
Lifestyle modification-induced increase in serum testosterone and SHBG decreases arterial stiffness in overweight and obese men
- DOI
- 10.1016/j.artres.2014.04.003How to use a DOI?
- Keywords
- Testosterone; Obesity; Lifestyle modification; Arterial stiffness
- Abstract
Background: Arterial stiffness—a risk factor for cardiovascular diseases—is more frequently observed in obese men. Moreover, the male sex hormone testosterone has an anti-atherogenic effect. Serum testosterone levels are found to be lower in obese men than in age-matched normal-weight men. However, the effect of lifestyle modification on testosterone in obese men has not been elucidated. Here, we examined the effect of lifestyle modifications on serum testosterone levels and arterial stiffness in overweight and obese men.
Methods: Eleven overweight and obese men (mean age: 53 ± 3 years) completed a 12-week lifestyle modification program. Before and after the program, we measured the mean blood pressure (MBP), carotid-femoral pulse wave velocity (cfPWV; as an index of arterial stiffness), and the serum total testosterone levels in all participants.
Results: We observed a significant weight loss after the 12-week lifestyle modification program. After the program, MBP and cfPWV significantly decreased and serum testosterone levels significantly increased. Moreover, we observed a negative relationship between the change in serum testosterone levels and that in cfPWV, although this relationship was affected by change in MBP.
Conclusions: Lifestyle modification increased the serum testosterone levels in overweight and obese men. The increase in serum testosterone levels was associated with a corresponding reduction in MBP and arterial stiffness. These results suggest that an increase in the testosterone levels may be an important mechanism underlying the beneficial effect of lifestyle modification on arterial stiffness. However, the association may not be direct, but may be mediated by a change in the MBP.
- Copyright
- © 2014 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
The prevalence of obesity continues to increase worldwide. Obesity has been identified as an independent risk factor for cardiovascular morbidity and mortality.1,2 In addition, increased arterial stiffness is a well-known independent risk factor for cardiovascular disease.3,4 Several studies have shown that arterial stiffness is higher among obese individuals than among non-obese individuals.5,6 We previously reported that lifestyle modification (dietary modification or aerobic exercise training) decreases arterial stiffness in overweight and obese men.7,8 However, the mechanism underlying this decrease in obese individuals has not yet been clarified.
Obesity and aging lead to decreases in serum testosterone levels.9 Foresta et al. reported that the level of serum testosterone in obese men is lower than that in age-matched non-obese men.10 Moreover, decreased serum testosterone levels are reportedly associated with cardiovascular morbidity and mortality.11 Therefore, a low serum testosterone levels in obese individuals is a risk factor for cardiovascular disease. Sex hormone binding-globulin (SHBG)—a glycoprotein produced by the liver—contributes to the action of testosterone on vascular function. Testosterone combines with SHBG to induce vasodilation.12–14 However, the effect of lifestyle modification on serum testosterone and SHBG levels in obese men remains unclear.
In the present study, we aimed to clarify the effect of lifestyle modification (dietary modification and aerobic exercise training) on arterial stiffness, serum testosterone levels, and serum SHBG levels in obese men. We hypothesized that lifestyle modifications would increase the serum levels of testosterone and SHBG and decrease arterial stiffness in obese individuals. To examine our hypothesis, we measured the serum levels of testosterone and SHBG, as well as carotid-femoral pulse-wave velocity (cfPWV; as an index of arterial stiffness), in obese individuals.
Methods
Participants
At baseline, 15 overweight and obese men were enrolled in the present study; of these, 4 men dropped out due to personal reasons or following the recommendation of a physician. Finally, 11 overweight and obese men (mean age, 53 ± 3 years; mean body mass index [BMI], 30 ± 1 kg/m2) completed the lifestyle modification program. None of the participants had any apparent cardiovascular diseases, as assessed by medical history and physical examination. The participants’ smoking habits and medication use did not change across the study period. This study was reviewed and approved by the institutional review board of the University of Tsukuba. All study procedures and potential risks were explained to the participants and each participant provided written informed consent for study participation.
