
Gender and Spatial Disparities of Suicide Mortality Risk in Kermanshah Province, Iran: A Brief Report
- DOI
- 10.2991/dsahmj.k.190827.001How to use a DOI?
- Keywords
- Suicide; mortality; ecological study; Iran
- Copyright
- © 2019 Dr. Sulaiman Al Habib Medical Group. Publishing services by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
In Iran, the estimated rate of complete suicide (2006–10) was about five per 100,000 population [1]. Several sociodemographic and economic factors (such as average household expenditure, unemployment rate, and divorce rate) were positively associated with suicide mortality [2]. In addition, marital problems and family conflicts are the two well-known familial risk factors for suicide [3]. Iran’s western provinces have a higher suicide rate compared to the other provinces in the country [1,4]. In addition, Kermanshah province has a noticeably higher suicide rate compared to the national average [1,5]. A previous study conducted in Kermanshah has also reported multiple individual level factors associated with the risk of attempted or completed suicide [6]. Determining the temporal and seasonal patterns of disease helps identify different spatial patterns over time and improve our understanding of the risk factors affecting the distribution of disease and death across the population and set them in the form of geographical maps [5,7]. Meanwhile, a previous ecological study has been conducted to visualize spatial heterogeneity in suicide mortality risk across the counties of the province [8]. Therefore, to improve preventive measures, a better understanding of the distribution of suicide at the national and subnational levels is important. So, the aim of this study is to update spatial variations in the risk of complete suicide across the counties of Kermanshah province, the most populated western province of Iran.
2. MATERIALS AND METHODS
2.1. Study Population
Kermanshah province is among the provinces with low socioeconomic status. Based on the 2016 Census of Population and Housing, the province’s population was 1,952,434 (about 2.5% of the total Iranian population) with an estimated unemployment rate of 22% in 2016. This province is composed of 14 counties (Kermanshah, Qasr-e Shirin, Islamabad-e Gharb, Sahneh, Sonqor, Sarpol-e Zahab, SalasBabajani, Ravansar, Dallahoo, Gilan-e Gharb, Javanrud, Kangavar, Harsin, and Paveh) and has a total land area of about 25,009 km2 [9]. The capital of Kermanshah province is the city of Kermanshah.
2.2. Data Collection and Data Analysis
In this study, county-level counts of suicide deaths in Kermanshah province were obtained from the dataset provided by the provincial Forensic Medicine Organization (FMO). Death certificates issued by the FMO have been accepted as a valid mortality data source for epidemiologic studies of suicide [4–7,10]. The corresponding populations of counties are obtained from the 2016 national census of population and housing [11]. We applied an appropriate Bayesian spatial approach—Besag, York and Mollie (BYM) model—to model the status of complete suicide in the Kermanshah province over a 1-year period, from March 21, 2016 to March 20, 2017. The BYM model, the most commonly used Bayesian model in spatial disease mapping, can be used for computing relative risk, with and without adjusting for independent variables (risk factors). This Bayesian model takes spatial proximity into account in the calculation of spatial risk which is widely used in epidemiology. The BYM model is one of the best choices in ecological analysis compared to other Bayesian ecological models for mapping spatial risk. Moreover, the BYM model outputs provide a map of population-adjusted relative risk [12]. This Bayesian spatial approach was fitted to make inference about the relative risk of complete suicide across the counties of the province. The model details and its application to suicide mapping have been described elsewhere [5,13]. All analyses were performed at the 0.05 significance levels using R package.
2.3. Ethical and Legal Considerations
Private information of deceased individuals who committed suicide was not used in the study; thus, informed consent was not required as the data are published in the public domain. The research protocol was reviewed and approved by the Ethics Committee of Kermanshah University of Medical Sciences in Iran (no. IR.KUMS.REC.1396.337).
3. RESULTS AND DISCUSSION
A total of 262 complete suicide cases were registered, with age ranging from 10 to 89 years, during the selected period. As shown in Table 1, the observed and estimated expected number of the complete suicide cases in each county of Kermanshah province for males, females, and all persons were calculated. Based on this calculation, Figure 1 shows the map of posterior mean of the county-specific relative risk. Demonstration of spatial (geographical) distributions enables the visual display of disparities within designated geographical areas. It can be seen that for all individuals, Dallahoo, Gilan-e Gharb, and Qasr-e Shirin are counties with high relative risk; also Paveh, Javanrud, and Ravansar fall into the low relative risk category. For females, Paveh, Sahneh, Sonqor, and Kangavar fall into the low relative risk category; moreover, Gilan-e Gharb is a county with high relative risk. For males, Paveh and Javanrud fall into the low relative risk category. This map reveals gender and spatial disparities in the suicide mortality relative risk in the county level, although it was not statistically significant. This finding is in line with past findings from studies that were conducted from 2006 to 2011 [5]. Findings from this study can be used to aid priority setting for suicide prevention interventions. In terms of the Human Development Index (HDI) [13], Iran ranks 60th among 189 countries in 2018. In Iran, the HDI was 0.834 for men and 0.726 for women [14]. This difference can be effective in justifying gender inequality in the distribution of suicide-related mortalities.
