
Inflammation and arterial function☆
Disclosure of interest: There is no conflict of interest. Source of funding: None.
- DOI
- 10.1016/j.artres.2007.03.005How to use a DOI?
- Keywords
- Inflammation; Arterial stiffness; Wave reflection; Endothelial function
- Abstract
During the last decade, several studies have documented the unfavourable effects of inflammation on cardiovascular function and its role in the pathophysiology of atherosclerotic disease. The interplay between inflammation and arterial system is multifaceted. On the one hand, the endothelium contributes to the initiation and the perpetuation of vascular wall inflammation. On the other hand, the inflammatory cascade affects adversely the endothelium-dependent processes and the mechanical properties of the arteries. These effects give rise to impaired vasomotion, arterial stiffening and increased wave reflections and thus result in an unfavourable haemodynamic loading of the heart. Chronic inflammatory diseases (such as rheumatoid arthritis, and others) as well as acute inflammatory stimuli (such as acute infections) may adversely influence the arterial performance. Moreover, systemic subclinical low-grade inflammation, as expressed by high circulating levels of inflammatory markers/mediators, is a common denominator of most cardiovascular risk factors (hypertension, diabetes, etc.) and importantly, it is closely related to impaired arterial elastic properties. In addition, vasculogenic erectile dysfunction, which comprises an alternative phenotype of arterial dysfunction and an emerging cardiovascular risk predictor, is accompanied by low-grade inflammatory activation. Among the several inflammatory markers/mediators, level of C-reactive protein has been consistently associated with indices of arterial function in several populations. However, data regarding a possible direct etiological role of C-reactive protein in arterial dysfunction and atherosclerosis, if any, are yet inconclusive. Current evidence suggests that anti-inflammatory strategies benefit arterial function in several clinical settings. Further research is needed to elucidate whether inflammation may comprise a worthwhile treatment target with regard to the cardiovascular system.
- Copyright
- © 2007 Published by Elsevier B.V. on behalf of Association for Research into Arterial Structure and Physiology.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
General considerations
Arterial function is a crucial determinant of the overall cardiovascular (CV) performance. Several studies indicate that arterial stiffness, wave reflections and endothelial function are associated with the presence and extent of CV disease, and moreover, that they are independent predictors of outcomes in several populations.1–4 Importantly, the recent Conduit Artery Function Evaluation (CAFE) study5 indicated that arterial function may comprise a worthwhile treatment target. In this study, the improvement of central haemodynamic indices after treatment was accompanied by reduced CV events, independent of peripheral blood pressure changes. In addition, the concept of “vascular age” as a risk stratification tool gains ground, and studies such as the recent Anglo-Cardiff Collaborative Trial6 and the European Project on Genes in Hypertension,7 which defined normal values of arterial indices, will undoubtedly facilitate the implementation of arterial stiffness in everyday clinical practice.
Atherosclerosis is currently recognized as an inflammatory disorder. Indeed, low-grade inflammation contributes to all stages of atherosclerosis, from the initial phase of increased endothelial permeability up to the formation of the mature atherosclerotic plaque and plaque rapture.8 Furthermore, accumulating data suggest that there is also an important link of clinically manifested inflammation, as in chronic inflammatory diseases or acute infectious disorders, with CV disease. Considering that arterial dysfunction indicates the presence and mediates the progression of CV disease and also predicts outcomes, current evidence with regard to the association of the different types of inflammation with arterial performance is of great interest, both in pathophysiological and clinical grounds.
