
The arterial system; its influence on the heart and circulation
- DOI
- 10.1016/S1872-9312(07)70002-9How to use a DOI?
- Keywords
- arterial pulse; arterial stiffness; wave reflection; blood pressure; heart failure
- Copyright
- © 2006 Published by Elsevier. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
From antiquity the arterial pulse was associated with life, and its absence with death. The pulse was considered to carry vital information on the state of health, and was a central part of the physical examination in Chinese, Greek and Arabian medicine [1]. Untold numbers of paintings show the physician feeling the radial artery pulse – though rarely conducting any other sort of examination.
The Roman physician Galen (AD ?130–?200), had a strong influence on this field for over fifteen hundred years. He wrote voluminously on the pulse in a series of tomes that came to assume huge influence in subsequent years – though not at the time of his life [1]. It appears that he was a loner, and not one of influence among contemporary colleagues. He had no pupils, acolytes or disciples. His characterisation of pulses was incomprehensible. But it survived unquestioned until the time of William Harvey [2].
1. Harvey
Modern scientific medicine began with William Harvey, whose great work was done in London while in practice at St. Bartholomew’s Hospital, and as an anatomist to the recently formed Royal College of Physicians. The College still has as its crest an illustration of a physician’s fingers palpating the arterial pulse. Harvey had been educated in the traditions of Galileo through studies in Padua. His brilliant monograph de Motu Cordis et Sanguinis in Animalibus [2] remains the most important application of the scientific method in all medical history. Such being the case, it is surprising how few modern physicians or cardiovascular researchers have read any translation of the original Latin text. Fewer still have read or even been aware of the criticism that Harvey faced, and the way that he defended his views – most notably in his open letters to Jean Riolan of Paris [3].
The view that Harvey proposed is now universally accepted, but it was highly controversial at the time. Harvey’s views were based on human anatomy, namely the size of the heart in systole and diastole, the function of veins, on comparative physiology and quantitative assessment. He proposed that oxygenated blood was propelled by left ventricular contraction into the arterial tree, then was “continuously, evenly and uninterruptedly driven by the beat of the arteries into every member and part”, then through veins, back to the heart, then from the right heart through similar small blood vessels in the lungs back to the left atrium and ventricle. He challenged the existing notion that arteries contain air, and that they expanded and contracted themselves independently of the heart. He stressed that they acted passively to accept blood from the left ventricle, and that left ventricular systole (contraction) caused arterial diastole (expansion), and that arterial systole (relaxation) occurred during cardiac diastole when the two systems were separated by the closed aortic valve.
Harvey was a tolerant man and knew he was asking for a huge leap for others to accept his arguments. He praised his predecessors and where possible pointed out where other persons’ views led on to his own. He even quoted Galen (whose basic views were utterly at odds) in relation to an experiment where a reed was used to occlude an artery with resulting strong reflection upstream – and in unambiguous terms “unde et fluxus inhibitor et impetus refringitor eo quod supra ligaturiam reverberatur”.
Harvey’s tolerance was limited, and so it was in 1649, 21 years after publication of de Motu Cordis that he wrote his second open letter [3] to Jean Riolan, first urging others against extremes in uncritical acceptance or malicious dismissal of any new technique, then attacking the latter in words that would now be considered improper, even defamatory:
“There are, moreover, those who cry out that I have striven after the empty glory of vivisections, and they disparage and ridicule with childish levity the frogs, snakes, flies, and other lower animals which I have brought on to my stage. Nor do they abstain from scurrilous language. To return scurrility with scurrility, however, I judge unworthy in a philosopher and searcher after truth. I think it will be better and wiser to tone down these many indications of bad manners by the light of true and trustworthy indications. It is unavoidable that dogs bark and vomit their surfeit, or cynics are numbered among the assembled philosophers, but one must take care that they do not bite, or kill with their savage madness, or gnaw with a canine tooth the very bones and foundations of truth. While I resolved with myself that censurers, mummers, and stain-defiled writers of disapprobations should never be read (as being men from whom nothing sound or remarkable except scurrility was to be expected), I judged them even less worthy of answer. Let them enjoy their evil nature: I think they will scarcely ever have well-disposed readers: and the most good God does not give to the wicked that which is most outstanding and most to be desired, namely, wisdom. Let them continue with their scurrility until it irks if it does not shame them, and finally tires them out.”.
