
Association between worldwide dietary and lifestyle patterns with total cholesterol concentrations and DALYs for infectious and cardiovascular diseases: An ecological analysis
- DOI
- 10.1016/j.jegh.2015.02.002How to use a DOI?
- Keywords
- Obesity; High cholesterol; Food balance sheets; Physical inactivity; Ecological analysis
- Abstract
Global dietary and lifestyle trends are primary risk factors for communicable and non-communicable diseases. An ecological analysis was conducted to examine the association of global dietary and lifestyle patterns with total cholesterol concentrations. This study also investigated whether total cholesterol modified the association between dietary and lifestyle habits with disability-adjusted-life-years-lost (DALYs) for infectious and cardiovascular diseases (CVDs). Country-specific mean total cholesterol concentrations and DALYs for infectious and CVDs were obtained. Data were then matched to country-specific food and energy availability for consumption and information on obesity, physical inactivity, urbanization, gross domestic product (GDP), life expectancy and smoking. Stepwise multiple regression models were developed to identify significant predictors of total cholesterol concentrations and DALYs for infectious and CVDs.
Life expectancy and egg and meat consumption were significantly associated with cholesterol concentrations. DALYs for infectious diseases were associated with smoking, life expectancy and per capita GDP. Smoking was the only predictor of DALYs for CVDs. The improvement of socio-demographic conditions and economic growth is likely to reduce the burden of communicable diseases in developing countries. A concurring increase in non-communicable diseases is expected, and these results have, yet again, identified smoking as a primary risk factor for CVDs.
- Copyright
- © 2015 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Cardiovascular diseases (CVDs) are one of the leading causes of worldwide disability and mortality [1]. Several risk factors are involved in the pathogenesis of CVDs which can be simply distinguished by non-modifiable (age, gender, genotype) and modifiable (dietary intake, smoking, stress, weight gain, sedentarism) [2]. Dietary cholesterol is an example of a modifiable risk factor for CVDs since elevated cholesterol concentrations have been linked to the development of endothelial dysfunction and atherosclerosis [3,4]. Reducing high blood cholesterol is thus important for CVD prevention. Statins – cholesterol lowering drugs – reduce cardiovascular events in people with a past history of CVD, as well as in otherwise healthy individuals at high risk for CVD.
In the Seven Countries Study, Keys and colleagues [5] observed a significant association of dietary fat intake, plasma cholesterol levels and the incidence of coronary heart disease (CHD). In addition, a recent analysis of the 40-year mortality follow-up data has shown a substantial homogeneity, across different countries, in the relationship between cholesterol concentrations and the risk of fatal CHD despite large between-country differences in absolute risk. This means that for a given change in serum cholesterol concentrations, each country would experience a similar increase in the relative risk for CHD mortality [6]. A meta-analysis of individual data from the Prospective Studies Collaboration reported a positive association between total cholesterol concentrations and CHD mortality in middle-aged and older subjects [7]. The evidence is, however, conflicting and more recent data have challenged the role of hypercholesterolemia as a disease risk factor, particularly in older aged individuals [8]. In addition, preliminary laboratory and epidemiological findings have suggested a role of cholesterol in the regulation of immune function and reported the association of high cholesterol levels with a lower risk of infections [9].
The prevalence of hypercholesterolemia in developed countries has overall stabilized or declined in the last 20 years, whereas a gradual increase has been observed in less affluent countries undergoing demographic, social and economic transitions [10]. These phenomena have been conceptualized within the nutrition transition model, which attempts to identify the main socio-economic, lifestyle and dietary factors linked to dynamic shifts of the global burden of communicable and non-communicable diseases [11]. The model essentially describes how the progressive improvement of social and economic welfare reduces the burden of communicable diseases on the one hand and increases the risk for non-communicable diseases on the other hand by the adoption of Westernized sedentary lifestyle and dietary patterns [12]. Raised cholesterol concentrations are generally one of the first signs of these lifestyle changes and mostly related to a greater consumption of food rich in saturated fat such as red meat, cheese or butter [13].
The primary aim of this study is to conduct an ecological analysis to identify worldwide dietary and lifestyle factors associated with total cholesterol concentrations obtained from 163 individual world nations. A cluster analysis was also conducted to identify typical dietary patterns of global food availability for consumption and to test whether they were linked to cholesterol concentrations. The impact of cholesterol concentrations on global health was evaluated by examining whether dietary patterns, lifestyle factors and blood cholesterol concentrations were independently associated with estimates of disability-adjusted life years lost (DALYs) for infectious diseases and CVDs. This would help to understand if cholesterol levels play a role in modifying the association between dietary and socio-demographic ecological variables and DALYs for infectious diseases and CVDS.
