
Arterial stiffness and diastolic blood pressure: what is the connection?
- DOI
- 10.1016/S1872-9312(07)70001-7How to use a DOI?
- Keywords
- hypertension; diastolic blood pressure; arterial stiffness; hemodynamics; epidemiology
- Abstract
Although brachial systolic blood pressure (SBP) is the overall best predictor of future cardiovascular risk for the entire hypertensive population, there is much that can be learned from assessing diastolic blood pressure (DBP) in relation to simultaneous levels of SBP, because the former is not distorted by pressure amplification. In very young (mean age of 20 years) hypertensives, discordantly low DBP, defined as isolated systolic hypertension (ISH), was associated with increased stroke volumes (SV), increased aortic stiffness or a combination of both. These individuals had a significantly higher mean central SBP than normotensive persons, and therefore, should not be classified as having spurious hypertension. In contrast, young adults with essential hypertension presented with elevated DBP and evidence of increased peripheral vascular resistance. Discordantly high DBP in young adults (mean age of 40 years) with isolated diastolic hypertension (IDH) was associated with a high prevalence of obesity and the metabolic syndrome; DBP was discordantly high because of a limited rise in SBP secondary to decreased pressure amplification. Discordantly very low DBP in the older age population (mean age ⩾60 years) with ISH defines a population with LVH, increased ventricular-arterial stiffness, and a propensity for diastolic dysfunction. Therefore, discordantly low DBP may be an early marker of increased SV and/or arterial stiffness in young adults and a late marker of ventricular-arterial stiffness in older adults. In contrast to risk prediction where brachial DBP may be of paramount importance, the therapeutic benefit of antihypertensive therapy is entirely related to decreased SBP.
- Copyright
- © 2006 Published by Elsevier. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
1. Introduction
With the recent emphasis on systolic blood pressure (SBP) as the best all around predictor of cardiovascular risk, it has become fashionable to downgrade the prognostic value of diastolic blood pressure (DBP) [1,2]. Furthermore, aortic stiffness – as measured by pulse wave velocity (PWV), central augmentation index (AIx) and central pulse pressure (PP) – has been shown to be sensitive independent predictor of cardiovascular risk [3,4]. On the other hand, brachial DBP, under certain circumstances, may be superior to brachial SBP as a predictor of arterial stiffness and cardiovascular risk.
There are certain caveats that must be considered in assessing blood pressure (BP) measurements. Measurement error is usually larger for DBP than for SBP because of the greater variability in the auscultatory end point [5]. In addition, there is a potential discrepancy between cuff and intraarterial BP measurements. With the most careful cuff measurements, true SBP may be underestimated by 0–5mmHg and true DBP overread by 5–15mmHg or more compared to simultaneous intraarterial pressure recordings [6]. The larger discrepancy in DBP, however, is more likely to be present in elderly hypertensives with large artery stiffness [6]. Therefore, diastolic pseudohypertension, if present, would lead to an underestimation of PP and of large artery stiffness. Finally, the term, discordant DBP, as used in this review, refers to the relative change in DBP as compared to change in SBP. Discordantly low brachial DBP (wide PP hypertension) is arbitrarily defined as the isolated systolic hypertension (ISH) subtype (DBP < 90 and SBP⩾140 mmHg). Similarly, discordantly high brachial DBP (narrow PP hypertension) is arbitrarily defined as the isolated diastolic hypertension (IDH) subtype (DBP⩾90 and SBP < 140 mmHg).
The value of brachial DBP in predicting cardiovascular risk requires an understanding of arterial pressure amplification. Although mean arterial pressure (MAP) and DBP are relatively constant throughout the arterial tree, SBP increases progressively with movement away from the aortic valve [7]. As a consequence, brachial artery PP is 5–20mmHg higher than that recorded in the ascending aorta. Arterial pressure amplification arises because of (1) increasing arterial stiffness as one moves from the elastic thoracic aorta to more distal muscular arteries; (2) progressive decrease in diameter of more distal arteries; and (3) the influence of wave reflection within the arterial tree. Furthermore, brachial artery PP may not always be a reliable surrogate for central artery PP because pressure amplification is not fixed but varies according to a number of demographic factors (height, gender, exercise, age, and heart rate) and cardiovascular risks (dyslipidemia, hyperglycemia, smoking, and impaired renal function) [7]. Thus, variations in pressure amplification may have important clinical implications, largely because the heart, brain, and kidneys “see” aortic rather than brachial pressure. In summary, brachial DBP, in relation to brachial SBP, may be a useful marker of central BP because it is not distorted by pressure amplification.