2. Hales & Poiseuille
Harvey’s work was of as much interest to natural philosophers (including members of England’s Royal Society) as it was to physicians, who in any case had little way to apply it in the seventeenth and eighteenth century. One such philosopher was the clergyman Stephen Hales, who conducted studies in vegetable statics (including movement of sap in trees) and on haemostaticks [4], and was the first to measure arterial pressure (from the height the column of blood rose in a glass tube connected to a horse’s crural artery). This was a measure of mean arterial pressure since inertia of the system prevented pulsations being accurately recorded. The value was measured at around 4–5 feet of blood, corresponding to around 100 mmHg. Hales showed the initial fall, then compensation in consequence of blood loss. Hales is credited with the concept of the Windkessel model of the arterial tree (distensibility of central arteries which cushioned flow pulsations and confined pulsations to these) [1,5], and the concept of vascular resistance residing in small peripheral blood vessels [6]. The French medical scientist J.L.M. Poiseuille confirmed the latter, having shown that pressure fall is trivial in the arterial vessels leading up to the microcirculation [7]; Poiseuille’s later work on viscosity and resistance was deliberately conducted in capillary tubes because of their physiological relevance to vascular resistance [8]. Poiseuille also showed how arterial pressure could be measured more easily in mmHg and arranged a system where this could be recorded graphically [7].
Poiseuille’s work in the nineteenth century was accompanied by other studies of arterial elasticity and pulse wave velocity by Thomas Young [5,6] and on the physical principles of pulsatile blood flow in rigid and distensible tubes by many others. All this was summarised in the first and subsequent editions of McDonald’s Blood Flow in Arteries [5]. Nothing quite as contentious as Harvey’s correspondence arose from this basic research.
3. London and Guy’s Hospital
On the clinical scene, progress in the nineteenth century was associated with appreciation of the problems of high arterial pressure. Richard Bright [9,10] at Guy’s Hospital in London had associated “hardness of the pulse” (denoting high blood pressure) with albuminuria, contraction of the kidneys, left ventricular hypertrophy, cardiac failure and stroke. Many of his cases had glomerulonephritis, and this was considered the cause of high blood pressure. After Bright’s death, this work was continued at the same hospital by Gull and Sutton who suspected that the condition described by Bright was due to generalised arteriolar constriction causing high peripheral resistance and arterial pressure, with secondary kidney damage [10]. Such views were presented gently to a receptive audience, and were supported by introduction of a quantitative sphygmogram by Frederick Mahomed, initially while a medical student at Guy’s [10]. Mahomed showed high arterial pressure could be assessed from the form of the radial artery pulse. Using this method he subsequently described the natural history of what we now call essential hypertension, and confirmed that high arterial pressure could result from or lead to disease of the kidneys [5,10].