2. Methods
A search for the most recent information on prevalence rates reported for each country was conducted using the World Health Organisation (WHO) Global InfoBase database. Year- and country-specific food balance sheets (FBS), urbanization, physical inactivity and smoking rates, obesity prevalence, life expectancy and per capita GDP estimates were retrieved. The project was undertaken between January and September 2013.
2.1. Mean cholesterol plasma levels
Data on total mean cholesterol levels (mmol/L) were obtained from the WHO Global InfoBase database (web link: https://apps.who.int/infobase/Indicators.aspx) and specifically utilizing the 2010 WHO Global Comparable Estimates. The estimates are based on aggregated data provided by countries to the WHO and obtained through a review of published and unpublished literature. A detailed description of the methods used to obtain the estimates is provided in the 2010 WHO Global status report on non-communicable diseases [13].
2.2. Disability-adjusted life years lost (DALYs)
The disability-adjusted life year (DALY) is a measure of overall disease burden, expressed as the number of years lost due to ill-health, disability or early death. Health burden has been expressed as Years of Life Lost (YLL), but this measure does not account for the impact of disability (Years Lived with Disability [YLD]). DALYs are derived as the sum of these two components (DALY = YLL + YLD) indicating that the burden associated with a specific chronic illness is both dependent on time lost due to premature death and time spent disabled by disease. One DALY, therefore, is equal to one year of healthy life lost. The WHO database (web link: http://www.who.int/healthinfo/global_burden_disease/estimates_country/en) was accessed to obtain data on the 2004 estimated DALYs per 100,000 population for infectious and parasitic diseases and CVDs.
2.3. Food availability for consumption
The FAOSTAT database (web link: http://faostat.fao.org/site/368/default.aspx#ancor) developed by the Food and Agriculture Organization (FAO) was accessed to obtain data on food availability consumption for the year 2010. Food balance sheets were used to extract information on energy availability for consumption from a selected list of commodities. A schematic representation of the classification of the food products used in the analysis is provided in the Online Supplementary Material (Fig. S1).
2.4. Smoking
Current smoking prevalence of any tobacco product (crude rate for cigarettes, cigars, pipes and any other form of smoked tobacco) for each country (individuals aged 15 years and above) was extracted from the Global Health Observatory Data Repository.
2.5. Life expectancy
Data were obtained from the WHO Global Health Observatory Data Repository database. Life expectancy at birth reflects the overall mortality level of a population, and it summarizes the mortality pattern that prevails across all age groups in a given year.
2.6. Physical inactivity
Data were extracted from the WHO Global Health Observatory Data Repository database. Physical inactivity was defined as not meeting any of the following criteria: (1) at least 30 min of moderate-intensity activity per day on at least 5 days per week; (2) at least 20 min of vigorous-intensity activity per day on at least 3 days per week; or (3) an equivalent combination.
2.7. Per capita gross domestic product (GDP)
The World Bank database (web link: http://data.worldbank.org/indicator/NY.GDP.PCAP.CD) was utilized to obtain the year-specific per capita GDP (in U.S. dollars) for each country. Per capita GDP is gross domestic product divided by midyear population. It was used to categorize countries in low (<$1000), lower middle ($1000–$3999), upper middle ($4000–$11,999) and high income (⩾$12,000) groups.
2.8. Urbanization
The percent urbanization of each country was obtained from the United Nations Population Division database (web link: http://apps.who.int/gho/data/#). Urbanization was defined as the percent of population living in urban areas.
2.9. Literacy
Literacy rates were extracted from the World Bank Database (web link: http://data.worldbank.org/indicator/SE.ADT.LITR.ZS) and taken as a percentage of people aged 15 and above who are characterized as literate.
2.10. Statistical analyses
Variables were checked for normality distribution (Q–Q plots), and appropriate transformations were applied to correct for skewness. Pearson’s correlation analysis was used to evaluate the associations between independent (food availability for consumption, socio-demographic, lifestyle factors) and dependent variables (total cholesterol concentrations). Stepwise multiple linear regression was performed to identify dietary, lifestyle and socio-demographic predictors of total cholesterol concentrations and DALYs for infection and CVDs (dependent variables). Independent variables entered into the model were: total energy available for consumption (kcal), percent energy availability from each food group considered, smoking, obesity prevalence, life expectancy, literacy, urbanization, per capita GDP, and physical inactivity. Cholesterol concentration was added to the models to predict DALYs for infections and CVDs.
