
P20 AUGMENTATION INDEX ASSOCIATES WITH IMPAIRED EARLY VENTRICULAR EJECTION
- DOI
- 10.1016/j.artres.2017.10.161How to use a DOI?
- Abstract
Background: Previously regarded as a measure of pressure wave reflection, central augmentation index (cAI) may be influenced by the pattern of early ventricular ejection. We examined the relationship of cAI to first-phase ejection-fraction (EF1), a measure of ventricular ejection up to the time of the first systolic peak in central pressure in patients with a wide range of cardiac and arterial phenotypes.
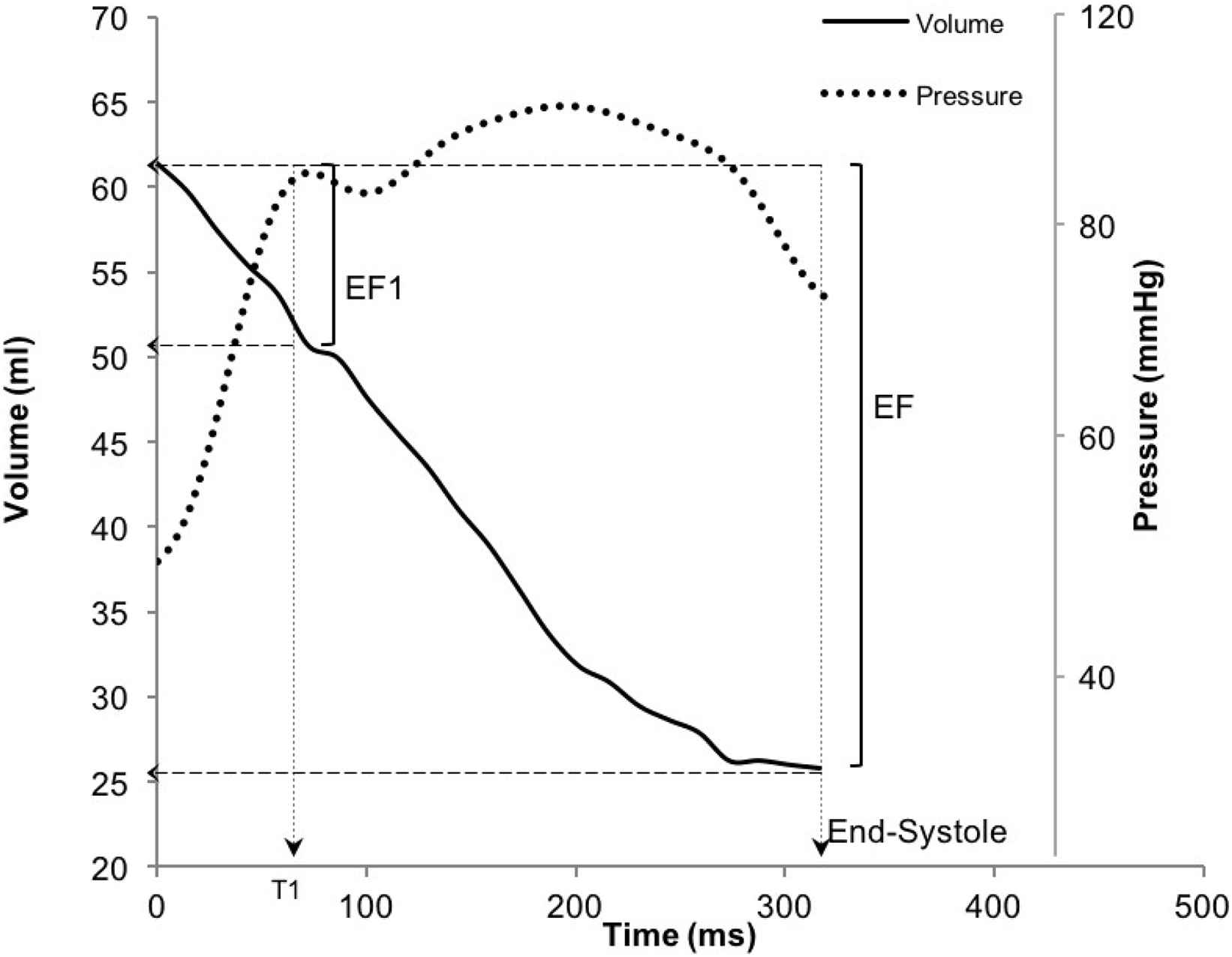
Methods: Carotid pressure, obtained by tonometry calibrated from peripheral mean and diastolic blood pressure, was used to calculate augmentation pressure (difference between the second and first systolic peaks of the aortic waveform) and index. Time- resolved LV volumes were obtained by 2D echocardiography. EF1 was defined as the fraction of LV volume ejected from the start of systole to the time of the first systolic peak (T1) on the carotid pressure waveform (Figure1). Aortic arch to abdominal aorta pulse wave velocity (aPWV) was measured by pulsed wave Doppler.
Results: We studied 127 subjects, including healthy subjects (n = 44, aged 51.5±13.6years) and patients with hypertension (n = 52, 53.6±12.9), severe aortic stenosis (AS, n = 10, 73.5±9.6) and Hypertrophic Obstructive Cardiomyopathy (HOCM, n = 21, 54.2±12.7). Ejection-fraction (58.7±5.3%) was preserved in all subjects. There was a graded inverse relationship between EF1 and cAI across different disease groups (healthy: EF1 = 21.0±1.3%, cAI = 22.6±2.5%; hypertension: EF1 = 17.4±1.0%, cAI = 31.7±1.5%; AS: EF1 = 15.9±2.7%, cAI = 36.0±3.8%; HOCM: EF1 = 23.7±1.3, cAI = −1.4±4.2%). In a multiple linear regression model, cAI was negatively associated with EF1 independent of age, gender, mean arterial pressure, aPWV and disease group (standardized regression coefficient β = −0.422, p = 0.003).
Conclusion: In patients with preserved EF, an impairment of early ejection is associated with greater augmentation pressure.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Cite this article
TY - JOUR AU - Haotian Gu AU - Gerry Carr-White AU - John Chambers AU - Phil Chowienczyk PY - 2017 DA - 2017/12/06 TI - P20 AUGMENTATION INDEX ASSOCIATES WITH IMPAIRED EARLY VENTRICULAR EJECTION JO - Artery Research SP - 98 EP - 99 VL - 20 IS - C SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2017.10.161 DO - 10.1016/j.artres.2017.10.161 ID - Gu2017 ER -