Mahomed’s instrument was an advance on that originally described by Etienne Marey in Paris during 1861. Marey [11] was more interested in movement than in medicine, though he had a medical training. He was the first to describe the effects of age on contour of the radial artery pressure pulse – as subsequently confirmed by Freis, Kelly and others (Figure 1 [5]).
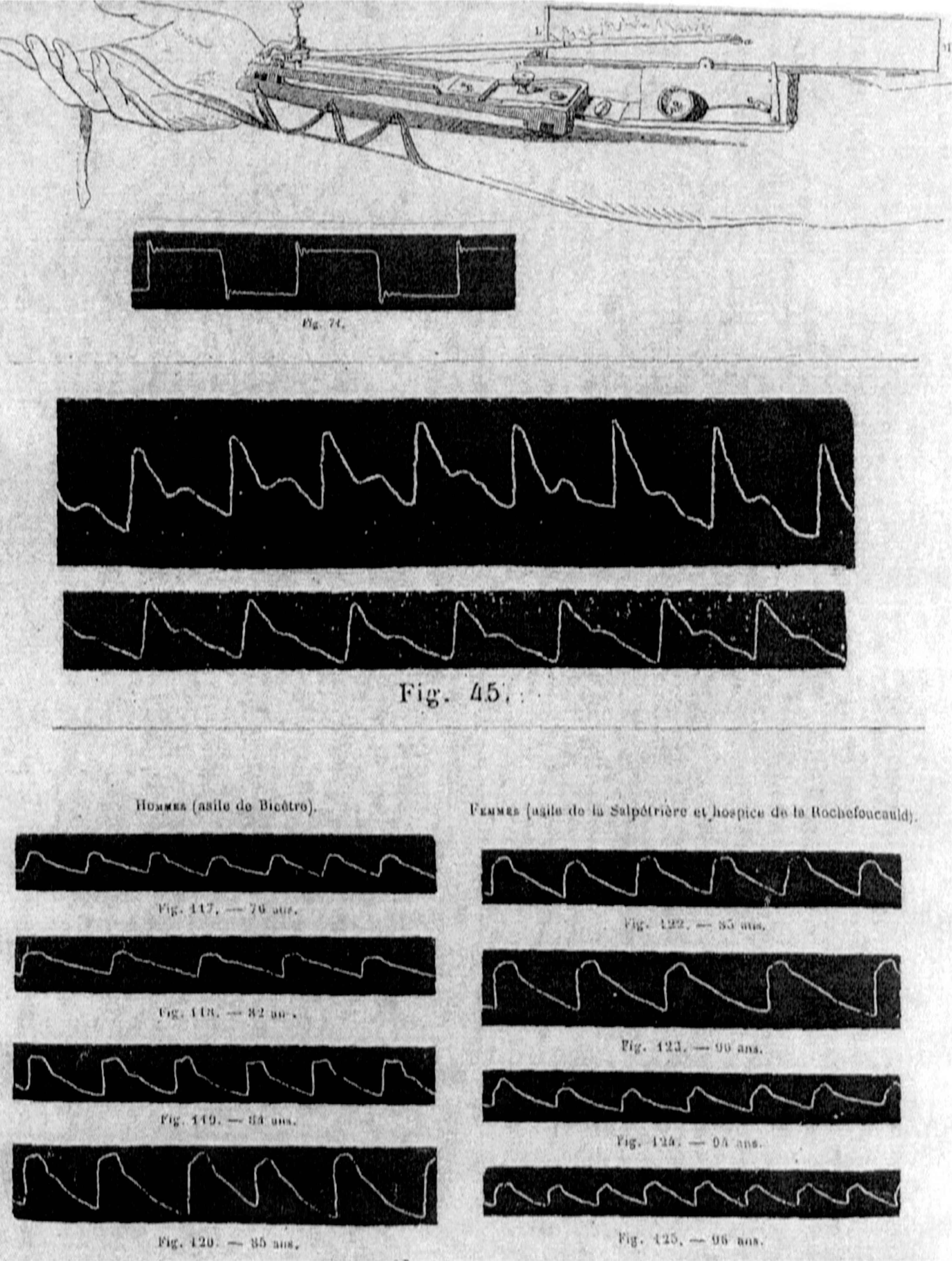
Illustrations from Marey’s (1863) original publication on the sphygmogram. Top: The original instrument, with base-plate applied over the radial artery, with long stylus, pivoting near the site of recording, drawing an amplified signal on smoked paper which was moved by a clockwork mechanism. Inset below is a ‘square wave’ test to establish frequency response and instrument artefact. Center: Sphygmogram tracings in two young adults, showing typical young radial patterns. Bottom: Sphygmogram tracings in old men (left) and women (right), showing typical patterns of senescence. From Nichols and O’Rourke (2005) [5].
In the nineteenth century, French and English sphygmograms were difficult to use, but they did give information on arterial pressure, and on cardiac rhythm, that was not available by any other method. In 1879 the first description of glyceryl trinitrate as an anti-anginal agent was accompanied by an illustration of the radial artery pulse which is virtually identical to that reported by Kelly et al. over a century later (Figure 2 [5]). Books and journals were liberally illustrated with sphygmograms. By the turn of the century Sir James Mackenzie [12] had emerged as the most prominent physician in England on the basis of his books on the heart and the pulse, and on his use of sphygmograms in clinical practice. Mackenzie founded the journal “Heart” and is generally regarded as the first cardiologist in the English-speaking world. His view on heart failure was that this is attributable to myocardial exhaustion, as a consequence of arterial stiffening. This fits well with current views on the paramount importance of left ventricular load and left ventricular systolic pressure in development of heart failure [13,14]. The main controversy about this time appears to have been proprietorial, between two English enthusiasts who claimed credit for initial clinical application, and whose feuding led to a Lancet editorial on plaguarism [15]. The Dudgeon sphygmograph was a beautiful little device favoured by Mackenzie [12], that sold around the world including to a Sydney suburban general practice. Dudgeon wished to improve the art of pulse interpretation which he described [16] as follows:
“The physician of old made his diagnosis chiefly by observation of the pulse and tongue. But, as the tongue could be rapidly inspected, and anyone could judge of its foulness or cleanness as well as himself, he concentrated his attention mainly on the pulse, in the feeling of which there was always scope for affecting the possession of peculiar skill and insight. To the uninitiated who regarded the doctor as the depositary of occult knowledge, and who received his dicta as though they were oracles, there was something very imposing in his method of pulse-palpation. The fingers of the right hand daintily grasping the patient’s wrist, while the doctor’s eyes were riveted on the loud-ticking gold chronometer he held in his left hand, his head gravely nodding the while synchronously with the arterial pulsations – all this formed a picture calculated to inspire beholders with reference and awe”.