A hierarchical cluster analysis was performed first to identify the number of clusters describing the dietary data using the Ward’s method. The number of clusters was evaluated by inspection of the dendrogram and agglomeration coefficients. A k-means cluster analysis was then performed to identify the characteristic dietary patterns of each cluster. Analyses identified three clusters characterized by a similar total energy intake and food availability for consumption for each food commodity (Table S1, Online Supplementary Material). Differences in food availability for consumption between countries stratified by dietary clusters were evaluated using the ANOVA method. Post-hoc analysis (Fisher’s Least Significant Difference) was conducted to assess differences between the individual clusters. Analyses were undertaken using Excel 2007 for Windows and SPSS 17 for Windows. Statistical significance was set at p < 0.05.
3. Results
3.1. Main characteristics
163 countries were eligible for inclusion in the final database. A list of the countries included in the analysis is provided in the Online Supplementary Material. Global total cholesterol concentrations ranged from 3.3 mmol/L to 6.1 mmol/L. The African region had the lowest total cholesterol concentrations (4.4 mmol/L), and the highest values were observed in Australia and the Pacific Islands (5.4 mmol/L).
3.2. Correlation
Total cholesterol concentrations showed a significant association with all food commodities, except for alcohol consumption. The association was stronger with meat (r = 0.62, p < 0.001) and egg (r = 0.62, p < 0.001) consumption and with life-expectancy (r = 0.69, p < 0.001) and per capita GDP (r = 0.61, p < 0.001) (Table 1). Similarly, DALYs for infectious diseases showed a significant association with almost all dietary, socio-demographic and lifestyle variables. Improvement of financial security and assimilation of Westernized dietary and lifestyle patterns seemed to be inversely associated with DALY’s for infectious diseases.
| Dietary and socio-demographic variables | Mean cholesterol concentrations (mmol/L) | DALYs infectious diseases | DALYs cardiovascular diseases |
|---|---|---|---|
| Total energy available for consumption (kcal) | 0.42*** | −0.79*** | 0.16* |
| Percent energy availability for consumption (%) | |||
| Cereals, excluding beer | −0.42*** | 0.55*** | −0.01 |
| Starchy | −.30*** | 0.46*** | −0.02 |
| Sugar and Sweeteners and Honey | 0.51*** | −0.50*** | 0.01 |
| Vegetables, Total | 0.28*** | −0.47*** | 0.27** |
| Fruits, excluding wine | 0.09 | −0.10 | −0.18* |
| Pulses | −0.33*** | 0.42*** | −0.12 |
| Vegetable oils | 0.06 | −0.29*** | 0.01 |
| Animal fat | 0.52*** | −0.72*** | 0.28** |
| Meat, total | 0.62*** | −0.65*** | 0.11 |
| Fish, seafood | 0.27*** | −0.29*** | −0.04 |
| Milk | 0.39*** | −0.64*** | 0.23** |
| Eggs | 0.62*** | −0.77*** | 0.18* |
| Alcoholic beverages | 0.34*** | −0.44*** | 0.16* |
| Socio-Demographic Factors | |||
| Life expectancy (years) | 0.69*** | −0.90*** | 0.09 |
| Obesity (%) | 0.52*** | −0.57*** | 0.06 |
| Per capita GDP ($) | 0.61*** | −0.85*** | 0.03 |
| Urbanization (%) | 0.40*** | −0.63*** | −0.08 |
| Smoking (%) | 0.33*** | −0.48*** | 0.34*** |
| Physical inactivity (%) | 0.33*** | −0.41*** | −0.12 |
| Literacy (%) | 0.68*** | −0.74*** | 0.37*** |
| DALYs | |||
| Infectious diseases | −0.65*** | – | – |
| Cardiovascular diseases | 0.15* | −0.19*** | – |
Pearson’s coefficients of correlation are reported.
Variables have been transformed before being entered in the analyses if they were not normally distributed.
p < 0.05.
p < 0.01.
p < 0.001.
Correlation analysis between total cholesterol concentrations (mmol/L) and disability-adjusted life years lost (DALYs) for infectious and cardiovascular diseases with socio-demographic, lifestyle factors and percent energy available for consumption from individual food commodities (Number of countries 163).
DALYs for CVDs was directly associated with total energy for consumption (r = 0.16, p < 0.05), animal fat (r = 0.28, p < 0.01), milk (r = 0.23, p < 0.01), eggs (r = 0.18, p < 0.05), alcoholic beverages (r = 0.16, p < 0.05) and smoking (r = 0.34, p < 0.001). The significant association of DALYs for CVDs with vegetable consumption (r = 0.27, p < 0.01) was surprising, whereas the expected, inverse association with fruit consumption (r = −0.18, p < 0.05) was observed (Table 1).
