systole were measured and related to brachial pulse pressure to determine distensibility. Both (area change and distensibility) were lower in old versus young healthy individuals and were lowest in old patients with diastolic heart failure. In addition, a high-grade correlation (r = 0.79) was found between the distensibility of the aorta (the opposite of stiffness) and peak oxygen consumption during an exercise test.37 This relationship was independent of age and gender in multivariable analysis. The associations between diastolic dysfunction/heart failure and increased PWV/increased central pressures have been confirmed in a series of recently published studies38–43(Table 1).
| Author (Reference) | Journal Publication year | n | pPP | cPP | AIx | cfPWV |
|---|---|---|---|---|---|---|
| Kang38 | Eur Heart J 2010 | 1764 | na | na | na | ↑ (baPWV) |
| Desai39 | J Card Fail 2009 | 53 | na | ↑ | ↔ | ↑ |
| Yambe40 | Hypertens Res 2004 | 147 | na | na | na | ↑ (baPWV) |
| Abhayaratna41 | J Hypertens 2008 | 233 | ↑ | ↑ | na | ↑ |
| Sharman42 | Am J Cardiol 2007 | 155 | ↔ | ↔ | ↔ | na |
| ↑a | ||||||
| Ikonomidis33 | J Hum Hypertens 2008 | 163 | ↔ | na | ↑ | na |
| Weber34 | Heart 2006 | 235 | ↑ | ↑ | ↑ | na |
| Kawaguchi43 | Circulation 2003 | 58 | ↑ | na | na | na |
pPP-peripheral pulse pressure; cPP-central pulse pressure; AIx-Augmentation Index; cfPWV-carotid-femoral pulse wave velocity; baPWV-brachial ankle pulse wave velocity.
elevated filling pressures.
Recent studies investigating the association between diastolic dysfunction/diastolic heart failure and measures of arterial stiffness/wave reflections.
What may be the therapeutic consequences of these findings? In the absence of randomized data, preliminary information can be drawn from a large study in high-risk hypertensives (ASCOT-BPLA). In that study,44 treatment with atenolol/thiazid was tested against the combination amlodipine/perindopril. The latter combination led to improved clinical outcomes, that may be due to the better control of the central systolic blood pressure throughout the study in the calcium-channel-blocker/ACE-inhibitor arm.45 In contrast, brachial blood pressures were well matched during the study period. Another ASCOT-substudy46 investigated diastolic function. At year 1, again for the same level of brachial systolic blood pressure, diastolic function, based on Doppler-and tissue-Doppler-echocardiography and natriuretic peptides, was better and filling pressures were lower in the calcium-channel-blocker/ACE-inhibitor arm, again suggesting a causative role for control of central systolic blood pressure.
b) Systolic heart failure
In systolic heart failure, we are faced with sometimes paradoxical results of observational studies: A higher brachial PP has been associated with a shorter47 survival in patients with severely impaired systolic function (mean EF 27%), but in relatively good functional class. On the other hand, in advanced chronic heart failure (NYHA III/IV) at the same level of systolic dysfunction (mean EF 26%), a higher brachial PP was associated with a longer48 survival. Although this cannot be quickly resolved, analysis of the pressure waveform may lead to further insights. It has been known for years that the arterial waveform undergoes relatively dramatic changes in the setting of severely impaired systolic function.1 Instead of showing the late systolic peak that is typical for elderly individuals, the aortic pressure curve shows a single rounded systolic peak as in young healthy adolescents, and a prominent diastolic wave. In addition, there is a progressive decrease in ejection duration with decreasing contractility, even after correction of any increase in heart rate, and a change in flow wave contour with early deceleration of aortic flow and, ultimately, abbreviation of systolic duration with fall in stroke volume.49 The most likely explanation is that the effects of wave reflection, which normally adds to pressure but subtracts from flow, in the situation of myocardial failure, are far more pronounced on flow (i.e. reduction) than on pressure. The failing LV is not able to cope with the reflected wave, and ejection of blood stops early. Supporting the concept, pulsatile hemodynamics have been studied invasively in 17 heart failure patients with severely impaired systolic function (mean EF was 27%) and in 11 controls matched for age, gender and mean blood pressure, with vasodilators withheld at least for 48 h. Simultaneous acquisition of high-fidelity pressure and flow enabled calculation of characteristic impedance, forward and reflected wave amplitude and their amplitude ratios. Results confirmed that wave reflection per se was not different between patients and controls.50
The difference in aortic pressure waveforms between patients with cardiomyopathy and controls has been observed in a number of clinical studies51–53: AIx and AP are lower, ejection duration is shorter in cardiomyopathy. On the opposite, PWV is not different from controls in most of the studies,51,52 or higher in patients with ischemic cardiomyopathy only.54 However, a higher pulsatile load may be detrimental in systolic heart failure: in patients with dilated cardiomyopathy, an inverse relationship between arterial stiffness (aortic PWV) and exercise capacity (peak exercise oxygen uptake) has been shown repeatedly.55,56
Conclusions and future directions
As outlined, increased arterial stiffness and wave reflections are involved in the pathogenesis of heart failure through various direct and indirect mechanisms. Vasodilators, the logical treatment to reduce wave reflections and—by lowering mean arterial pressure—arterial stiffness, are of proven clinical benefit in systolic heart failure, although the evidence is less clear in diastolic heart failure. However, therapeutic trials targeted directly towards a decrease of arterial stiffness/wave reflection are currently lacking. Moreover, the diagnostic potential of measures of arterial stiffness/wave reflection in heart failure remains largely to be studied.
References
Cite this article
TY - JOUR AU - Thomas Weber PY - 2010 DA - 2010/11/05 TI - Systolic and diastolic function as related to arterial stiffness JO - Artery Research SP - 122 EP - 127 VL - 4 IS - 4 SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2010.10.033 DO - 10.1016/j.artres.2010.10.033 ID - Weber2010 ER -