2. Discordantly low DBP in very young adults with ISH
Although ISH is usually associated with the elderly, there is now firm evidence that ISH is also the majority hypertensive subtype in adolescents and young adults. Sorof et al. [8] found that ISH was 2.8 times as common as diastolic hypertension in adolescent boys and girls and was associated with increased body mass index (BMI) and echocardiographic LVH; hemodynamic studies were not done. McEniery et al. [9] studied young adult university students with a mean age of 20 years in the ENIGMA study and confirmed that ISH, also associated with increased BMI, outnumbered those with essential hypertension (elevated SBP and DBP, or DBP alone) by a ratio of ∼2:1. This study measured peripheral and central BP, aortic PWV, cardiac output (CO), stroke volume (SV) and calculated peripheral vascular resistance (PVR) in 1008 subjects. The major new findings of this study were that ISH and essential hypertension had different hemodynamic mechanisms. Essential hypertension was associated with elevated PVR, reduced SV, normal isobaric PWV and almost an equal gender distribution. In contrast, ISH in young adults had ∼90% male predominance and a heterogeneous hemodynamic pattern distinctly different from essential hypertension. A scatterplot (Figure 1) showed that 28% of subjects with ISH had increased SV and normal isobaric aortic PWV; 20% had an increased isobaric aortic PWV indicative of increased aortic stiffness and normal SV; and 41% had elevated SV and increased aortic PWV, suggestive of a mixed hemodynamic state; all 3 ISH groups had heart rates indistinguishable from normotensive control subjects, but significantly lower than those with essential hypertension.
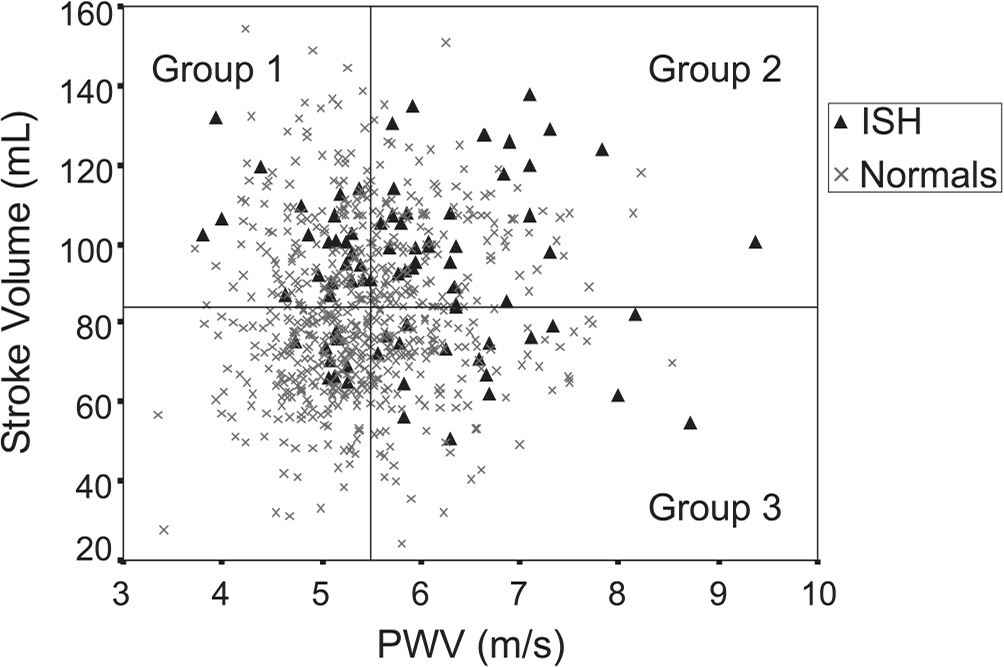
Scatterplot of SV versus PWV in normotensive (-x-) and ISH (-%-) subjects. The crossbars represent the normotensive means for SV (horizontal) and PWV (vertical). A indicates upper SV, lower PWV; B, upper SV, upper PWV; C, lower SV, Upper PWV; and D, lower SV, lower PWV. Percentages within the graph represent the proportion of subjects within each quadrant. Reproduced with permission from McEniery CM, et al. Hypertension 2005;46:221–226.