Subclinical, low-grade inflammation and arterial function
It is established that subclinical low-grade inflammatory activation, as expressed by high circulating levels of inflammatory markers/mediators, is a common denominator of most CV risk factors. In diabetic patients, levels of C-reactive protein (CRP) and serum amyloid-A, and white blood cell count are related to increased arterial stiffness.9 Notably, a relationship between abdominal adiposity and low carotid distensibility has been observed in diabetic patients, and this is fully accounted for by the increased levels of CRP and interleukin-6 (IL-6).10 Similarly, in subjects with metabolic syndrome, there is a close association of arterial stiffness with the amount of subcutaneous fat, a tissue that is largely involved in the synthesis of proinflammatory cytokines.11 Likewise, carotid–femoral pulse wave velocity (PWV), a measure of aortic stiffness, is related to the level of CRP in hypercholesterolaemic patients.12
The relation of arterial elastic properties with subclinical inflammation has also been studied in hypertensive populations. Our group and other investigators have observed that stiffness of large, elastic-type arteries deteriorates in parallel with increasing levels of CRP in hypertensive patients.13,14 Moreover, we also observed that CRP is associated with stiffness of medium, muscular-type arteries, as expressed by the carotid–radial PWV.13 Concerning augmentation index (AIx), which is a composite index of wave reflections integrating arterial stiffness, peripheral vascular tone and characteristics and cardiac contractility, data regarding associations with CRP are not consistent.13–15 The relation of inflammation with stiffness in hypertension has been further highlighted by a recent study showing that patients with low level of adiponectin, a cytokine with anti-inflammatory and atheroprotective properties, have high aortic stiffness.16 Furthermore, we have observed that the plasma level of fibrinogen, which is a procoagulant substance that also reflects the degree of inflammatory activation, is an independent determinant of large elastic artery stiffness in untreated hypertensives.17
During the last years, there is a growing interest on vasculogenic erectile dysfunction, since this syndrome is regarded as an alternative phenotype in patients with generalized arterial disease, and moreover it is independently related to increased cardiovascular events. Recently, we investigated the link between subclinical inflammatory activation and erectile dysfunction in men. We observed that erectile dysfunction is associated with higher levels of inflammatory markers/mediators, such as CRP, IL-6, IL-1β and tumor necrosis factor-α (TNF-α) (Fig. 1).18 For most of these markers, we found no interaction between vasculogenic erectile dysfunction and presence of angiographically documented coronary artery