Experimental design
All the overweight and obese men were studied before and after the 12-week lifestyle modification program (dietary modification and aerobic exercise training). All the measurements were recorded after the participants abstained from caffeine and after an overnight fast, and none of the participants exercised the day before the measurements were recorded. Participants were examined under supine resting conditions in a quiet, temperature-controlled room (24–26 °C). All measurements were performed after a rest period of at least 20 min.
Dietary modification
The dietary modification protocol is a low-calorie diet intervention that affects body composition, body fat distribution, and coronary heart disease risk factors.7,15 Based on the diet protocol used in this study, all the participants were instructed to take meals consisting of an average of 420 kcal of protein, 840 kcal of carbohydrate, and 420 kcal of fat per day (1680 kcal/day). Participants maintained daily food diaries during the 12-week lifestyle modification program and learned about proper daily nutrition (well-balanced intake of protein, carbohydrate, fat, amino acids, vitamins, and minerals) through weekly lectures and counseling by skilled dietitians.
Aerobic exercise training
The participants performed exercise training in the form of walking and jogging for sessions of 40–60 min each (3 days/week) as previously described with minor modifications.8 Briefly, the participants were supervised by 2 or 3 exercise instructors. In the first 2 months, the exercise consisted only of walking, with the target Borg’s scale score ranging from 11 (light) to 13 (fairly hard). The distances walked were 3.5 and 4.5 km in the first and second months, respectively. In the last month, the participants performed a combination of a 3.0-km brisk walk and a 1.0-km medium-intensity jog with the target Borg’s scale score ranging from 13 (fairly hard) to 15 (hard). The participants measured their heart rate using portable heart rate monitors (s610i; Polar Electro OY, Oulu, Finland) while walking and jogging and recorded the duration (in minutes) and intensity (heart rate or Borg’s scale score) during each exercise session. Subjects recorded their actual exercise and additional physical activity in a diary. The daily steps during the 12-week lifestyle modification program were recorded using a uniaxial electrical accelerometer (Lifecorder; Suzuken Co. Ltd., Nagoya, Japan).
Anthropometric measurements
Anthropometric measurements were performed before and after the 12-week lifestyle modification program. Body weight was measured once to the nearest 0.1 kg using a digital scale (WB-150; TANITA, Tokyo, Japan), whereas height was measured once to the nearest 0.1 cm using a wall-mounted stadiometer (YG-200; Yagami, Nagoya, Japan); the participants were barefoot and wearing only underwear during these measurements, which were performed prior to eating in the morning. BMI was calculated as the weight (in kilograms) divided by height (in meters) squared. Waist circumference was measured directly on the skin at the level of the umbilicus in the standing position. The waist circumference measurements were recorded in duplicate to the nearest 0.1 cm.
Serum levels of testosterone and SHBG and blood biochemistry
Each blood sample was placed in a serum separator tube, allowed to clot for 2 h, and then centrifuged at 3000 rpm for 15 min at 4 °C. The serum obtained was stored at −80 °C until the assay was performed. Total testosterone serum concentrations were determined using standard radioimmunoassay procedures, whereas SHBG levels were determined using a commercial enzyme-linked immunosorbent assay kit (Quantikine DSHBG0; R&D Systems Inc., Minneapolis, MN, USA). The SHBG assay was performed according to the manufacturer’s instructions. Serum concentrations of total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, triglycerides, insulin, and homeostasis model of insulin resistance (HOMA-IR) were determined using standard enzymatic techniques. Hemoglobin A1c (HbA1c) levels were measured in whole blood using an immunoturbidimetric latex test immediately after sampling.
V .
Before and after the 12-week lifestyle modification program,
Carotid-femoral PWV
cfPWV was measured using applanation tonometry as previously described with minor modifications.16 Briefly, carotid and femoral arterial pulse waves were obtained in triplicate using arterial applanation tonometry incorporating an array of 15 transducers (form PWV/ABI; Colin Medical Technology, Komaki, Japan). The distance traveled by the pulse waves was assessed in triplicate with a random zero-length measurement over the body surface with a non-elastic tape measure. PWV was calculated by dividing the distance (carotid to femoral artery) by the transit time. The pulse-wave transit time was determined from the time delay between the proximal and distal “foot” waveforms. The foot of the wave was identified as the commencement of the sharp systolic upstroke, which was automatically detected. Thus, cfPWV was calculated as the distance divided by the transit time and was assessed in triplicate.