Radial artery sphygmograms published by W. Murrell (Nitroglycerin as a remedy for angina pectoris. Lancet 1879: 80–81, 151–151, 225–227). Tracings show progressive reduction in amplitude of the late systolic reflected wave. From Nichols and O’Rourke (2005) [5].
4. Riva Rocci
Introduction of cuff sphygmomanometric methods for blood pressure recording, first by Riva-Rocci, then by Korotkov [17], led to the demise of the sphygmograph for blood pressure recording, while development of electrocardiography by Eithoven and clinical application by Lewis and others found another method for identifying cardiac arrhythmias [5,18]. By 1917, the value of systolic blood pressure measurement for life insurance risk had been confirmed [18]. Cuff sphygmomanometry then came to dominate clinical practice though it was not until the end of the twentieth century that views on diastolic pressure and pulse pressure were challenged. This was not the initial response. Korotkov had a hard time gaining recognition for his auscultatory method for determining systolic and diastolic pressure [17].
5. Cardiovascular physiologists
Through the early and mid twentieth century, methods were improved for direct measurement of arterial pressure and flow, notably in the USA whence scientists had fled from war-ravaged Europe. This too is summarised in the McDonald books [15,19]. Most prominent were Wiggers in Cleveland, Hamilton and others in Augusta, Georgia, and with clinical applications pressed by Paul Wood at the Mayo Clinic. A turning point was introduction of pulse waveform study in the frequency domain by Donald Macdonald and his colleagues John Womersley and Michael Taylor in London’s St. Bartholomew’s Hospital (where Harvey had practised) [5,6,19]. Basic to this was an assumption that the arterial system behaved in a linear fashion with respect to pressure and flow. This clearly was not the case, though Womersley’s theoretic studies suggested that nonlinearities were sufficiently small to be neglected to a first approximation [6]. Taylor’s subsequent experimental work on vascular impedance and pressure/pressure transfer functions showed that nonlinearities were indeed far smaller than he and others had originally thought. This work moved on to explain pressure and flow in the arterial system in terms of wave travel and reflections. Details are summarised in the McDonald third to fifth editions [5].
Original reaction to McDonald’s work was profoundly sceptical. Data to support this was slow to emerge, and McDonald was a colourful and undiplomatic character [20]. He was uncompromising in his view that pressure and flow waves could only be analysed properly in the frequency domain, and declined to consider how wave reflection may influence pressure and flow displayed by waveforms as a function of time (ie. in the time domain). This was the only way that contemporary physiologists operated. Consequently McDonald’s views were systematically ignored by the American Physiological Society and its handbooks and reviews, with the first such not appearing until 1980 [21]. But others, including Taylor and his colleagues in Sydney, Milnor in Baltimore, Murgo in San Antonio and Westerhof in Amsterdam linked both approaches. By 1998, and in the fourth edition of McDonald’s book, and 25 years after his death, there was general acceptance of his views on frequency analysis, but there was agreement that these could be considered with traditional analyses – and with all showing evidence of wave travel and strong wave reflection in the arterial tree.
6. Human application
Human application was advanced by introduction of a catheter-mounted electromagnetic flow meter by Mills from London in 1966, and a micromanometer by Millar and Murgo shortly afterwards. Use of these instruments at cardiac catheterisation extended the studies on experimental animals, but showed that humans were different, with far higher aortic impedance and pulse wave velocity than seen in experimental animals [5]. This accounted for the characteristically different waveforms in older humans, and the evidence of deterioration in vascular/ventricular interaction that appeared to be the norm in humans by the age they came to cardiac catheterisation.
A series of studies on ascending aortic impedance at cardiac catheterisation was done in different countries – notably in the USA, France and Japan from 1975 to 1995 and these established aging change, effects of disease and of drugs [5]. These however lapsed, and for a number of reasons. The catheters were very expensive, and not always approved for multiple use. The flow waveforms were subject to distortion as a consequence of disturbed flow in the ascending aorta close to the heart. General agreement had been reached on the effects of age, hypertension, cardiac failure and of drugs. Non-invasive methods were improving and were far easier to apply.