disease, implying that the combination of erectile dysfunction and coronary artery disease is associated with higher levels of such markers, on top of CAD alone.18 Interestingly, we observed a significant inverse linear correlation between level of CRP and erectile performance, as expressed either by the score of the five-item form of the Sexual Health Inventory for Men or by the pharmacologically stimulated peak systolic velocity of penile arteries.18,19 These findings offer an inflammatory basis to support the increasingly recognized notion that erectile dysfunction is an expression of a generalized arterial defect rather than a local phenomenon.
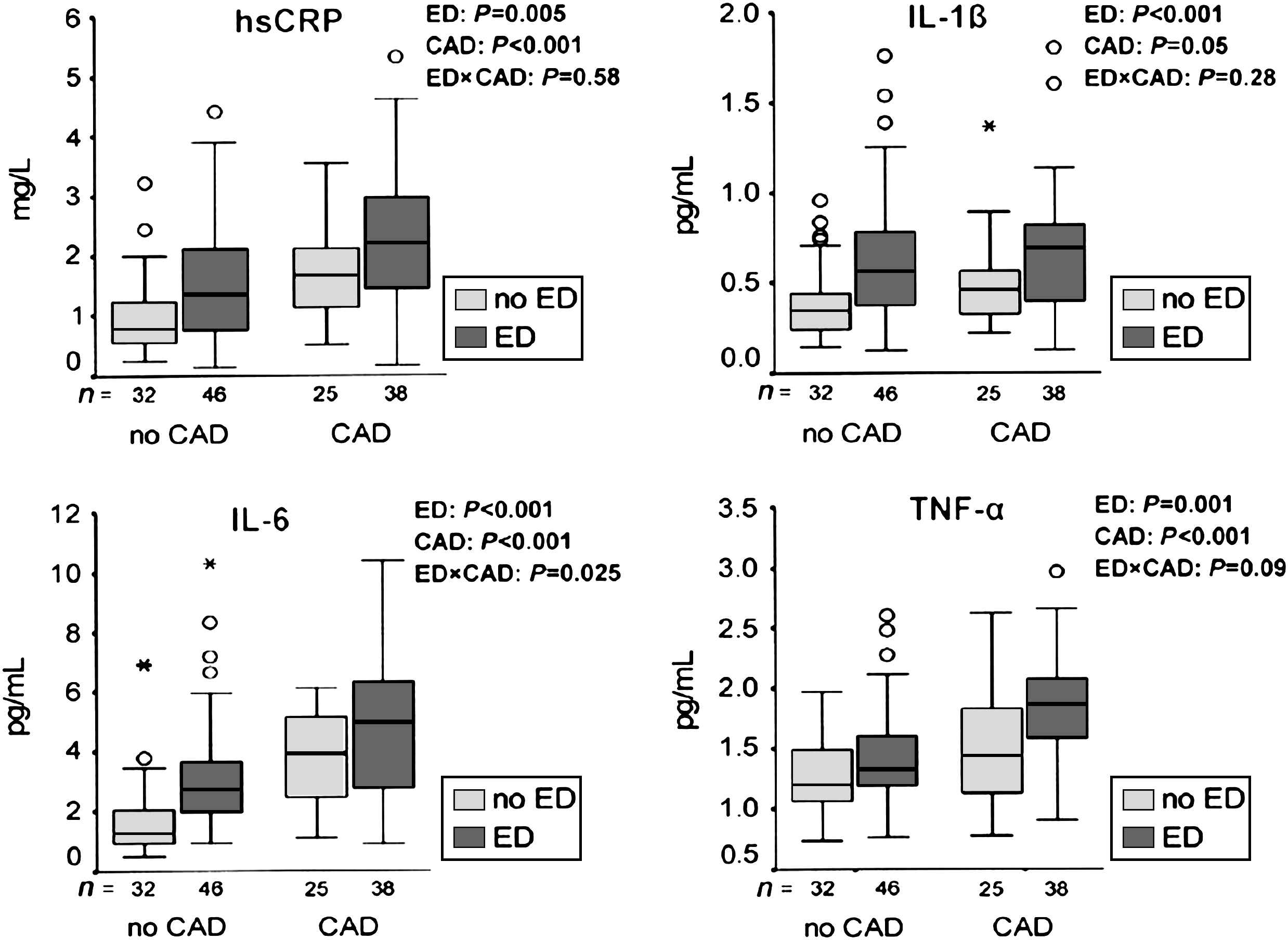
Levels of inflammatory markers/mediators according to the presence of erectile dysfunction (ED) and coronary artery disease (CAD). Probability values for ED indicate that ED is associated with significantly higher level of these markers. Probability values for ED × CAD interaction indicate that for the majority of these markers (except IL-6), the combination of ED and CAD is associated with a more intense inflammatory activation compared with CAD alone. Reprinted with permission from Vlachopoulos et al.18
Associations between inflammatory compounds and arterial function have been observed even in the general population and in apparently healthy subjects, who are supposed to have the lowest degree of low-grade inflammatory activation. In such populations, CRP level has been related to pulse pressure, stiffness of elastic and muscular arteries and central wave reflections.20,21 Furthermore, circulating level of matrix metalloproteinase-2 (MMP-2) is inversely associated with carotid–femoral PWV in healthy persons.22 In contrast to subjects with CV risk factors,23 it seems that in healthy, low-risk populations without the activation of low-grade inflammatory mechanisms, a higher MMP-2 level probably reflects a higher availability of nitric oxide (NO, a molecule with anti-inflammatory properties)24 and more physiological extracellular matrix turnover, and thus it is associated with a lower aortic stiffness. Finally, we have observed that in healthy individuals, a readily available test such as white blood cell count may independently explain a greater amount of the variation of AIx than CRP.25
Occult persistent infections represent another type of subclinical inflammation that may also coexist with impaired arterial function. In particular, Chlamydia pneumoniae seropositivity has been related to augmented arterial stiffness and aortic wall thickness even in asymptomatic children, indicating an adverse impact on vascular structure and function.26 Although recent studies showed that antibiotic therapy targeting these microorganisms does not reduce the incidence of CV disease, the debate on the significance of such infections for the initiation of atherosclerosis still continuous.