Blood pressure and heart rate
The resting supine arterial blood pressure and heart rate were determined from each subject’s right arm using an automated device (form PWV/ABI; Colin Medical Technology). We measured arterial blood pressure 3 times, and the mean values were used for the analysis.
Statistical analysis
The data are expressed as mean ± SE. To evaluate the differences in the levels before and after the lifestyle modification program, the Student’s t-test for paired values was used. Analysis of covariance was used to determine the effects of smoking, medication, waist circumference, and the changes in mean blood pressure. Relationships between the percentage changes in non MBP-adjusted cfPWV or serum testosterone concentrations and other factors were analyzed using Pearson’s correlation, partial correlation, and stepwise multivariable linear regression analysis. For stepwise multiple linear regression analysis, the percentage changes in non MBP-adjusted cfPWV were used as dependent variables, whereas the changes in mean blood pressure, heart rate, serum testosterone levels, total cholesterol, LDL cholesterol, triglycerides, insulin, and HbA1c were used as independent variables. Furthermore, to determine whether the effect of testosterone on non MBP-adjusted cfPWV was associated with mean blood pressure, we performed an additional multivariate analysis using the percentage changes in mean blood pressure as the dependent variables, and the percentage changes in the levels of serum testosterone, non MBP-adjusted cfPWV, total cholesterol, LDL cholesterol, triglycerides, insulin, and HbA1c as independent variables. Values of P < 0.05 were considered to be significant.
Result
The characteristics of the overweight and obese men before and after the 12-week lifestyle modification program are shown in Table 1. The body mass, BMI, and waist circumference decreased markedly in overweight and obese men after the 12-week lifestyle modification program. In overweight and obese men, the concentrations of total cholesterol, LDL cholesterol, triglycerides, insulin, HOMA-IR index, and HbA1c significantly decreased after the 12-week program compared to the values before the program. The
