
Comparison of augmentation index derived from multiple devices
- DOI
- 10.1016/j.artres.2011.06.002How to use a DOI?
- Keywords
- Arterial wave reflection; Augmentation index; Arterial stiffness; Applanation tonometry; Vascular device
- Abstract
One of the most commonly evaluated features of the arterial pressure waveforms is augmentation index (AI). Multiple devices have been developed and marketed that measure AI at peripheral arteries. Currently, it is not known if and how these measures of AI are related. Aortic and radial AI (using SphygmoCor), radial AI (Omron), and finger AI (Itamar) were measured in 40 apparently healthy subjects. All the AI values were correlated with each other with Pearson r-values ranging from 0.78 to 0.94. The coefficients of variation ranged from 3.4 to 20.0%. We concluded that even though the absolute values derived by each technique were different, there were high and significant correlations between AI values.
- Copyright
- © 2011 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
Since the very beginning of medicine, the arterial pressure pulse has served as an important window from which to assess health and well-being.1 One of the most commonly evaluated features of the arterial pressure waveform is the magnitude of secondary rise in pressure or pressure augmentation that is commonly expressed as augmentation index (AI).2,3Higher values of carotid artery AI are associated with an increased risk of cardiovascular mortality,4 a reduction in maximal aerobic capacity,5 and a more rapid onset of exercise-induced ischemia.6 One major technical issue with the classic measurement of AI is its reliance on applanation of superficial central arteries (e.g., carotid artery) by hand-held tonometry. Because peripheral arteries are typically easier to access and isolate than central arteries, multiple devices have been developed and marketed that measure AI at peripheral arteries (e.g., finger, wrist) using various technologies (e.g., tonometry, plethysmography).Currently, it is not known if and how these measures of AI are related.7 Such information is important as an increasing number of studies are reporting that various measures of AI provide prognostic information. Accordingly, the aim of the present study was to determine the relations among commonly-used methodologies for assessing AI.
Methods
Forty apparently healthy subjects (28 males, 12 females) aged 19–68 years (mean ± SD; 32 ± 13 years) were studied. All subjects were normotensive, non-obese, non-smokers, and free of overt cardiovascular diseases as assessed by medical history. The study was approved by the institutional review board, and written informed consents were obtained from all subjects.
Subjects fasted and abstained from coffee and alcohol for at least 4 h before the start of the study. Subjects rested quietly in a supine position in a dimly-lit, temperature-controlled (23–25 °C) laboratory room for 30 min before measurements. Augmentation index was measured using three different methodologies on the same day. In order to determine the variability and reliability, multiple measurements were made with each device.
Radial artery AI was measured using an applanation tonometry-based automated AI measurement device (HEM-9010AI; Omron Healthcare, Kyoto, Japan).3 Radial AI was calculated as the ratio of the amplitude of the late systolic peak to the amplitude of the early systolic peak. The Endo-PAT 2000 device (Itamar Medical, Franklin, MA) was used to obtain a beat-to-beat plethysmographic recording of the finger arterial pulse wave amplitude.8 Finger AI was calculated as (the late systolic peak minus the early systolic peak) divided by the late systolic peak. Both aortic and radial AIx values were obtained by applanation tonometry using the SphygmoCor Vx (AtCor Medical, Sydney, Australia).9 The radial artery waveforms were recorded, and the system software was then used to derive a central aortic pressure waveform using a generalized transfer function.
Pearson product moment correlational analyses were used to determine the relation among measures of AI by different methodologies.
Results
Table 1 displays inter-correlations among augmentation index values determined by different methods. All the augmentation index values were correlated with each other with Pearson r-values ranging from 0.78 to 0.94.Table 2 shows the reproducibility data of each technique. The first and second measurements were not different and were highly correlated with coefficients ranging from 0.94 to 0.98. The coefficients of variation were 3.4–20.0%.