| County | All | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Yi | ni | Êi | Yi | ni | Êi | Yi | ni | Êi | |
| Kermanshah | 151 | 925,962 | 146.32 | 102 | 465,624 | 94.28 | 49 | 460,338 | 51.99 |
| Islamabad-e Gharb | 22 | 120,094 | 18.98 | 16 | 60,702 | 12.29 | 6 | 59,392 | 6.71 |
| Dallahoo | 13 | 30,803 | 4.87 | 8 | 15,208 | 3.08 | 5 | 15,595 | 1.76 |
| Gilan-e Gharb | 13 | 49,561 | 7.83 | 3 | 25,024 | 5.07 | 10 | 24,537 | 2.77 |
| Kangavar | 11 | 64,613 | 10.22 | 8 | 32,363 | 6.55 | 3 | 32,250 | 3.64 |
| Sonqor | 11 | 69,876 | 11.04 | 8 | 34,998 | 7.09 | 3 | 34,878 | 3.94 |
| Harsin | 9 | 65,261 | 10.31 | 4 | 32,791 | 6.64 | 5 | 32,470 | 3.67 |
| Sarpol-e Zahab | 9 | 71,316 | 11.27 | 4 | 35,599 | 7.21 | 5 | 35,717 | 4.03 |
| Qasr-e Shirin | 6 | 20,020 | 3.16 | 5 | 10,660 | 2.16 | 1 | 9360 | 1.06 |
| Salas-Babajani | 5 | 28,504 | 4.50 | 2 | 14,550 | 2.95 | 3 | 13,954 | 1.58 |
| Javanrud | 5 | 61,385 | 9.70 | 2 | 31,193 | 6.32 | 3 | 30,192 | 3.41 |
| Ravansar | 3 | 39,571 | 6.25 | 3 | 20,225 | 4.10 | 0 | 19,346 | 2.18 |
| Sahneh | 3 | 60,580 | 9.57 | 3 | 30,281 | 6.13 | 0 | 30,299 | 3.42 |
| Paveh | 1 | 50,464 | 7.97 | 1 | 25,408 | 5.14 | 0 | 25,056 | 2.83 |
| Total | 262 | 1,658,010 | 261.99 | 169 | 834,626 | 169.01 | 93 | 823,384 | 92.99 |
The observed (Yi) and estimated expected (Êi) number of cases of complete suicide in each county of Kermanshah province, from March 2016 to March 2017, for males, females, and both sexes combined. The corresponding populations (ni) of counties are obtained from the 2016 national census of population and housing
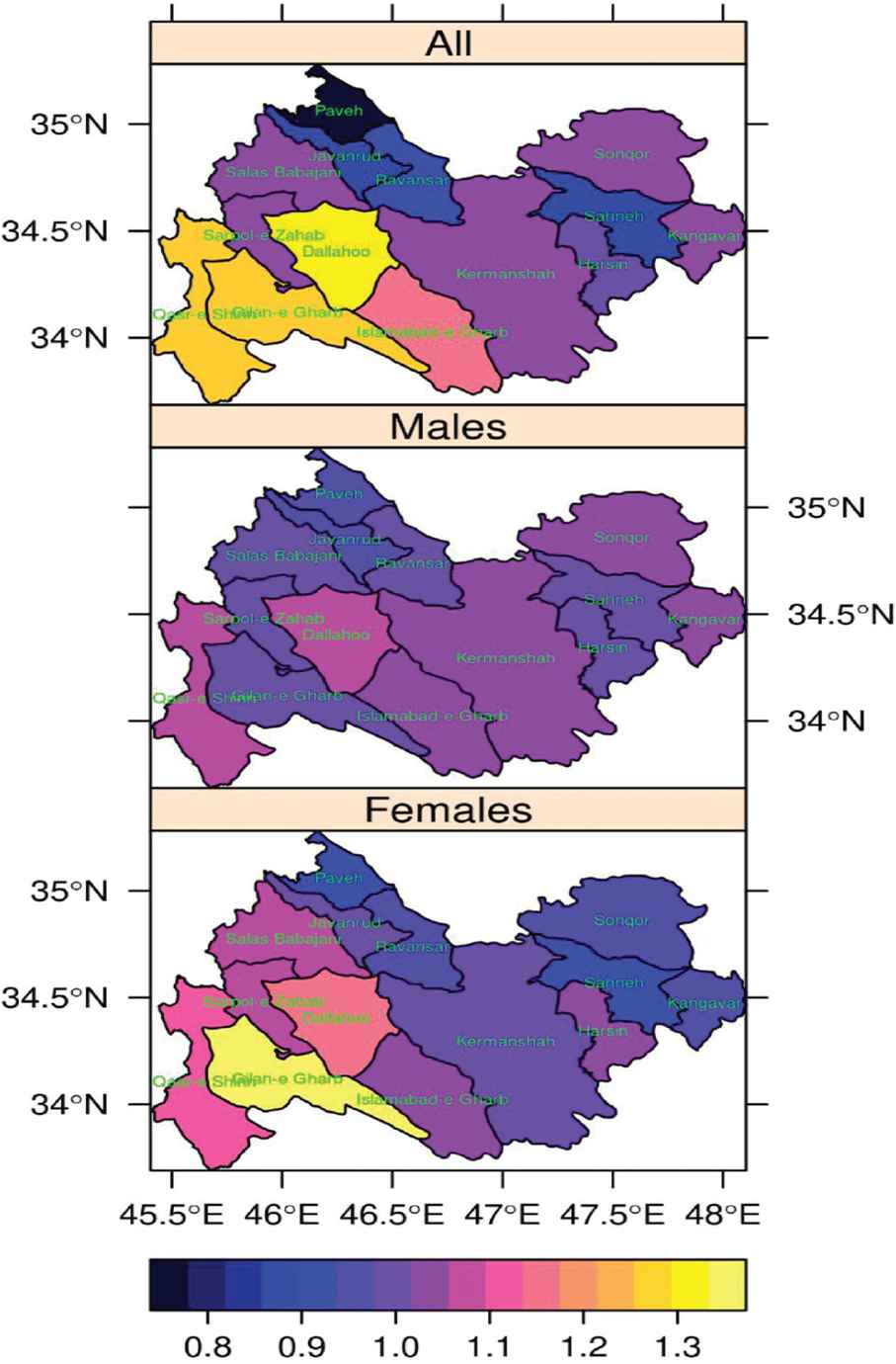
Posterior mean of the county-specific relative risk of complete suicide in the counties of Kermanshah province, compared to the risk level for the whole province, from March 2016 to March 2017.
