
Study of atherosclerosis in abdominal aortic aneurysms of autopsied patients
- DOI
- 10.1016/j.artres.2018.04.003How to use a DOI?
- Keywords
- Atherosclerosis; Aorta; Autopsy; Collagen
- Abstract
Background: Any kind of change in the arterial wall as atherosclerosis, may be the etiologic agent of the formation of aneurysm in an artery. The aim of this study was to describe the morphological and morphometric characteristics of the aorta with aneurysm in autopsied patients in relation to age, gender, white and non-white patients and the aortic segment.
Methods: 22 samples of aorta were evaluated, from patients autopsied, grouped in 11 patients with aneurysm and 11 patients without aneurysm. Macroscopic evaluation of the intensity of atherosclerosis has been described quantitatively in centimeters. Staining were made by Picrosirius for quantification of collagen fibers. The analysis of captured images was performed by software Leica QWin Plus®. For statistical, the data were analyzed with the software GraphPad Prism®.
Results: There was a positive and non significant correlation between the intensity of atherosclerosis and age of the total group (rS = 0.352; p = 0.29).There was a greater intensity of atherosclerosis in relation to age in the group with aortic aneurysm (PA) (U = 26.50; p = 0.03) and higher percentage of collagen fibers (U = 31,950; p < 0.0001)when compared to the NA group. A negative correlation was observed between the percentage of collagen fibers and the intensity of atherosclerosis (rS = −0.109; p = 0.02) (PA).
Conclusions: The intensity of atherosclerosis presented a relation with age, feminine gender, white patients and abdominal aortic segment. The aging process is the cause of atherosclerosis, causing alterations in the arterial walls as an increase of the collagen fibers, thus favoring the appearance of vascular aneurysms.
- Copyright
- © 2018 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
Abdominal aortic aneurysm (AAA) is a permanent localized dilatation of abdominal aorta that exceeds normal diameter by 50% accompanied by inflammatory response in the wall of abdominal aorta.1 The risk factors include male gender, age, prior vascular disease, hypertension, cigarette smoking, family history, hypercholesterolemia.2 Atherosclerosis is the most common causative factor.3
Atherosclerosis is a chronic inflammatory disease that occurs affecting of medium and large-caliber arteries.1,4,5 Any kind of change in the arterial wall, either congenital or acquired, which causes weakening or compromises arterial wall resistance, as in atherosclerosis, may be the etiologic agent of the formation of aneurysm in an artery.6–8
Thus, this study suggests there is a relation of age with the intensity of atherosclerosis and that there is an increase in the percentage of collagen in the media and adventitia layers of the aorta with aneurysm. The aim of this study was to describe the morphological and morphometric characteristics of the aorta with aneurysm in autopsied patients in relation to age, gender, white and non-white patients and the aortic segment.
Material and methods
This study was approved by the Ethics Committee of the Federal University of Triangulo Mineiro, under number 1265.
From the files of the Discipline of General Pathology of the UFTM, 141 segments of aortas were analyzed, in the 1976–2004 period. We found 11 segments with aortic aneurysm, which constituted the group PA (Fig. 1). Selection for the PA group was performed regardless of age, gender, patients were white or non-white and or segment of the affected aorta. For paired with the PA group, another 11 segments were collected and formed the group without aneurysm (NA).