Echocardiographic techniques are now widely used for measurement of ascending aortic flow velocity in routine assessment. These have been used with non-invasive carotid pressure (as a surrogate of ascending aortic pressure) for determination of ascending aortic impedance since 1988 [22]. Mitchell and colleagues [23] and others have extended this work in recent times and have confirmed and advanced the invasive studies.
7. Tonometry supplements the brachial cuff
An important advance for non-invasive measurement of the arterial pressure waves was Millar’s development of the applanation tonometer [5]. Similar devices are now made by other manufacturers. All use the same principle as used in ocular tonometry, flattening of a small segment of the anterior wall of the artery. When this is achieved throughout a cardiac cycle, the pressure wave is identical to that recorded within the artery [24]. These instruments are far more accurate and far easier to use than the mechanical sphygmogram, and more accurate than the microphonic systems as used for systolic time intervals in the 1970s.
Extensive studies of carotid tonometry have now been published. Carotid tonometry is presently being implemented as part of the Framingham study. The carotid pressure wave can be calibrated against upper limb pressure by assuming that mean pressure and diastolic pressure are the same in the carotid artery as in the brachial or radial artery; systolic pressure can then be calculated from the digitized waveform by extrapolation [22]. This technique has acceptable accuracy (assuming cuff pressures are accurate) and can also be applied to the carotid diameter waveform [25,26]. Studies of carotid tonometry have to date provided conflicting results. Use with measured or assumed cardiac output for measuring systemic arterial compliance has not shown the clear-cut aging changes demonstrated through measurement of aortic pulse wave velocity. Calculation of central systolic pressure has not always been shown superior to brachial cuff pressures or to measurement of pulse wave velocity in outcome studies. These problems could be technical. We have found the carotid pressure waveform difficult to measure accurately and reproducibly, and uncomfortable for the patient [27]. We have also been concerned about dislodging plaque, especially when an operator has difficulty measuring the wave reproducibly through the full cardiac cycle, and seeks to persevere. In consequence we have preferred to generate aortic pressure from the radial pressure waveform.
Measurement of the radial pressure wave is hallowed by history, and was the technique used by Mahomed, Mackenzie and others over a five decade span (see above). Records can be made easily, reproducibly and with no discomfort to the patient, and without the risks posed for the carotid. Calibration can reasonably be made directly with the brachial pressure cuff values [5]. Central systolic and pulse pressure can be measured directly from the radial pressure wave through identification of the beginning of a reflected wave in later systole, but is generally undertaken through use of transfer functions which can be used to synthesise the whole aortic systolic pressure wave [5]. This is the technique provided by the SphygmoCor process (and with whose manufacturer, AtCor Medical, M. O’Rourke is associated). Use of a generalised transfer function to generate central aortic from radial pressure waveform has been approved by the US FDA following a host of validation studies [5,28,29]. It does involve the same technique as introduced by McDonald, and extended by Taylor and colleagues [6]. Challenges still appear in the literature to this method [30,31], but even these most ardent detractors have published data which is similar to that presented by others and used in the SphygmoCor system (Figure 3). The need for some form of transfer function to allow for distortion of the pressure pulse in the upper limb is apparent from all published transfer functions [5,29]; all show substantial deviation from unity at frequencies between 2 and 7 Hz.

Modulus of transfer functions for pressure waves between radial artery and aorta as calculated from data published by Hope, Jay, Meredith and Cameron in J Hypertens 2003;21:1299–1305 [30] and Heart Lung Circulation 2004;13:S267 [31]. Harmonic number adapted to heart rate from average value in text; amplitude calculated as radial ÷ aortic by inversion of published data. Transfer functions with the two different catheter systems, under control conditions and with Valsalva manoeuvre are similar to those published by others [5,29] and as used in a commercial (SphygmoCor) device over the range 0–6 Hz which normally contains 99% of waveform energy.
8. Modern blood pressure studies
Modern views on the arterial system are different to what they were twenty years ago, or even five years ago. Twenty years back, diastolic blood pressure levels were regarded as all important, and were required for a diagnosis of hypertension to be made. The landmark SHEP trial [32] transformed this. Now, diastolic pressure is largely ignored in treatment of patients over age 50 and systolic (or pulse) pressure is considered all important. Elevated systolic pressure is now considered as the principal cause of the epidemic of heart failure in the elderly [14]. Inaccuracy of casual clinical blood pressure recordings is increasingly recognised and recourse is now taken more frequently to measurement on multiple occasions at home. Lower levels of pressure are now targeted for treatment than before, especially in the presence of diabetes mellitus, renal insufficiency and cardiac failure [5].