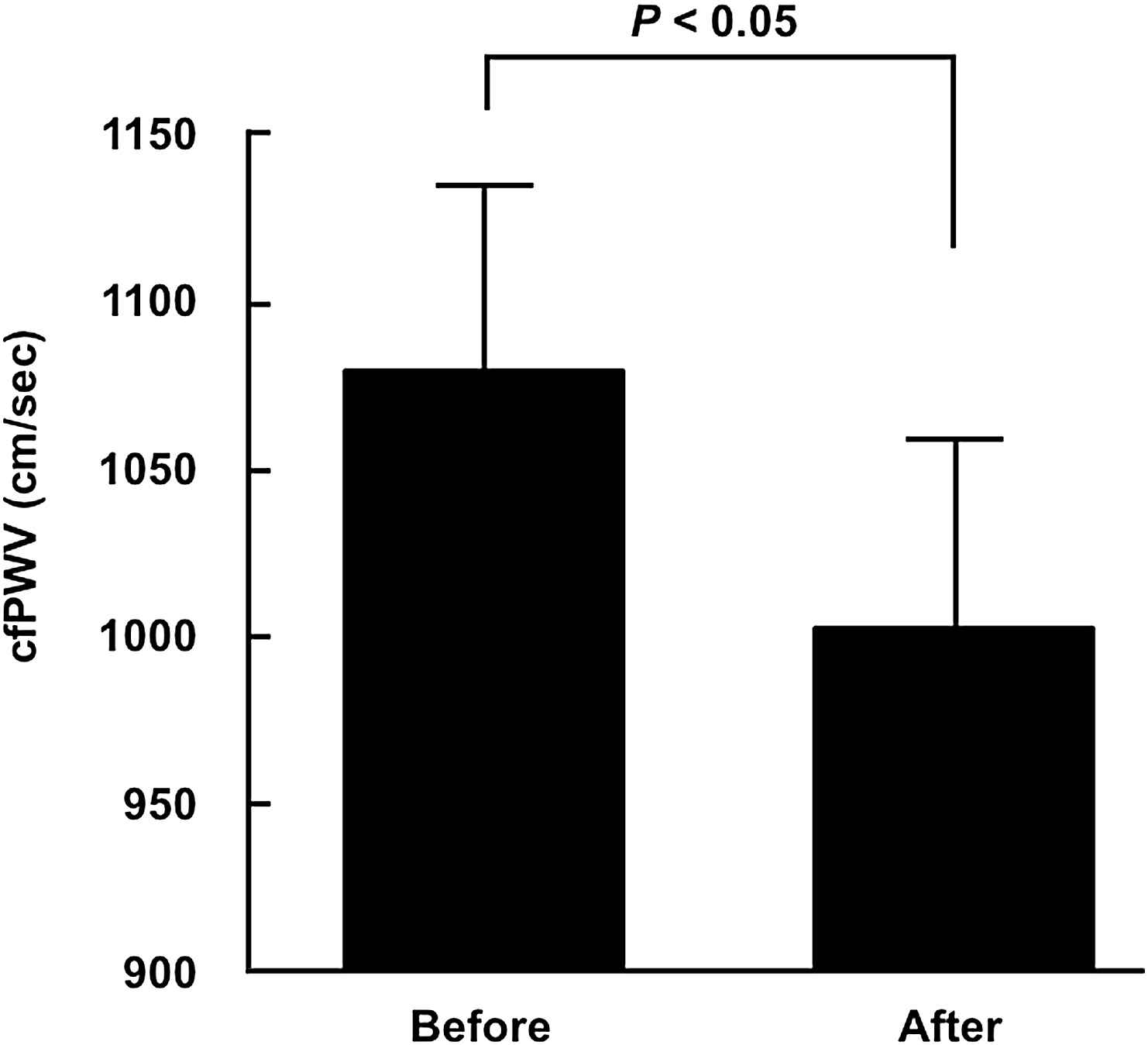
Carotid-femoral pulse wave velocity before and after the 12-week lifestyle modification. Data are expressed as mean ± SE.
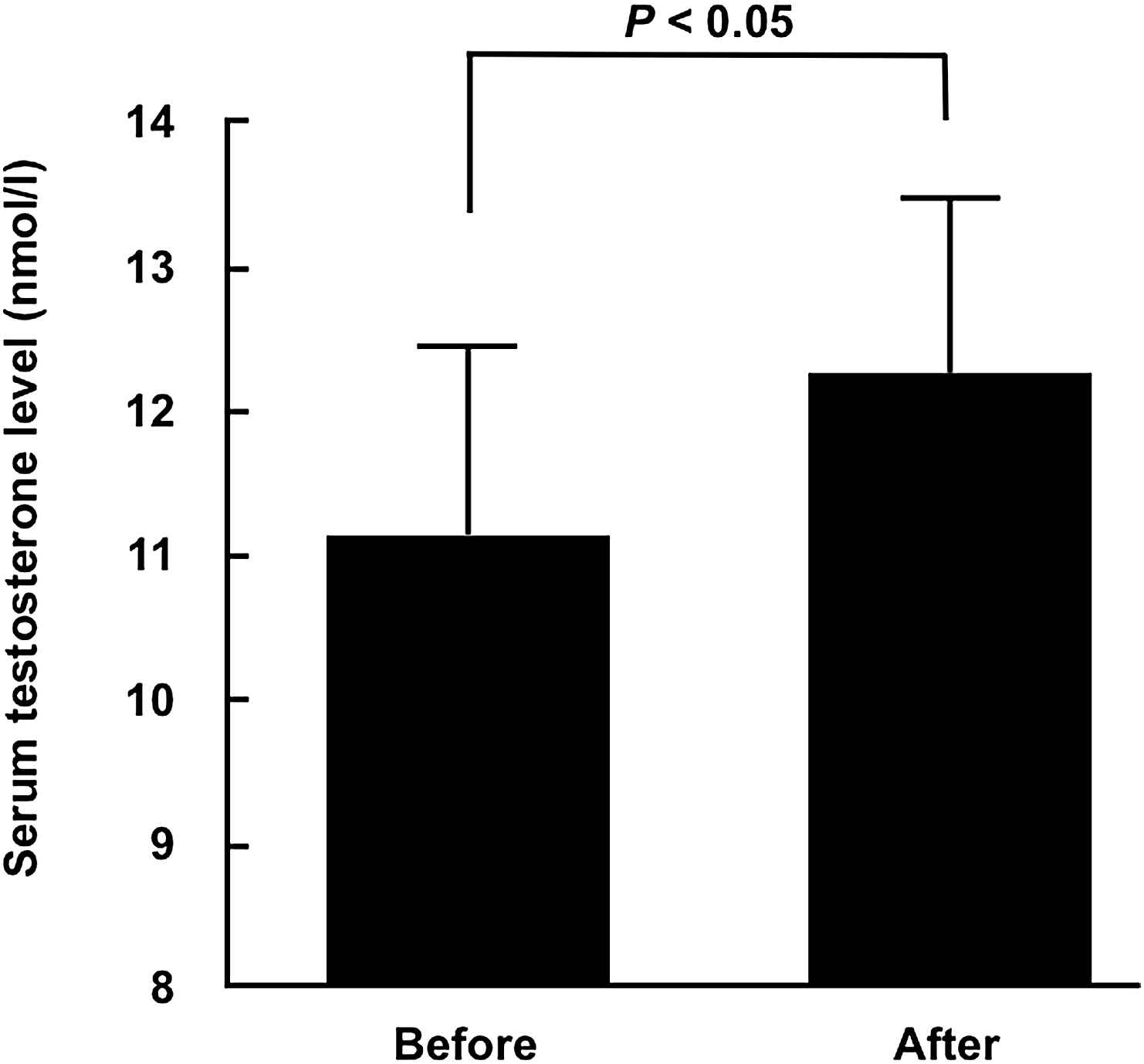
Serum testosterone levels before and after the 12-week lifestyle modification program. Data are expressed as mean ± SE.
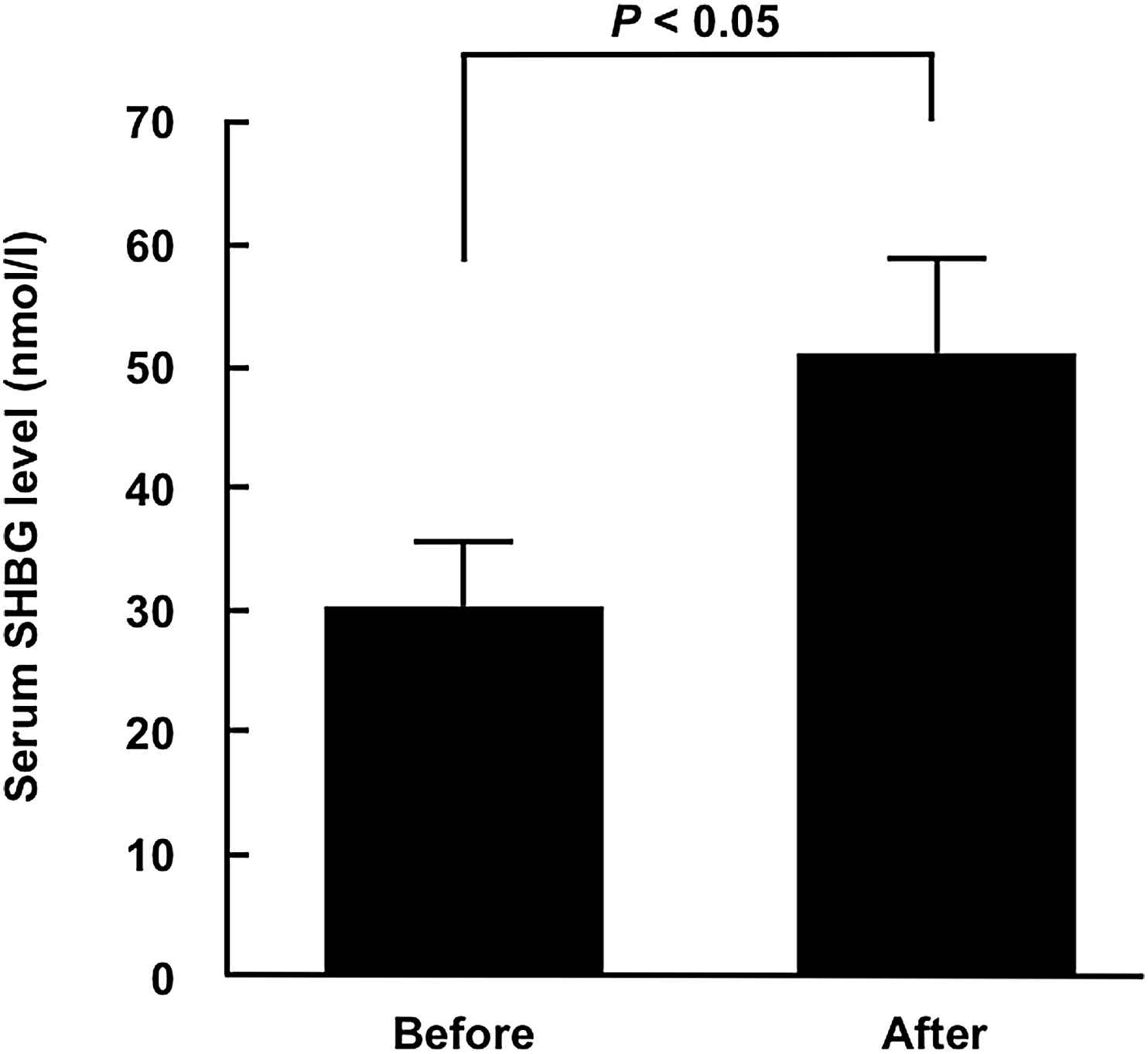
Serum sex hormone binding-globulin levels before and after the 12-week lifestyle modification program. Data are expressed as mean ± SE.

Relationships between the percentage changes in the carotid-femoral pulse wave velocity and serum testosterone levels.
| Before | After | |
|---|---|---|
| Age (years) | 53 ± 3 | – |
| Height (cm) | 171.0 ± 1.1 | – |
| Body mass (kg) | 86.9 ± 3.3 | 75.0 ± 2.5* |
| Body mass index (kg/m2) | 30 ± 1 | 26 ± 1* |
| Waist circumference (cm) | 101 ± 2 | 90 ± 2* |
| Total cholesterol (mg/dL) | 233 ± 13 | 184 ± 10* |
| HDL cholesterol (mg/dL) | 52 ± 4 | 55 ± 3 |
| LDL cholesterol (mg/dL) | 140 ± 12 | 107 ± 9* |