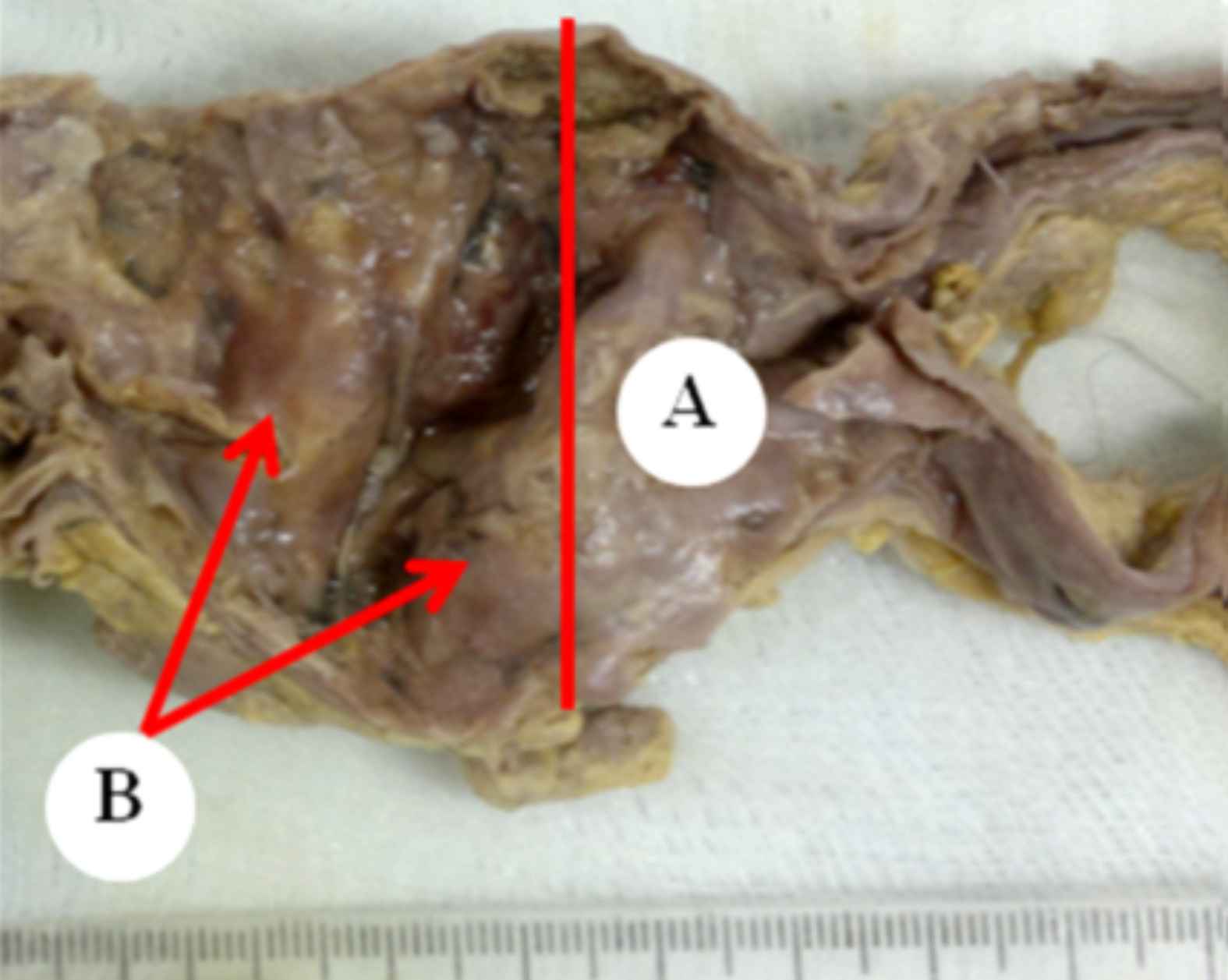
Segment Abdominal aortic aneurysm patient with autopsied at HC-UFTM in 1976–2004. (A) aneurysmal dilatation (50% or more). (B) Are observed fibroadenomatous plates with calcifications (severe atherosclerosis).
The inclusion criterion for the PA group was the macroscopic view of the aneurysm, and the segment being at least 15 cm long. For the NA group was the absence of aneurysm, a segment with at least 15 cm, and being paired with the PA group in age, white and non-white patients and gender.
For the assessment subjective of the intensity of atherosclerosis, the macroscopic view of the extension of the atheromatous plaques, lipid striae and calcification were considered.6 The intensity of the macroscopic atherosclerosis was semi-quantitatively classified into mild (predominance of lipid striae), moderate (predominance of atheromas) or severe (predominance of calcifications).