Central aortic pressure is increasingly seen as of greater importance than brachial. That this should be so appears obvious, and has been confirmed recently in the CAF’E substudy of ASCOT [33], the STRONG heart study [34] and the REASON trial [35]. Measurement of central aortic pressure requires measurement of the pressure waveforms, and combines the ease of cuff sphygmomanometry with the benefits of the old technique of sphygmography.
9. Pulsations enter the microvasculature
Attention is now being focused on arterial stiffness as a cause of cardiovascular events especially in older persons, as well as in persons with diabetes mellitus, renal failure and cardiac failure. While explanations have been readily given as to how arterial stiffening increases left ventricular and aortic systolic pressure and so predisposes to left ventricular hypertrophy, cardiac failure and angina [5], attention is now shifting to the microvasculature [36]. Harvey [1] had referred to the microvasculature as being perfused “continuously, evenly and uninterruptedly” throughout the cardiac cycle as a consequence of the elastic properties of arteries. With large artery stiffening, pulsations cannot be cushioned in the large arteries, and extend further down into the microvasculature, particularly that in the highly perfused organs (brain and kidneys) [37]. High flow pulsations have been confirmed in cerebral arteries, and have even been shown extending through into the venous sinuses [38]. Such high pulsation in the microvasculature appears to be responsible for partial rupture, with haemorrhage from these vessels resulting in fibrinoid necrosis and amyloid deposits and for endothelial damage and thrombosis with resultant micro-infarcts [37]. Evidence is emerging that this is substantial in older persons, and is exaggerated when the smaller vessels are unusually fragile, as in diabetes mellitus, and/or when control of vasomotion is impaired [39]. Evidence is emerging that the major problems of modern society (dementia and renal failure) are due to such later microvascular damage [40] as well as to the earlier aortic damage consequent on elastin fibre fracture and arterial stiffening [5].
10. A gathering storm
The points of view presented here refer to the arterial system as a whole and appreciation of its role as conduit and cushion, and with problems arising principally from disturbance of the cushioning role. This is not the view in modern cardiology, where preoccupation persists with atherosclerotic disease, and with imaging techniques, and where all arterial disease in vessels of any size and in all organs is addressed in terms of atherosclerosis and organ ischaemia. The majority of practising cardiologists are involved with procedures directed at identifying arterial narrowing and relief of arterial narrowing. The majority of hospitals at which such persons work have a huge investment in diagnostic equipment directed towards ongoing practice of angiography and angioplasty. These hospitals and these cardiologists are served by a huge imaging industry. Modern cardiologists see modern problems in terms of images rather than physiological mechanisms. Currently, members of organisations such as the American College of Cardiology are exerting pressure on government agencies to extend imaging techniques and their reimbursement, at the expense of other procedures and treatments. Problems in such an approach are emerging in the lay press. The New York Times reported (18th April 2006) on the problems of angina in women, quoting eminent authorities, and considered only macrovascular and microvascular narrowing and none of the other physiological mechanisms which determine myocardial blood need and supply. The Boston Globe (25th July 2006) questioned publication of a supplement in the American Journal of Cardiology which promoted expensive imaging techniques which had not been shown incrementally beneficial to current methods: publication had been sponsored by industry, and papers had not proceeded through this journal’s regular review process.
This article has described the controversies that have been associated with different phases of knowledge in arterial function, with the most intense at the very beginning. It is likely that further debate lies ahead, and will represent the interests of clinical cardiologists and imagers against those who appreciate the totality of arterial function, and the multiple ways in which disease can occur, can be measured, and can affect the human race.
Disclosure of interest
Dr O’Rourke is a founding director of AtCor Medical, Sydney, Australia.
References
Cite this article
TY - JOUR AU - M.F. O’Rourke AU - J. Hashimoto PY - 2007 DA - 2007/06/13 TI - The arterial system; its influence on the heart and circulation JO - Artery Research SP - S7 EP - S14 VL - 1 IS - S1 SN - 1876-4401 UR - https://doi.org/10.1016/S1872-9312(07)70002-9 DO - 10.1016/S1872-9312(07)70002-9 ID - O’Rourke2007 ER -