3.3. Stepwise multiple regression
The regression models including only food commodities as independent variables (Model 1) showed that cholesterol concentrations were associated with energy availability for consumption from eggs, meat and total sugar (Table 2). In fully adjusted models (Model 2), life expectancy and eggs and meat energy availability for consumption were significant predictors of total cholesterol concentrations. DALYs for infectious diseases were associated with animal fat consumption, smoking, life expectancy and per capita GDP. Smoking was the only predictor of DALYs for CVDs (Table 3).
| Mean cholesterol concentrations (mmol/L) | ||
|---|---|---|
| B ± SE | p | |
| Model 1 (dietary variables) | ||
| N | 161 | |
| R2 | 0.51 | |
| Energy availability for consumption from eggs (%) | 1.55 ± 0.33 | <0.001 |
| Energy availability for consumption from meat (%) | 1.75 ± 0.41 | <0.001 |
| Energy availability for consumption from total sugar (%) | 0.23 ± 0.07 | 0.002 |
| Energy availability for consumption from fruits (%) | – | – |
| Model 2 (model 1 + Socio-demographic and lifestyle variables) | ||
| N* | 93 | |
| R2 | 0.49 | |
| Energy availability for consumption from eggs (%) | 2.31 ± 0.55 | <0.001 |
| Energy availability for consumption of meat products (%) | 1.86 ± 0.55 | <0.001 |
| Life expectancy (years) | 10.98 ± 3.27 | 0.001 |
Results are shown for significant variables. Independent variables entered into Model 1 were: total energy available for consumption (kcal), percent energy availability from cereals, fruit, total vegetables, all sugar, vegetable oils, starchy roots, pulses, alcoholic beverages, meat total, animal fat, eggs, milk, fish and seafood. Model 2: Model 1 + smoking, life expectancy, obesity prevalence, literacy, urbanization, per capita gross domestic product (GDP) and prevalence of physical inactivity. B = unadjusted regression coefficient; SE, standard error; R2 = explained variance; N = number of countries. Variables were transformed to fit linearity assumptions of the regression models.
Missing data of smoking and physical inactivity data determined the lower number of cases.
Stepwise multiple linear regression to identify dietary, lifestyle and socio-demographic predictors of total cholesterol concentrations.
| Model | DALYs infectious diseases | DALYs cardiovascular diseases | ||
|---|---|---|---|---|
| B ± SE | p | B ± SE | p | |
| N* | 93 | 93 | ||
| R2 | 0.87 | 0.42 | ||
| Life expectancy (years) | −5.84 ± 0.75 | <0.001 | – | – |
| Smoking prevalence (%) | −0.40 ± 0.09 | <0.001 | 0.34 ± 0.05 | <0.001 |
| Per capita GDP ($) | −0.44 ± 0.08 | <0.001 | – | – |
Results are shown for significant variables. Independent variables entered into Model 1 were: total energy available for consumption (kcal), percent energy availability from cereals, fruit, total vegetables, all sugar, vegetable oils, starchy roots, pulses, alcoholic beverages, meat total, animal fat, eggs, milk, fish and seafood. Model 2: Model 1 + smoking, life expectancy, obesity prevalence, cholesterol concentrations, literacy, urbanization, per capita gross domestic product (GDP) and prevalence of physical inactivity. B = unadjusted regression coefficient; SE, standard error; R2 = explained variance; N = number of countries. Variables were transformed to fit linearity assumptions of the regression models.
Missing data of smoking and physical inactivity data determined the lower number of cases.
Stepwise multiple linear regression to identify dietary, lifestyle and socio-demographic predictors of disability-adjusted life years lost (DALYs) for infectious and cardiovascular diseases.
3.4. Dietary patterns
The cluster analyses identified three dietary patterns, which were characterized by a different consumption of energy and food products. These patterns were named as: agricultural, transitional and Westernized (Table S1). The agricultural pattern was characterized by a higher consumption of cereals, starchy food and pulses and lower energy intake. The transitional and Westernized patterns showed a similar consumption of sugar, fruits, vegetables and eggs. However, the transitional pattern showed greater energy intake and consumption of vegetable oils, meat, alcoholic beverages, animal fat and milk and a lower consumption of cereals and starchy food compared with the Westernized pattern (Fig. S3). A progressive increase in physical inactivity, urbanization and per capita GDP was observed as countries moved from the agricultural to the Westernized dietary pattern (Fig. 1). The agricultural pattern was associated with lower cholesterol concentrations and prevalence of obesity, whereas no difference was observed between the transitional and Westernized patterns (Fig. 2A and B). The three dietary clusters showed no difference for DALYs for CVDs (p = 0.13, Fig. 2C), whereas a significant decline in DALYs for infectious diseases (p < 0.001, Fig. 2D) was observed as countries moved from the agricultural to the Westernized dietary pattern.