From a criterion already described in the literature9,10 the atherosclerosis was quantitatively categorized. With a non-millimetric standardized scale of 0.0 cm–12.0 cm, the examiner has subjectively determined the intensity of the degree of atherosclerosis in this scale, registering a point on it. With a millimetric ruler, the distance of 0.0 cm to the point recorded for each of the segments was measured. We observed varying degrees of atherosclerosis and accurate values for the classifications mild, moderate and severe. The intervals 0.1–4.0 cm were adopted as mild, 4.1 to 7.0 as moderate and 7.1 to 12.0 as severe degree.
From each of the aortic segments, for the PA group the selected site was the center of the aneurysm, and for the NA group, the fragment was removed from the nearest location of the lesions (striae, atheromatous plaques, calcifications). The fragments fixed in 10% formaldehyde, were histologically processed to morphometric analysis.
The slide was stained using Picrosirius11 for quantification of collagen in the media and adventitia layers of aortas, examined under polarized light, with final magnification of 1600× (Fig. 2). The analysis and morphometry were performed by the software Leica QWin Plus®.12,13 The number of fields for quantification of collagen fibers was defined by the test of cumulative means.14
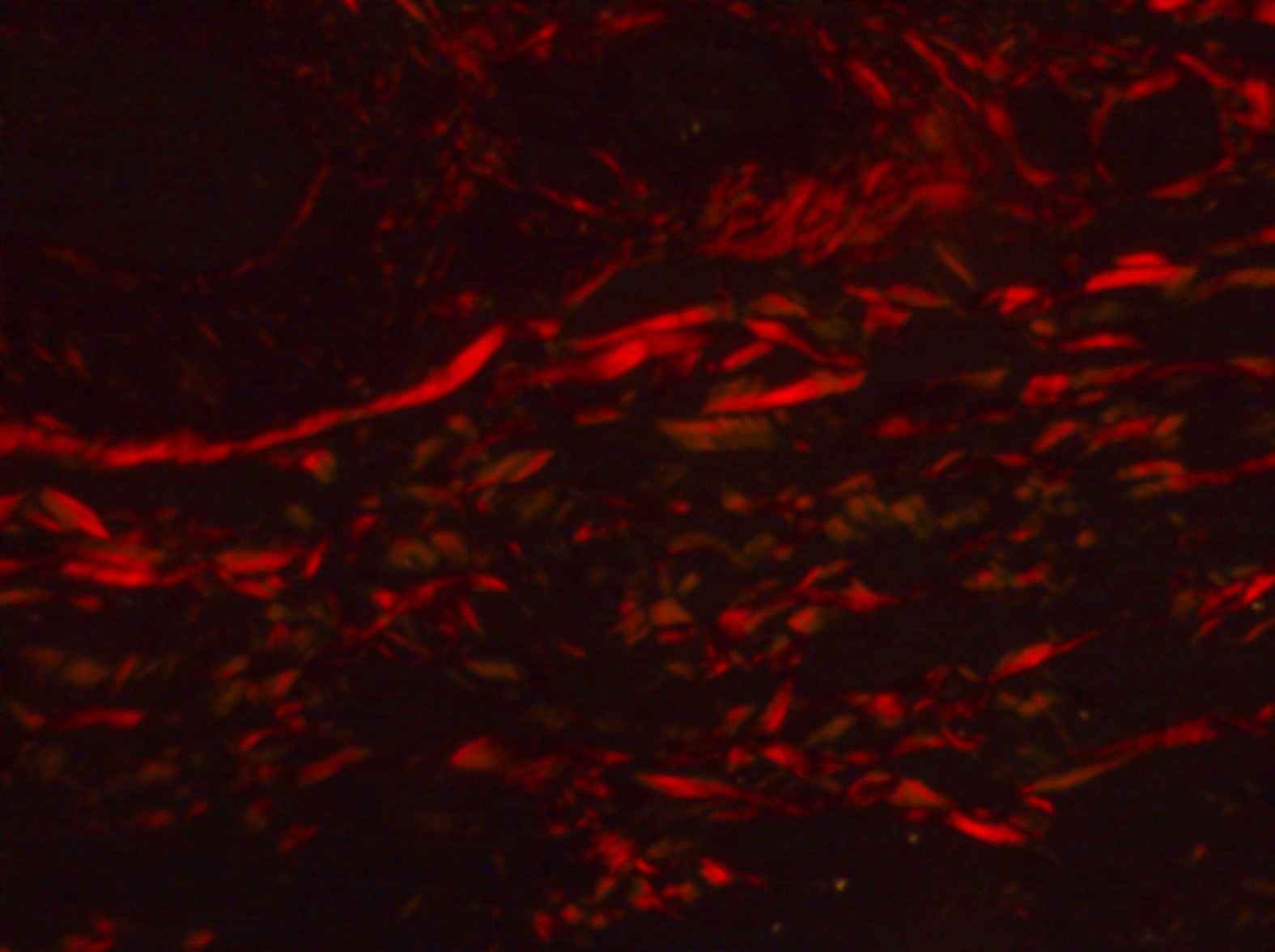
Quantification of collagen in the media and adventitia layers of aortas (PS under polarized light, 1600×).