Chronic inflammatory diseases and arterial function
Cardiovascular disease is one of the leading causes of morbidity and mortality in patients with chronic inflammatory disorders. Recent studies have highlighted the close association between the level of inflammatory activation and impaired arterial performance in such patients. In rheumatoid arthritis, chronic inflammation affects adversely arterial stiffness, aortic haemodynamics and the performance of small arteries.27–29 Interestingly, as the majority of deaths in patients with rheumatoid arthritis are related to CV events, these data suggest that impaired arterial function may mediate a part of the increased CV risk of rheumatoid arthritis. In addition, arterial elastic properties are impaired in patients with systemic lupus erythematosus27 or autoimmune systemic vasculitis.30 In children with Kawasaki syndrome, arterial stiffness and wave reflections are increased,31 presumably because the vasculitis is not confined to coronary arteries but also affects other arterial beds. Furthermore, vascular function is compromised when inflammatory activation caused by chronic infections is present. In particular, HIV-infected subjects have impaired peripheral artery endothelial function as expressed by brachial artery endothelium-dependent vasodilation.32
In Athens Medical School we have studied patients with Adamantiades-Behcet’s disease, a relapsing autoimmune inflammatory disorder of unknown etiology, which may serve as a model of chronic inflammation. This disorder is characterized by recurrent oral and genital ulcerations and a high incidence of CV manifestations, due to systemic vasculitis. We observed that these patients have impaired endothelial function, as expressed by the endothelium-dependent, flow-mediated dilation of the conduit brachial artery.33 Moreover, in subjects with Adamantiades-Behcet’s disease not taking corticosteroids, aortic AIx is higher compared to control subjects,34 thus indicating an unfavourable effect of the chronic inflammatory activation on central haemodynamics. Interestingly, patients with a high aortic AIx have left ventricular diastolic dysfunction, thus establishing a link between abnormal arterial function and impaired cardiac performance in this syndrome.35
Acute inflammation and arterial function
Apart from the link between chronic inflammation and atherosclerosis, accumulating data suggest also an association of acute inflammatory responses, as during an acute respiratory or urinary tract infection, with a short-term increased risk for a cardiovascular event.36 Regarding the arterial effects of acute inflammatory stimuli, earlier studies had found that infusion of proinflammatory cytokines in forearm arterial bed induces a transient and reversible endothelial dysfunction. Recent observational studies that employed more “physiological” inflammatory stimuli, showed that an acute respiratory infection may impair endothelial function for at least 2 weeks.37 Our knowledge on the vascular effects of acute inflammation has been enriched by a group of studies using a validated vaccination model (Salmonella typhi vaccine) that elicits an acute, systemic, subclinical, transient and reproducible inflammatory response. The investigators who first used this model for arterial studies have consistently found that the vaccine impairs both conduit brachial artery and resistance artery endothelial performance in healthy humans.38–40 All the above studies had targeted endothelial function and until recently, no data regarding the effect of acute inflammation on arterial elastic properties were available. By using the same validated vaccine model, we observed that even a subclinical acute inflammatory stimulus may impair the stiffness of large elastic arteries such as the aorta, as expressed with an increase of carotid–femoral PWV.41 This increase of aortic stiffness in our study, as well as the impairment of endothelial function in the previous studies were consistently associated with the elevations of cytokine level such as interleukin-6 after vaccination.38–41 In spite of this increase of PWV with inflammation, aortic AIx was reduced after the vaccine in our study.41 This seemingly paradoxical effect is mainly attributed to a profound vasodilatory effect of acute inflammation, as shown by the decrease of total peripheral arterial resistance.