| Triglycerides (mg/dL) | 217 ± 37 | 111 ± 28* |
| Insulin (μU/dl) | 12.8 ± 2.8 | 6.8 ± 1.7* |
| HOMA-IR (IU) | 3.1 ± 0.7 | 1.6 ± 0.4* |
| HbA1c (%) | 6.0 ± 0.2 | 5.7 ± 0.2* |
|
|
16.1 ± 1.1 | 20.4 ± 1.7* |
| Steps (steps/day) | 6154 ± 1029 | 10948 ± 970* |
| Total energy intake (kcal/day) | 2153 ± 119 | 1543 ± 69* |
| Carbohydrate intake (g/day) | 285.5 ± 13.4 | 205.4 ± 7.7* |
| Protein intake (g/day) | 89.8 ± 5.9 | 74.9 ± 3.2* |
| Fat intake (g/day) | 57.0 ± 5.0 | 41.0 ± 4.0* |
HDL: high-density lipoprotein; LDL: low-density lipoprotein;
Data are expressed as mean ± SE. Significant difference VS. before lifestyle modification, *P < 0.05.
Characteristics of overweight and obese men before and after the lifestyle modification.
| Before | After | |
|---|---|---|
| Systolic blood pressure (mm Hg) | 135 ± 5 | 122 ± 3* |
| Diastolic blood pressure (mm Hg) | 87 ± 2 | 78 ± 2* |
| Mean blood pressure (mm Hg) | 105 ± 3 | 94 ± 2* |
| Heart rate (bpm) | 68 ± 3 | 57 ± 2* |
Data are expressed as mean ± SE. Significant difference VS. before lifestyle modification,
P < 0.05.