The cross-section nature of the first phase of the ENIGMA study does not shed light on the underlying causative mechanism or long-term prognosis of young adult subjects with ISH. Two previous studies have suggested that ISH in young males may result from exaggerated pressure amplification of a normal central PP, and hence, represents spurious or pseudohypertension [10,11]. In the ENIGMA study, however, there was no difference in PP amplification between normotensive subjects and those with ISH. Furthermore, central SBP was ∼22mmHg higher in ISH than in normotensives; therefore, ISH in young adults might not be a benign condition. Undoubtedly, some of the ISH subjects with elevated CO/SV may well progress to develop essential hypertension with elevated PVR and reduced SV, as has been reported in earlier studies [12,13]. The mechanisms underlying the increased SV in subjects with ISH are unclear. However, the ∼20% of subjects with ISH in the ENIGMA study with increased isobaric aortic PWV and normal SV may have premature aortic stiffening. Interestingly, the Framingham Heart Study [14] showed that about 60% of new-onset ISH never went through a phase of essential hypertension. It is possible that some of these young adults in the ENIGMA study with evidence of early arterial stiffness, discordantly low DBP and ISH may keep this pattern throughout middle-age and beyond. Future longitudinal studies will be necessary to distinguish between parallel and sequential causative pathways in the development, evolution and ultimate prognosis of ISH in very young adults.
3. Discordantly high DBP in young adults with IDH
The Framingham Heart Study examined the relationship between BP and coronary heart disease (CHD) risk as a function of age [15]. From the age of 20 to 79 years there was a continuous, graded shift from DBP to SBP and eventually to PP as predictors of CHD risk. In the age group <50 years of age, DBP was a more powerful predictor of CHD risk than SBP and PP was not predictive. Confirmatory evidence favoring DBP over SBP in predicting CHD risk in young adults was noted in a study utilizing intra-arterial BP measurements [16] and in the recent German PROCAM study [17].
None of these studies, however, made a distinction between the two subtypes of diastolic hypertension: systolic–diastolic hypertension (SDH, SBP ⩾140 and DBP ⩾90 mmHg) and IDH. The National Health and Nutrition Examination Survey (NHANES III, 1988–91) [18] showed that IDH was the most frequent form of diastolic hypertension in young adults < age 40 and of comparable frequency as SDH from age 40 to 49. Together, IDH and SDH accounted for >75% of younger adult individuals with untreated hypertension. Surprisingly, despite its frequency in young hypertensives, IDH has been considered to be an artifact of measurement [19] or a benign condition of no clinical importance in the New York Work-Site Hypertension Control Program [20], the Honolulu Heart Program [21], the Copenhagen City Heart Study [22], and the Finish Male Cohort Study [23].
A subsequent Framingham Heart Study showed that new-onset IDH developed primarily from normal and highnormal BP during a 10-year follow-up [14]. Furthermore, 82.5% of participants with baseline IDH developed SDH during the ensuing 10 years of follow-up, suggesting that IDH was a frequent precursor for the development of SDH, and therefore, potentially not a benign condition. In addition to BP, predictors of IDH were increased body mass index at baseline, weight gain over time, and being a young adult male. Not surprisingly, because this study examined subjects in the 1950s and 1960s and did not record waist circumference or measure HDL-cholesterol and serum triglycerides, the contemporary components of the metabolic syndrome could not be studied.
A recent NHANES, 1999–2002 study [24] addressed the presence of the metabolic syndrome in untreated subjects with IDH. The major new findings of this study were that women and to a lesser extent men with IDH had the highest odds ratio (OR) for having the metabolic syndrome as compared to those individuals with SDH or ISH, despite persons with IDH being considerably younger (mean age of 40 years) than individuals in the other 2 hypertension subtypes. Previous investigations have shown that the prevalence of the metabolic syndrome increases with aging. The present study suggests that the abdominal obesity factor (and possibly other metabolic risk factors) have a closer association with the IDH subtype than age. Indeed, since young women, as compared to young men, had a lower prevalence of IDH (∼1:4), severe obesity in young women may be a critical factor in their development of IDH [24]. Furthermore, Safar et al. [25] showed that the presence of the metabolic syndrome, independent of MAP, SBP and DBP, accelerated PWV (and hence arterial stiffening) in a 6-year longitudinal French population, thus, strongly suggesting premature vascular senescence. Future long-term outcome studies, however, will be necessary to determine the overall incidence of new-onset diabetes and of cardiovascular events that occur in persons with the metabolic syndrome and IDH. Undoubtedly, the current epidemic of obesity in adolescents and young adults has contributed substantially to the increased prevalence of this entity. In summary, the preponderance of evidence suggests that IDH, far from being benign, is a legitimate form of essential hypertension in young adults that is strongly associated with the metabolic syndrome.