Arterial effects of inflammation: potential mechanisms
The mechanisms underlying the association between inflammation and vascular dysfunction are complex and multifaceted. In brief, an inflammatory acute or chronic stimulus may trigger the synthesis of proinflammatory cytokines, such as interleukins and TNF-α, which in turn activate the endothelium to produce adhesion molecules and chemokines, and induce recruitment of white blood cells.8 In parallel with these effects, cytokine-induced endothelial activation also results in accentuation of oxidative mechanisms and a decrease of NO bioavailability, with simultaneous partial loss of the normal vasodilating, antiplatelet, and antithrombotic endothelial action. These effects further compromise the anti-inflammatory defenses, and in case of a chronic inflammatory condition, a vicious cycle starts. NO is a major marker and mediator of arterial endothelial function, and moreover, there is now ample evidence that the NO pathway plays also a crucial role in the regulation of the elastic properties of large arteries.42 However, not only NO inactivation, but also myogenic or neurogenic effects or changes of extracellular matrix23,43 may contribute to the inflammation-related impairment of large artery stiffness. Of note, existing evidence suggests a cause-and-effect link of acute inflammation with impaired arterial performance.38–41 On the other hand, no etiological relationship between the CV risk factor-related low-grade inflammatory activation and arterial dysfunction has yet been established.
The role of C-reactive protein
Among several inflammatory markers, CRP is the most thoroughly investigated compound and the one that carries the highest amount of independent prognostic information regarding future CV events. Until recently, CRP was thought as an inert bystander of vascular inflammation, which indicates but does not directly contribute to arterial dysfunction. However, given that CRP may act through several mechanisms (complement activation, stimulation of synthesis of adhesion molecules and chemoattractant chemokines, modification of ionic channels), it was hypothesized that it may have a direct proatherosclerotic effect. Concerning arterial function, it has been shown that exogeneously administered CRP may decrease NO production in vitro.44 However, these results were opposed by newer data showing that contaminating bacterial products found in the recombinant CRP preparations may actually account for the deleterious vascular effects attributed to CRP.45 On the other hand, we have observed that after the Salmonella vaccination, a large increase of CRP level coincides with the restoration rather than the deterioration of aortic stiffness (Fig. 2).41 Likewise, another study has reported explicitly similar results concerning the temporal associations of vaccine-induced endothelial dysfunction and CRP changes40 (Fig. 2). Proceeding further, this latter study showed that CRP per se may actually benefit the NO availability.40 These findings suggest that CRP does not account for the arterial dysfunction observed in acute inflammatory conditions, and indicate the complexity of this issue. Animal experiments have recently shown that CRP may directly increase the extent of necrosis in the setting of acute myocardial infarction.46 However, regarding the involvement of CRP in the chronic process of atherosclerosis (and the accompanying arterial dysfunction) in humans, existing evidence favours the notion that CRP is a marker and not a mediator. Studies using the currently available specific CRP blockers46 will demonstrate whether CRP has any definitive etiological role on arterial dysfunction and the atherosclerotic process in general.