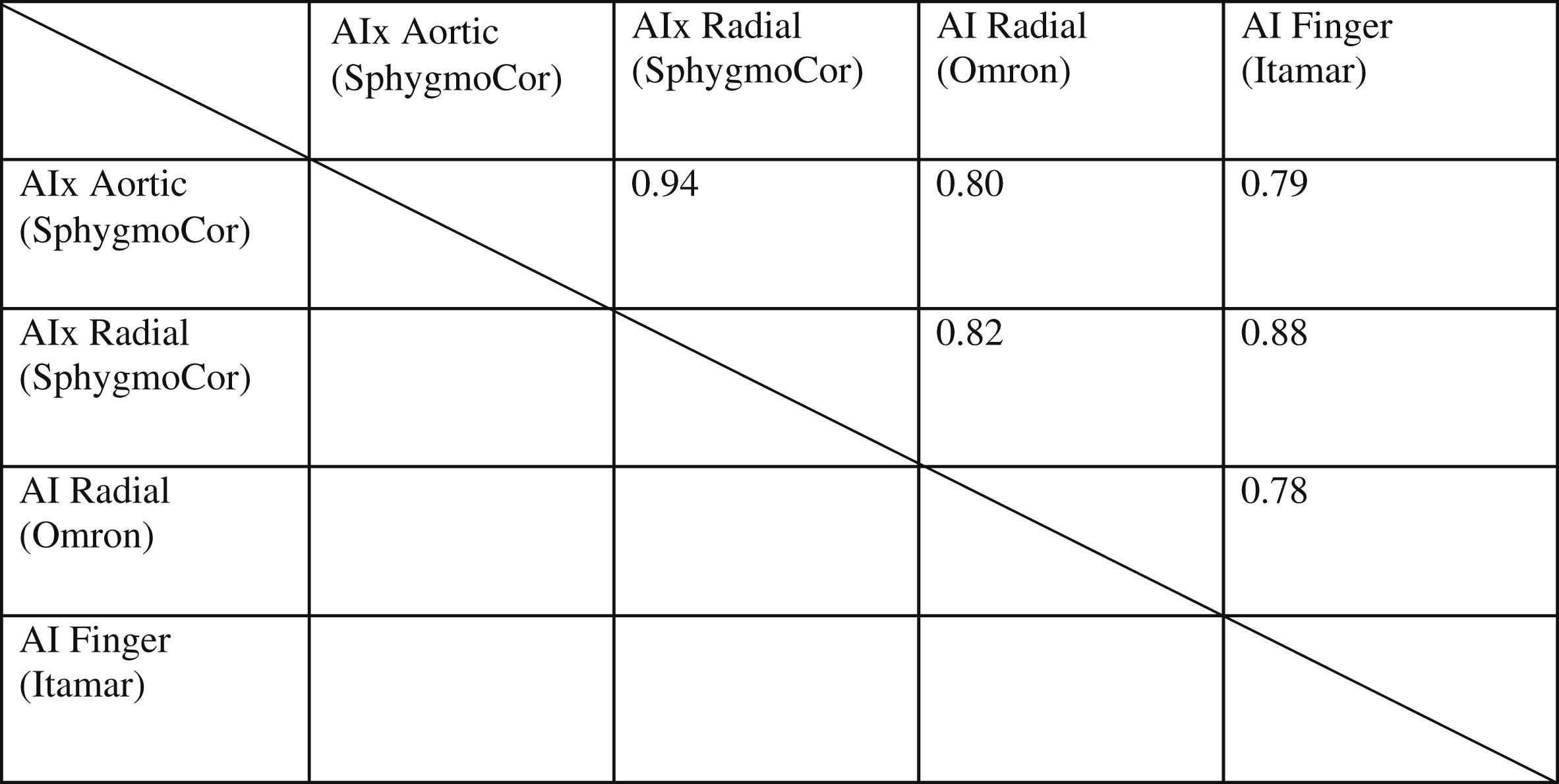
Inter-correlations among augmentation index derived from different technologies.
| 1st reading | 2nd reading | Pearson’s r | CV | |
|---|---|---|---|---|
| AIx Radial SphygmoCor (%) | 54.1 ± 20.9 | 53.6 ± 20.1 | 0.98 | 8.2% |
| AIx Aortic SphygmoCor (%) | −4.6 ± 16.1 | −4.2 ± 15.9 | 0.98 | 20.0% |
| AI Itamar (%) | −10.7 ± 20.5 | −8.8 ± 27.2 | 0.94 | 16.1% |
| AI Omron (%) | 55.5 ± 14.0 | 55.6 ± 13.4 | 0.98 | 3.4% |
Data are means ± SD. CV=coefficient of variation.
The reliability data for augmentation index derived from different technologies.
Conclusion
In the present study, inter-relations among commonly-used methodologies for assessing augmentation index were determined. There were high and significant correlations between AI values even though the absolute values derived by each technique were different. The disparity between absolute values is not surprising as these techniques assess AI in various vascular beds using different techniques and conversions.
References
Cite this article
TY - JOUR AU - Mandeep Dhindsa AU - Jill N. Barnes AU - Allison E. DeVan AU - Jun Sugawara AU - Hirofumi Tanaka PY - 2011 DA - 2011/07/02 TI - Comparison of augmentation index derived from multiple devices JO - Artery Research SP - 112 EP - 114 VL - 5 IS - 3 SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2011.06.002 DO - 10.1016/j.artres.2011.06.002 ID - Dhindsa2011 ER -