What explains the difference between IDH and more conventional subtype of systolic–diastolic essential hypertension? The frequent progression from prehypertension to IDH in young adults is consistent with underlying increased peripheral resistance [14]. Brachial DBP and SBP rise with increases in peripheral resistance, but the rise in peripheral SBP, unlike DBP, is partially attenuated by the reduction in peripheral amplification that occurs with the development of hypertension in young adult men and to a lesser extent in young women [26]. Therefore, discordantly high brachial DBP predicts the increase in aortic PP more accurately than brachial SBP or brachial PP in young adult subjects with IDH. There is much evidence supporting this concept. Wilkinson and colleagues [27], using pulse wave analysis with applanation tonometry, showed that a rise in brachial DBP was accompanied by an attenuated rise in brachial SBP as a result of decreased peripheral amplification in subjects < age 50 (but not in those ⩾ age 50); thus, narrow brachial PP (IDH) was associated with wider central PP. Similarly, Millasseau and colleagues [28] showed that carotid-femoral PWV, an indicator of aortic stiffness, was more closely correlated with peripheral DBP than SBP in subjects < age 50, but SBP correlated better than DBP with increased PWV in those ⩾ age 50. By the same token, Nurnberger et al. [29] found that DBP, unlike SBP, was strongly correlated with 2 arterial stiffness markers in young males – AIx and aortic PWV.
4. Discordantly low DBP in elderly adults with ISH and ventricular-arterial stiffness
The NHANES III survey [18] showed that ISH becomes the dominant hypertensive subtype by the decade of age 50 to 59. Indeed, after 50 years of age, 80% of all untreated hypertensive persons had the ISH subtype. The Framingham Heart Study [30] showed that the rise in SBP and DBP up to age 50–55 could best be explained by the dominance of peripheral vascular resistance. In contrast, by the seventh decade of life (age 60–69), increasing PP and decreasing DBP were surrogate measurements for increasing central elastic artery stiffness.
The Framingham Heart Study findings also support the concept of an interaction between aging and hypertension in the progressive fall of DBP and rise of SBP [30]. Subjects with mean baseline BPs of 110/70 (Figure 2, group 1) had no rise in PP from age 30 to 54 years of age. Nevertheless, this group of normotensive subjects showed a significant rise in PP and fall in DBP from age 55 to 59 years onward, presumably caused by an increase in large artery stiffness secondary to aging. In contrast, hypertensive subjects with baseline mean BP of 173/90 (Figure 2, group 4) showed a steeper rise in PP and a steeper fall in DBP after age 50 than was observed in group 1 subjects. This divergent rather than parallel tracking pattern observed in group 4 subjects suggest a linkage between untreated hypertension and acceleration of large artery stiffness; in turn, this can perpetuate a vicious cycle of accelerated hypertension and further increases in stiffness. Indeed, hypertension left untreated, can accelerate the rate of vascular aging by as many as 15–20 years, comparing age-related PP changes in group 4 versus group 1 subjects (Figure 2) [30]. Furthermore, increased peripheral vascular resistance may initiate essential hypertension, but acceleration of large artery stiffness is the driving force leading to the steeper rise of SBP after age 50 in the hypertensive groups 3 and 4 as compared to the normotensive groups 1 and 2.

Pulse pressure by age. Group averaged data (left panel) and averaged individual regression analysis (right panel) for all subjects and with deaths, myocardial infarctions, and heart failure excluded. Curves plotted based on blood pressure predicted values at 5-year intervals by systolic blood pressure (SBP) groupings. Adapted with permission from Franklin SS, et al. Circulation 1997;96:308–315.
These findings were confirmed by Benetos et al. [31], who found that annual rates of progression in PWV were higher in treated hypertensive subjects than in normotensive subjects, suggesting accelerated progression of arterial stiffness among the treated hypertensive subjects. In addition, these investigators showed that MAP, a surrogate measure of peripheral resistance, did not increase throughout the 6-year follow-up, but PWV progression was >3 times greater in poorly controlled as compared with the well-controlled hypertensive subjects. Thus, the Framingham and Benetos et al. studies suggest a linkage between untreated or incompletely treated hypertension and subsequent acceleration of age-related large artery stiffness – a measure of vascular aging.