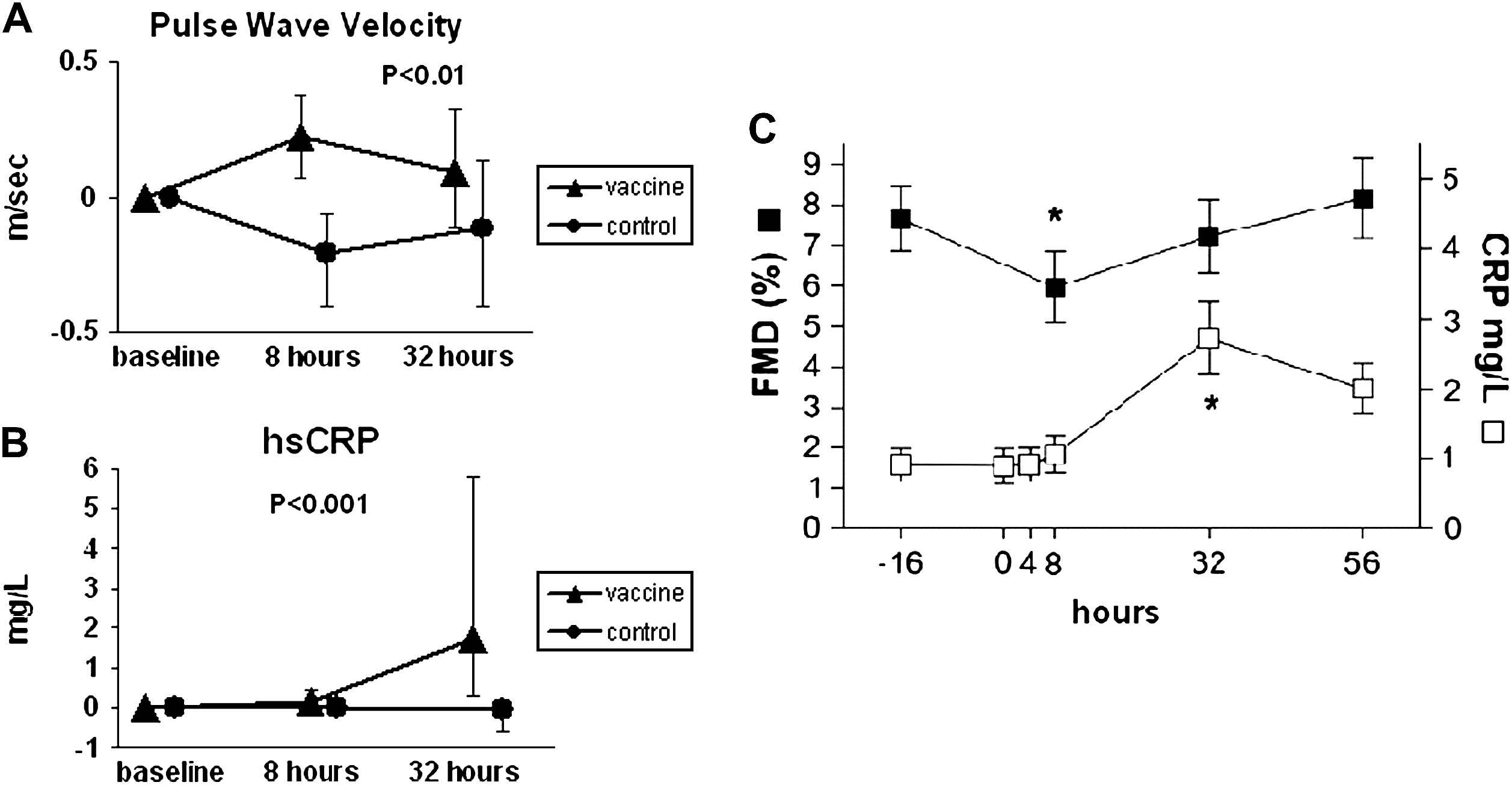
Changes (differences from baseline) in carotid–femoral pulse wave velocity and C-reactive protein (CRP) after Salmonella typhi vaccination in healthy volunteers. The large increase of CRP level (at 32 h) coincides with the restoration rather than the deterioration of aortic stiffness (change of pulse wave velocity is significant at 8 h but non-significant at 32 h) (A, B). A striking similarity is noted regarding the response of flow-mediated dilation (FMD) of the brachial artery and CRP after the vaccination (C). Reprinted with permission from Clapp et al.40 and Vlachopoulos et al.41
Effects of drugs with anti-inflammatory properties on arterial function
An increasing number of pharmaceutical treatments with potential anti-inflammatory properties have been proved beneficial in improving the inflammation-related arterial dysfunction.