For statistical, the data were analyzed with software GraphPad Prism® 5. Verification of distribution of quantitative variables was performed with the Kolmogorov–Smirnov test. The t-test was used to assess age between the PA and NA groups. Fisher’s exact test was used to evaluate qualitative variables such as gender, color and aortic segment in both groups.
The Mann Whitney test was used to compare the percentage of collagen fibers between the PA and NA groups. To associate the intensity of atherosclerosis with age, gender, color and aortic segment, the variables were analyzed using the unpaired “t” test or by ANOVA. Cases with non-normal distribution were analyzed by Kruskal–Wallis test (H). To correlate the percentage of collagen fibers with the intensity of atherosclerosis, we used the Spearman coefficient (rS) or the Pearson coefficient (r). The results were considered statistically significant at p < 0.05.
Results
The general characteristics of PA and NA groups are given in Table 1. There was no significant difference between age (p = 0.59), gender (p = 1.00), white and non-white patients (p = 1.00) and aortic segment (p = 0.67), thus a homogeneous distribution between the groups.
| Characteristics | PA group (n = 11) | NA group (n = 11) | Total (n = 22) |
|---|---|---|---|
| Agea (years, mean ± SD) | 70.2 ± 8.8 | 68.4 ± 6.7 | 66.5 ± 7.7 |
| Sexb (M:F) | 5:6 | 5:6 | 10:12 |
| Colorc (W:NW) | 9:2 | 9:2 | 18:4 |
| Segmentod (A:T) | 6:5 | 4:7 | 11:11 |
SD: standard deviation; M: male; F: female; W: white; NW: not-white; C: cause of cardiovascular death; NC: not cause of cardiovascular death.
Test t, t = 0.5473; p = 0.59.
Fisher’s exact test, p = 1.00.
Fisher’s exact test, p = 1.00.
Fisher’s exact test, p = 0.67.
General characteristics of patients autopsied the PA and NA groups.
There was a positive and non-significant correlation between age and intensity of atherosclerosis in PA group (rS = 0.352; p = 0.29) and in NA group (rS = 0.078; p = 0.81) (Fig. 3A and B).