As suggested by their age-dependent divergent patterns of onset, diastolic hypertension and ISH may be two distinct disorders with significant overlap. People who have had untreated or poorly-treated diastolic hypertension at a younger age may develop ISH as they become older and their arteries become stiffer, but data from the Framingham Study suggests that only about 40% of patients with “high peripheral resistance” diastolic hypertension convert to ISH in this manner [14]. The majority of people who developed ISH never go through a stage of diastolic hypertension.
Arterial stiffness is also accompanied by the phenomenon of early wave reflection [3,4,7]. In young subjects the reflected pressure waves return to the ascending aorta in diastole and serve to elevate mean DBP, thus boosting coronary artery perfusion (normal ventricular-vascular coupling). Between the ages of 20 and 70 years, as arteries stiffen, the pulse wave velocity doubles. In older individuals, the reflected pressure wave returns to the ascending aorta earlier during late systole and increases or ‘augments’ the central SBP and PP, thus decreasing pressure amplification and simultaneously contributing to increase cardiac afterload (ventricular-vascular uncoupling) [3,4,7].
Therefore, central and not peripheral SBP, regardless of age, determines cardiac afterload, which is the important component of cardiac risk. The changing pattern of age-related brachial artery BP components that predict CHD risk results from altered peripheral resistance, aortic stiffness, and early wave reflection, all acting in concert to raise SBP, decrease DBP, and abolish pressure amplification; this leads to an age-related shift from sphygmomanometric-determined DBP to SBP and ultimately to ISH and wide PP as the predictors of cardiac risk (Figure 3) [15]. These findings represent a significant paradigm shift in our understanding of how we use brachial artery cuff BP components to predict cardiovascular risk.
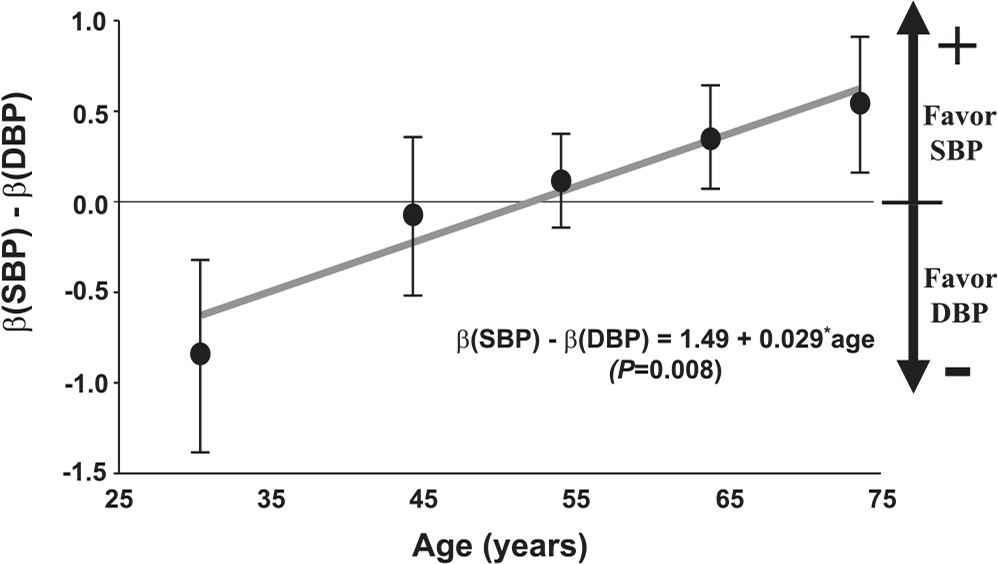
Differences in coronary heart disease prediction between systolic blood pressure (SBP) and diastolic blood pressure (DBP) as a function of age. Difference in β coefficients (from Cox proportional-hazards regression) between SBP and DBP is plotted as function of age, obtaining this regression line: β(SBP) − β (DBP) = 1.49848 + 0.0290 · age (p = 0.008). Adapted with permission from Franklin SS, et al. Circulation 2001;103:1245–1249.