A single high oral dose of aspirin, a pluripotent compound that benefits several aspects of CV pathophysiology, has been shown to abrogate the deterioration of forearm endothelial function that is induced by the Salmonella typhi vaccine.39 Similarly, we observed that aspirin pretreatment fully prevents the acute increase of aortic stiffness after the vaccine,41 although the inflammation-induced rise of CRP or IL-6 is not mitigated. Since the dose of aspirin in the above studies is much higher than the dose used for primary and secondary prevention in everyday practice, the clinical significance of this anti-inflammatory effect of aspirin is currently unknown.
The CV safety of the selective cycloxygenase-2 inhibitors has been questioned. However, an issue remains whether the increase of CV outcomes associated with chronic use of such drugs is a class effect, or whether reservations should concern only certain drugs in the class. Interestingly, some observations support the notion that this is perhaps not a class effect. In particular, in patients with chronic coronary artery disease, celecoxib may improve endothelial performance.47 Similarly, we recently observed that in healthy subjects, celecoxib blunts the increase of inflammatory markers/mediators such as IL-1β induced by acute cigarette smoking48 and furthermore it prevents the deterioration of endothelial function and arterial stiffness after smoking.49
Intermittent infusions of drugs that directly inhibit proinflammatory cytokines are currently used in the treatment of several chronic inflammatory diseases. In patients with rheumatoid arthritis, treatment with anti-TNF-α compounds lowered the activity of the disease, it improved aortic stiffness and peripheral endothelial function, but it did not alter wave reflections.50,51 In a study of patients with inflammatory vasculitis, anti-TNF-α factor infliximab was beneficial to forearm endothelial function after 3 months of treatment, and this was associated with a simultaneous decrease of inflammatory markers and clinical remission.52 However, the potential favourable CV effects of anti-TNF-α therapy have to be considered with great caution, because there are data showing that in subjects with established CV disease, this treatment may be associated with new onset heart failure.
Finally, the anti-inflammatory effects of statins (which are considered independent of lipid lowering effects) are currently under intense investigation. In patients with rheumatoid arthritis, a 3-month atorvastatin regimen was shown to decrease wave reflections, especially in subjects with high activity of the disease.53 In patients with heart failure that is accompanied by intense inflammatory activation, short-term administration of atorvastatin improved forearm vasomotion and decreased the level of cytokines.54 The anti-inflammatory efficacy of statins has also been demonstrated in acute inflammatory conditions. In healthy individuals, preliminary results from our laboratory show that a 4-day pretreatment period with atorvastatin may prevent the decline of brachial artery flow-mediated dilation that is caused by the Salmonella typhi vaccine model of acute inflammation, although this drug does not blunt the initiation of the inflammatory cascade induced by the vaccine.55
Epilogue
Almost all types of inflammation have been associated with an impairment of arterial function (arterial stiffness, wave reflections, endothelial function), which are important determinants of CV performance and predictors of the corresponding outcomes. With regard to acute inflammatory stimuli and chronic inflammatory diseases (autoimmune or infectious), it seems that there is a cause-and-effect relationship between inflammatory activation and abnormal arterial performance. In case of chronic subclinical inflammation (cardiovascular risk factors, erectile dysfunction), an association between circulating level of inflammatory markers/mediators and arterial dysfunction indices is noted. However, there are no sufficient data to support that this is an etiological relation and not an epiphenomenon. At the moment, there is no sound evidence to suggest a causal involvement of C-reactive protein in the induction of arterial dysfunction and the genesis of atherosclerosis. Several drugs with documented effectiveness, especially statins, have been proved beneficial in improving the inflammation-related vascular dysfunction. As knowledge on the molecules and the pathways that initiate the inflammatory cascade continues to evolve, it is expected that appropriately designed future studies will clarify whether inflammation per se may be regarded as a treatment target for the cardiovascular health.
References
Cite this article
TY - JOUR AU - Konstantinos A. Aznaouridis AU - Christodoulos I Stefanadis PY - 2007 DA - 2007/06/06 TI - Inflammation and arterial function☆ JO - Artery Research SP - 32 EP - 38 VL - 1 IS - 1 SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2007.03.005 DO - 10.1016/j.artres.2007.03.005 ID - Aznaouridis2007 ER -