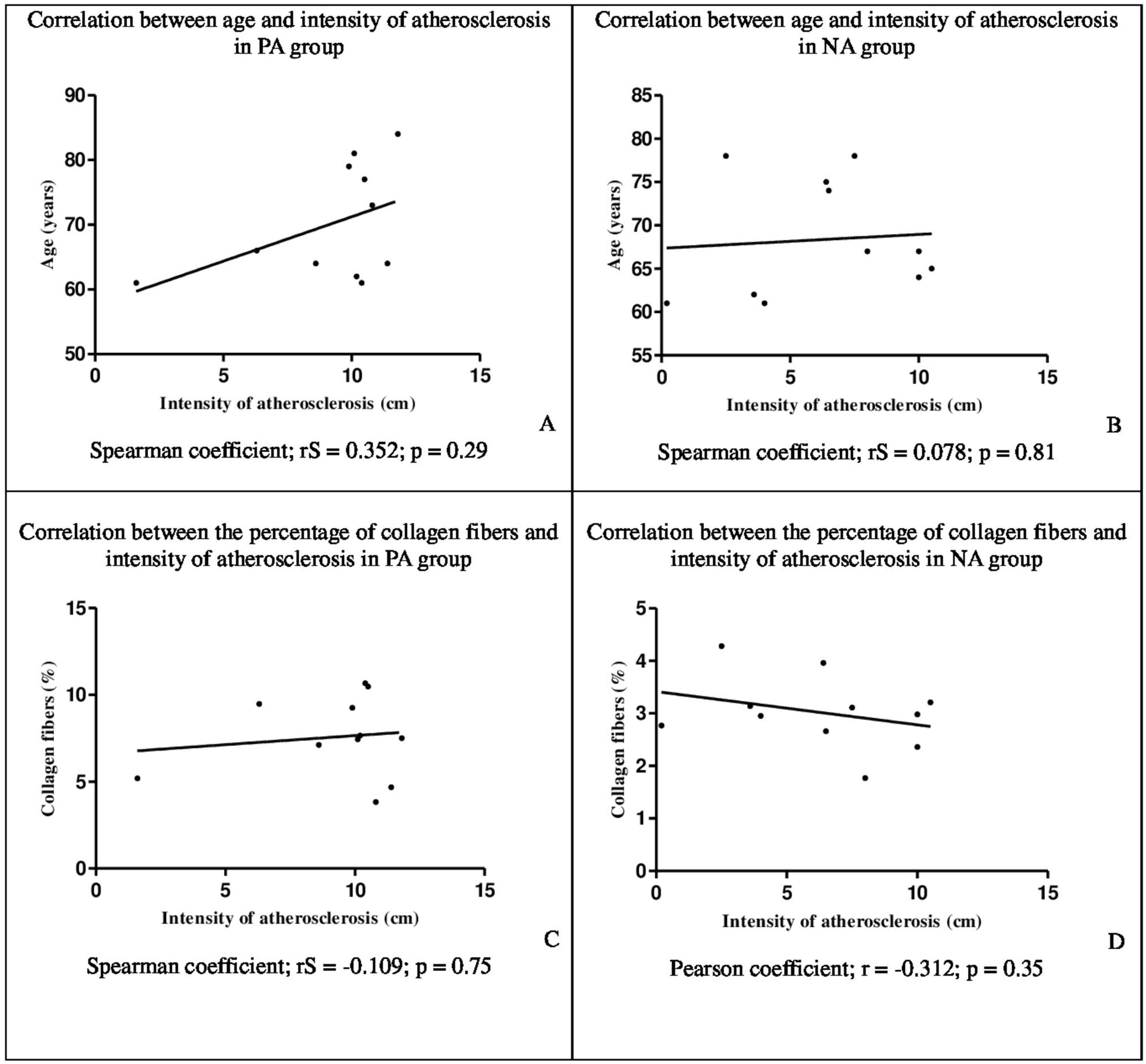
Correlation between age and intensity of atherosclerosis in PA group (A) and NA group (B). Correlation between the percentage of collagen fibers and intensity of atherosclerosis in PA group (C) and NA group (D).
Although no significant difference, feminine gender had a higher intensity of atherosclerosis when compared to male gender, both in PA (t = 1.649; p = 0.13) and NA groups (t = 0.582; p = 0.57). In the PA group, white patients had higher intensity of atherosclerosis (F = 6.812; p = 0.08) (Table 2).
| PA Group | NA Group | |||
|---|---|---|---|---|
| Intensity of atherosclerosis (cm, mean ± SD) | Malea | 7.76 ± 3.87 | Maleb | 5.62 ± 3.72 |
| Femalea | 10.47 ± 1.12 | Femaleb | 6.85 ± 3.29 | |
| Whitec | 9.42 ± 3.07 | Whitec | 5.47 ± 3.16 | |
| Not-whitec | 8.4 ± 2.97 | Not-whitec | 10 | |
| Abdominal d | 10.47 ± 0.55 | Abdominale | 7.63 ± 3.25 | |
| Thoracicd | 7.76 ± 4.02 | Thoracice | 5.53 ± 3.44 | |
| Intensity of atherosclerosis (cm, mean ± SD) | 9.24 ± 2.93f | 6.3 ± 3.37f | ||
| Percentage of collagen fibers (%, mean ± SD) | 7.57 ± 4.5g | 3.02 ± 2.22g |
Test t, t = 1.649; p = 0.13.