Hemodynamics of overweight and obese men before and after lifestyle modification.
Discussion
In the present study, we investigated the effect of a 12-week lifestyle modification program on arterial stiffness and serum testosterone levels in overweight and obese men. Our findings showed that cfPWV was significantly decreased and that the serum levels of testosterone and SHBG were significantly increased in overweight and obese men after the program compared to the values before the program. Furthermore, we observed a negative relationship between the changes in non MBP-adjusted cfPWV and serum testosterone levels in overweight and obese men. These results suggest that the 12-week lifestyle modification program increases the testosterone and SHBG levels in overweight and obese men and that these elevations may be involved in the mechanism underlying the lifestyle modification-induced decreases in arterial stiffness.
Several studies have reported that arterial stiffness is greater in obese individuals than in non-obese individuals.5,6 We previously demonstrated that aerobic exercise training or dietary modification decreases arterial stiffness in obese individuals.7,8 However, the mechanism underlying lifestyle modification-induced decreases in arterial stiffness in overweight and obese individuals has not yet been clarified. In the present study, we demonstrated that arterial stiffness significantly decreased and serum testosterone levels increased in overweight and obese men after a combination of dietary modification and aerobic exercise training. Decreases in the serum testosterone levels have been reported to increase arterial stiffness in men, which represents the onset of cardiovascular disease.17 Previous studies have shown that the short-term administration of testosterone to patients with coronary artery disease can induce a relaxing effect on coronary circulation and improve endothelial vasomotor function.18,19 These findings suggested that testosterone is an anti-atherogenic factor. Testosterone is a type of androgen and is primarily produced by the Leydig cells within the testes. The majority of circulating testosterone is bound to transporter proteins. Approximately 60% of circulating testosterone is bound to SHBG with high affinity. SHBG, a glycoprotein produced in the liver, is a known transporter of circulating testosterone. The testosterone–SHBG complex has been reported to trigger blood vessel wall vasodilation.12–14 Moreover, insulin has been reported to have a vasodilation effect similar to nitroglycerin. However, the vasodilation effect of insulin is reportedly impaired by obesity-induced hyperinsulinemia or insulin resistance.20 In the present study, we measured HOMA-IR—an index of insulin resistance—in overweight and obese subjects. Its value was changed from 3.1 IU to 1.6 IU, which represents an improvement following lifestyle modification. Therefore, based on the results of the present study, it may be possible that insulin did not play the role of a vasodilator. Moreover, we noted that lifestyle modification increased the serum levels of testosterone and SHBG in overweight and obese men after the 12-week program. Furthermore, we found a negative relationship between the changes in non MBP-adjusted cfPWV and serum testosterone levels. Thus, these results suggest that the vasodilator function of testosterone may contribute to decreased arterial stiffness in overweight and obese men. However, there may be several related and complicated mechanisms underlying the improvement in blood pressure and cfPWV (such as those involving adiponectin, inflammatory factors, and lipids).21–23
In the present study, we noted that the 12-week lifestyle modification program increased the serum testosterone levels and decreased non MBP-adjusted cfPWV in overweight and obese men. Many previous studies have demonstrated that changes in blood pressure strongly influence arterial stiffness.24–26 In the present study, stepwise multivariable linear regression analysis indicated that decreased non MBP-adjusted cfPWV was positively associated with decreased mean blood pressure (β = 0.835, P < 0.01). Moreover, the changes in mean blood pressure were negatively associated with changes in non MAP-adjusted cfPWV (β = 0.682, P < 0.05) and changes in serum testosterone levels (β = −0.646, P < 0.05) due to lifestyle modifications on stepwise multivariable linear regression analysis. Furthermore, testosterone replacement therapy has been shown to have an anti-hypertensive effect in obese men.27–29 Thus, we suggest that the increased serum testosterone levels induces the lowering of the mean blood pressure, thereby contributing to the decrease in non MBP-adjusted cfPWV.