In addition to arterial stiffening, the left ventricle itself becomes stiffer, perhaps as an adaptation to facilitate cardiac ejection and maintain matched coupling of heart to arteries. This is particularly notable in hearts that develop left ventricular hypertrophy – a common occurrence in the elderly with ISH. A stiffer left ventricular coupled to a stiffer arterial system can contribute to increased cardiovascular risk in several ways, as has been shown by the studies of Kass et al. [32–35]. First, there is increased late-systolic wall stress, and the cardiac energy costs imposed on the heart. Second, imposition of increased systolic load during late systole markedly slows cardiac relaxation rates, leading to incomplete relaxation of the left ventricle during diastole, elevated diastolic pressures, and compromised cardiac reserve. This appears to be a factor in patients with heart failure symptoms who have apparent preservation of normal ejection fractions. Third, loss of arterial distensibility appears to alter vascular mechano-signaling, so that the normal augmentations of nitric oxide release and vasoprotective mechanisms with each expansion of the aorta are compromised. Lastly, increased pulsatile stress, secondary to the loss of the conduit artery cushioning function, can contribute to endothelial dysfunction, increased coronary atherosclerosis, rupture of unstable atherosclerotic plaques, and acute coronary heart syndromes [7]. Many of these disturbances in cardiovascular function characterize the elderly person with long-standing ISH and markedly elevated PP.
The conventional wisdom is that the reduction DBP that accompanies ventricular-arterial stiffening results in compromised coronary perfusion. Whereas reflected waves normally return during early diastole and thereby enhance coronary perfusion, this increased boost is absent in elderly persons with ISH [7]; the decline in DBP, however, rarely falls to the critical level of ∼60mmHg required to disturb coronary flow autoregulation [36]. Furthermore, cardiac ejection into the stiff arterial system results in more coronary perfusion during systole. This suggests that the frequent reduction in DBP that accompanies increased PP does not compromise coronary perfusion significantly unless there is a treatment-induced critical reduction in both SBP and DBP in conjunction with severe coronary artery stenosis. It is more likely that the reduction in DBP that occurs in most individuals with ISH is primarily a surrogate risk marker for ventricular-arterial stiffness.
In summary, coupling disease, resulting from stiffness of both the heart and large elastic arteries, interacts to produce diastolic dysfunction and heart failure; this results from the combination of an elevated cardiac afterload presented to a compromised left ventricle, which is unable to handle the load. Thus, cardiovascular risk of an increased PP is defined by: (1) increased SBP, a marker of cardiac afterload; and by (2) discordant decreased DBP in association with an increased SBP, a marker of increased stiffness of the left ventricle and the proximal aorta.
5. Therapeutic determinants of cardiovascular outcome: DBP versus SBP
The question as to what extent lowering of SBP versus DBP with antihypertensive therapy contributes to a reduction in cardiovascular events was investigated by Wang et al. [37]. They performed a large meta-analysis of trials in hypertension, comparing active drug treatment against placebo or no treatment in the young (30–49 years of age), the old (60–79 years of age), and in the very old (⩾80 years of age). This study confirmed the earlier work of Koch-Weser [38] that antihypertensive therapy maximized the decrease in SBP and minimized the reduction in DBP in direct proportion to the age-related stiffening of large arteries; the degree of stiffening was reflected in the pre-treatment elevation of PP. In spite of the differential lowering of SBP and DBP in this metaanalysis, antihypertensive treatment reduced the risk of all cardiovascular events in the three age strata to a similar extent. Furthermore, a matched-pair analysis corroborated the hypothesis that the degree of DBP reduction did not lead to differences in cardiovascular outcome as long as SBP decreased substantially; lowering the DBP below 70mmHg did not decrease the benefit of treatment. This retrospective study supports the hypothesis that benefit of treatment is directly related to a reduction in cardiac afterload, as defined by a reduction in SBP. It follows that a reduction in large artery stiffness and in early wave reflection raises DBP, whereas a reduction in peripheral resistance lowers it. Thus, the beneficial therapeutic lowering of SBP may be accompanied by a minimum or no reduction in DBP, as was observed in some elderly persons with ISH; in this situation the decrease in arterial stiffness and early wave reflection dominated over a decrease in peripheral resistance. Therefore, while discordant DBP may be predictive of cardiovascular risk and increased elastic artery stiffness, a thesis put forward in this review, the DBP response to treatment does not define cardiovascular benefit.
References
Cite this article
TY - JOUR AU - Stanley S. Franklin PY - 2007 DA - 2007/06/13 TI - Arterial stiffness and diastolic blood pressure: what is the connection? JO - Artery Research SP - S1 EP - S6 VL - 1 IS - S1 SN - 1876-4401 UR - https://doi.org/10.1016/S1872-9312(07)70001-7 DO - 10.1016/S1872-9312(07)70001-7 ID - Franklin2007 ER -