Test t, t = 0.582; p = 0.57.
Kruskal–Wallis test, F = 6.812; p = 0.08.
Test t, t = 1.649; p = 0.13.
Test t, t = 0.991; p = 0.35.
Mann Whitney test; U = 26.50; p = 0.03.
Mann Whitney test; U = 31,950; p < 0.0001.
Comparison of percentage of intensity of atherosclerosis and percentage of collagen fibers in individuals with aortic aneurysm (PA) (n = 11) and individuals without aortic aneurysm (NA) (n = 11).
The segments of abdominal aorta of patients in PA (t = 1.649; p = 0.13) and NA (t = 0.991; p = 0.35) groups presented greater intensity of atherosclerosis (Table 2).
The PA group presented a higher percentage of collagen fibers (U = 31,950; p < 0.0001) when compared to the NA group (Table 2).
In the PA Group, negative correlation between the percentage of collagen fibers and intensity of atherosclerosis was observed (rS = −0,109; p = 0.02) in the media and adventitia layers of the aortas (Fig. 3C). In the NA group, the correlation between the percentage of collagen fibers and intensity of atherosclerosis in the media and adventitia layers of the aortas was negative (r = −0.312; p = 0.35) (Fig. 3D).
Discussion
In this study, no significant difference was found between the mean age between the PA and NA groups. However the literature highlights a tendency of individuals to present a greater intensity of atherosclerosis at older age.15 Although we did not find significant difference, we found a positive correlation between age and intensity of atherosclerosis, both in the PA group and in the NA group, indicating that age may be a determining factor for the intensity of atherosclerosis. The aging is a determining factor for morphological and functional changes in arterial walls facilitating atherogenesis.14,15
It is demonstrated in the literature a higher incidence of cardiovascular disease in male gender, including atherosclerosis.15 Another study found that moderate or severe aortic atherosclerosis is most commonly observed in male elderly.16 Although we did not measure estrogen levels, one study observed that as the menopause occurs usually around 50 years old, the result above was probably due to a natural decline in estrogen levels, resulting in a greater exposure to atherosclerosis risk factors. This hormone presents an anti-inflammatory effect, which stabilizes the atheromatous plaque until the premenopausal period.17 As in another study in which they found a very rare case of distal aneurysm of anterior cerebral artery segments associated with multiple intracranial saccular aneurysms with an abdominal aortic aneurysm in cadavers of elderly women.18 In this study, despite a non-significant difference between feminine gender and male gender, both in the PA group and in the NA group, we believe that there is a tendency for women to suffer more in this age group. The lack of consensus in the results found shows that the gender component may have no influence on the relationship with the intensity of atherosclerosis.
The results of this study demonstrate that in the PA group there is a tendency of predominance of atherosclerosis intensity in white patients in comparison to non-whites, although studies show that there is a greater incidence in black people.17,19 This is because the miscegenation of Brazilian population makes it difficult to characterize which ethnicity would be more susceptible to atherosclerotic disease. Possibly the socioeconomic status of most patients seen in public attendance could contribute to the increased exposure to risk factors for atherosclerosis, regardless of ethnicity. The Pan American Health Organization points out that socioeconomically disadvantaged population are more exposed to cardiovascular risk factors.20
With aging of the population there is a higher incidence of aortic aneurysms, especially abdominal.21–24 The abdominal aortic aneurysm is usually a sequel of atherosclerosis, both diseases considered more advanced in the elderly.25 In this study macroscopically, a marked involvement of atherosclerosis plaques was observed throughout the abdominal aortic aneurysm, which corroborates with another study that observed throughout the aortas with abdominal aneurysm the involvement of atherosclerosis in 75% of the cases.26 Despite these reports in the literature, we believe that there is a tendency of the abdominal segment to be more affected by a higher intensity of atherosclerosis in the PA group and in the NA group.