Owing to the unavailability of data, we included 1 year of data in our analysis. Therefore, we ended up with a small sample size, which might have influenced the statistical significance of results. Some major influential factors such as mental health problems (major depressive disorders, mood and anxiety disorders, substance use disorders), and socioeconomic characteristics were not included in this study, because the related dataset has not been provided by the FMO. These factors were basic requirement data for designing suicide prevention interventions. Previous studies show that majority of suicide victims have committed suicide using violent methods in this province [5,6,10]. In conclusion, this short report presents an evidence of gender and spatial (geographical) heterogeneity in suicide mortality risk in the county level in a high incidence province of Iran. It is beyond the scope of this report to discuss the possible causes of this heterogeneity; thus, further research is warranted to gain a better understanding as well as to illustrate the factors associated with gender and spatial disparities of suicide mortality risk over a longer period.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
MR, AJ and SR participated in literature review, data analysis, and wrote the manuscript. AK were involved in data collection, and data entry. All of the authors performed step-by-step follow-up and reviewed and revised the whole paper.
ACKNOWLEDGMENTS
This study was financial supported by the Research Council of Kermanshah University of Medical Sciences (Grant Number: 96332).
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Mehran Rostami AU - Abdollah Jalilian AU - Shahab Rezaeian AU - Artin Kamali PY - 2019 DA - 2019/09/08 TI - Gender and Spatial Disparities of Suicide Mortality Risk in Kermanshah Province, Iran: A Brief Report JO - Dr. Sulaiman Al Habib Medical Journal SP - 55 EP - 57 VL - 1 IS - 3-4 SN - 2590-3349 UR - https://doi.org/10.2991/dsahmj.k.190827.001 DO - 10.2991/dsahmj.k.190827.001 ID - Rostami2019 ER -