Serum testosterone levels are lower in obese men than in normal-weight men. Previous studies have investigated the effect of weight reduction by dietary modification on serum testosterone levels in obese men.30,31 One study indicated that serum testosterone levels significantly increased in obese men after the dietary weight-loss intervention,30 whereas another study reported that this did not occur.31 Thus, the effect of weight reduction by dietary modification on serum testosterone levels in obese men is unclear. However, Muller et al. reported in a cross-sectional study that increased physical activity could increase serum testosterone levels in middle-aged and elderly men.9 However, it is not clear whether aerobic exercise training increases serum testosterone levels in obese men. In the present study, we demonstrated that serum testosterone levels significantly increased in overweight and obese men after the 12-week lifestyle modification program. Pasquali et al. reported that decreasing serum insulin levels increased serum testosterone levels in normal-weight and obese men.32 Serum insulin levels are known to decrease after dietary modification or habitual aerobic exercise in obese individuals.33,34 The present study demonstrated that serum insulin levels significantly decreased in overweight and obese men after the lifestyle modification program compared to the levels before the program. Moreover, we observed a significant negative relationship between changes in serum testosterone levels and serum insulin levels in overweight and obese men before and after the lifestyle modification program (r = −0.661, P < 0.05). However, SHBG production has also been reported to decrease with changes in insulin levels.35 Thus, decreases in the serum insulin levels by dietary modification and aerobic exercise training may stimulate an increase in the serum levels of testosterone and SHBG in overweight and obese men.
Dietary habits and physical activity have been reported to affect SHBG production. Selva et al. demonstrated that a high carbohydrate and high protein diet stimulates hepatic lipogenesis and decreases SHBG production.36 However, Tikkane et al. demonstrated in a cross-sectional study that increased physical activity led to elevated serum SHBG concentrations in middle-aged men.37 In the present study, the total carbohydrate and total protein intakes significantly decreased and the number of steps significantly increased in overweight and obese men after the 12-week lifestyle modification program compared to the values before the program. Therefore, we suggest that serum SHBG levels increase with increasing physical activity and dietary modification. Moreover, Ronde et al. reported the presence of a positive relationship between serum SHBG levels and serum testosterone levels in healthy men, and indicated that an increasing serum SHBG level induces an increase in the serum testosterone levels.38 Thus, we suggest that increasing serum SHBG levels induce increasing testosterone levels in overweight and obese men.
In conclusion, the present study showed that the 12-week lifestyle modification program (dietary modification and aerobic exercise training) decreased arterial stiffness and increased serum levels of testosterone and SHBG in overweight and obese men. Furthermore, we demonstrated that the changes in serum testosterone levels before and after the lifestyle modification program in overweight and obese men were negatively correlated with those of arterial stiffness. Although the increase in serum testosterone levels was associated with a corresponding reduction in arterial stiffness, the association appears to be mediated by a change in blood pressure and not a direct, causal link between the two key variables. Clearly, the possibility cannot be excluded that increased testosterone levels may have mediated the reduction in blood pressure. However, this requires further investigation.
Limitations
The lack of an appropriate control/observational group and a small sample size are clear limitations of the present study. Furthermore, there may be more than one mechanism underlying the improvement in blood pressure and cfPWV (such as mechanisms involving adiponectin, inflammatory factors, and lipids). Therefore, further research needs to clarify the mechanisms underlying the decrease in cfPWV in overweight and obese men.
Conflict of interest
We have no financial, consultant, institutional or other relationships that might lead to bias or a conflict of interest.
Acknowledgments
This work was supported by Grants-in-Aid for Scientific Research (
References
Cite this article
TY - JOUR AU - Hiroshi Kumagai AU - Asako Miyaki AU - Ryota Higashino AU - Nobuhiko Akazawa AU - Youngju Choi AU - Song-Gyu Ra AU - Miki Eto AU - Kiyoji Tanaka AU - Ryuichi Ajisaka AU - Seiji Maeda PY - 2014 DA - 2014/05/09 TI - Lifestyle modification-induced increase in serum testosterone and SHBG decreases arterial stiffness in overweight and obese men JO - Artery Research SP - 80 EP - 87 VL - 8 IS - 3 SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2014.04.003 DO - 10.1016/j.artres.2014.04.003 ID - Kumagai2014 ER -