Atherosclerosis is described as an important risk factor in the etiology of the aneurysm, although disturbances of connective tissue metabolism may be involved.27,28 In fact, atherosclerosis and AAA share a number of risk factors, such as age, smoking, systemic arterial hypertension and hypercholesterolemia.29 In our study we + found a higher intensity of atherosclerosis in the PA group when compared to the NA group. Despite these findings, currently in the literature it has been described that atherosclerosis would not be a risk factor for the occurrence of aneurysm, but rather that both diseases develop independently, but share risk factors in common.1
Among the alterations in the arterial wall, as age increases, there is an increase in collagen deposition.30,31 These changes cause adaptive thickening, increasing the likelihood of aneurysms.32,33 It was found in this study higher percentage of collagen fibers in the PA group. Our findings are corroborated in the literature,34 which observed increased collagen in the abdominal aortic aneurysm when comparing the normal abdominal aorta with atherosclerotic abdominal aorta with aneurysm. Growth factors, cytokines and other substances produced during atherosclerosis contribute to the regulation of inflammatory response and cell proliferation. The result is the stability of an atherosclerotic plaque against a fibroproliferative response. The stability of the plaque depends on the thickness and composition of the fibrous layer, composed of collagen, elastin and proteoglycan proteins belonging to the extracellular matrix and synthesized by smooth muscle cells.35,36
Although atherosclerosis may not be the only factor in the development of aneurysms, it is reported in the literature that plaque formation in the aorta is associated with aortic enlargement and decreased thickness of the medial and adventitial layers.37 As in the same study that affirms the hypothesis that degeneration of the atherosclerotic arterial wall occurs as an important etiologic factor in the formation of aneurysms, particularly in the abdominal aorta.37 In our findings, the non-significant negative correlation between the intensity of atherosclerosis and the percentage of collagen fibers in the middle and adventitial layers of the PA group aortas was explained. However, another study38 described a decrease in collagen content in the abdominal aortic aneurysms corroborating our study.
A rupture of the aortic wall caused by aneurysms can be drastically fatal. Aneurysms are silent until the interval. The death of a patient with an aneurysm, if not properly diagnosed, may be erroneously associated with another cause, unless an autopsy is performed.39
Conclusion
The macroscopic method employed in this study is presented with higher sensitivity than semiquantitative analysis to determine the intensity of atherosclerosis in aorta segments. There were varying degrees for mild, moderate and severe ratings. Through the evaluation, it was concluded that seems to be a relation of the intensity of atherosclerosis with age, female gender, white patients, abdominal aortic segment.
Finally, the aging process was the primary cause of atherosclerosis, causing morphological changes in arterial walls, favoring the appearance of vascular aneurysms. The anatomopathological study in autopsies shows the importance of the evaluation of abdominal aortas in relation to atherosclerosis, contributing to the prevention and treatment of other patients at the clinic.
Conflict of interest statement
The authors declare no conflicts of interest.
Acknowledgements
This study was conducted with grants from
References
Cite this article
TY - JOUR AU - Maria Helena Soares AU - Mariana Silva Oliveira AU - Aline Cristina Souza da Silva AU - Bianca Gonçalves Silva Torquato AU - Gabriela Ribeiro Juliano AU - Guilherme Ribeiro Juliano AU - Márcia Fernandes de Araújo AU - Camila Lourencini Cavellani AU - Lívia Ferreira Oliveira AU - Mara Lúcia Fonseca Ferraz AU - Vicente de Paula Antunes Teixeira PY - 2018 DA - 2018/05/05 TI - Study of atherosclerosis in abdominal aortic aneurysms of autopsied patients JO - Artery Research SP - 43 EP - 48 VL - 22 IS - C SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2018.04.003 DO - 10.1016/j.artres.2018.04.003 ID - Soares2018 ER -