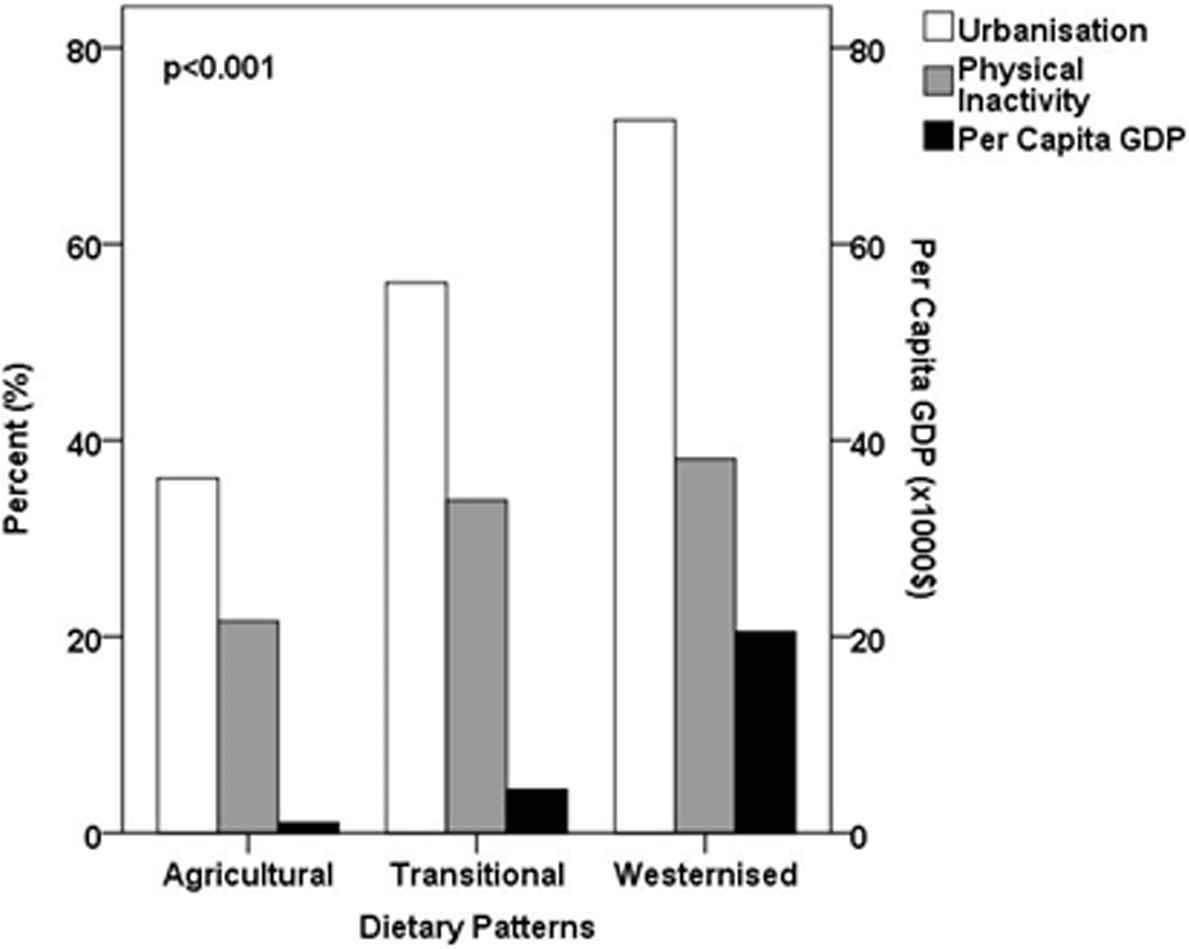
Association of dietary patterns with urbanization, physical inactivity prevalence (%) and per capita gross domestic product (GDP). Dietary patterns were identified using k-means cluster analysis. A description of cluster analysis is provided in the methods section. GDP values were divided by a fixed factor (1000) to allow comparison with the other two groups. Urbanization, physical inactivity prevalence and per capita GDP were all statistically different (p < 0.001) between the three dietary patterns. Univariate analysis of variance (ANOVA) was used and variables were transformed if not normally distributed.
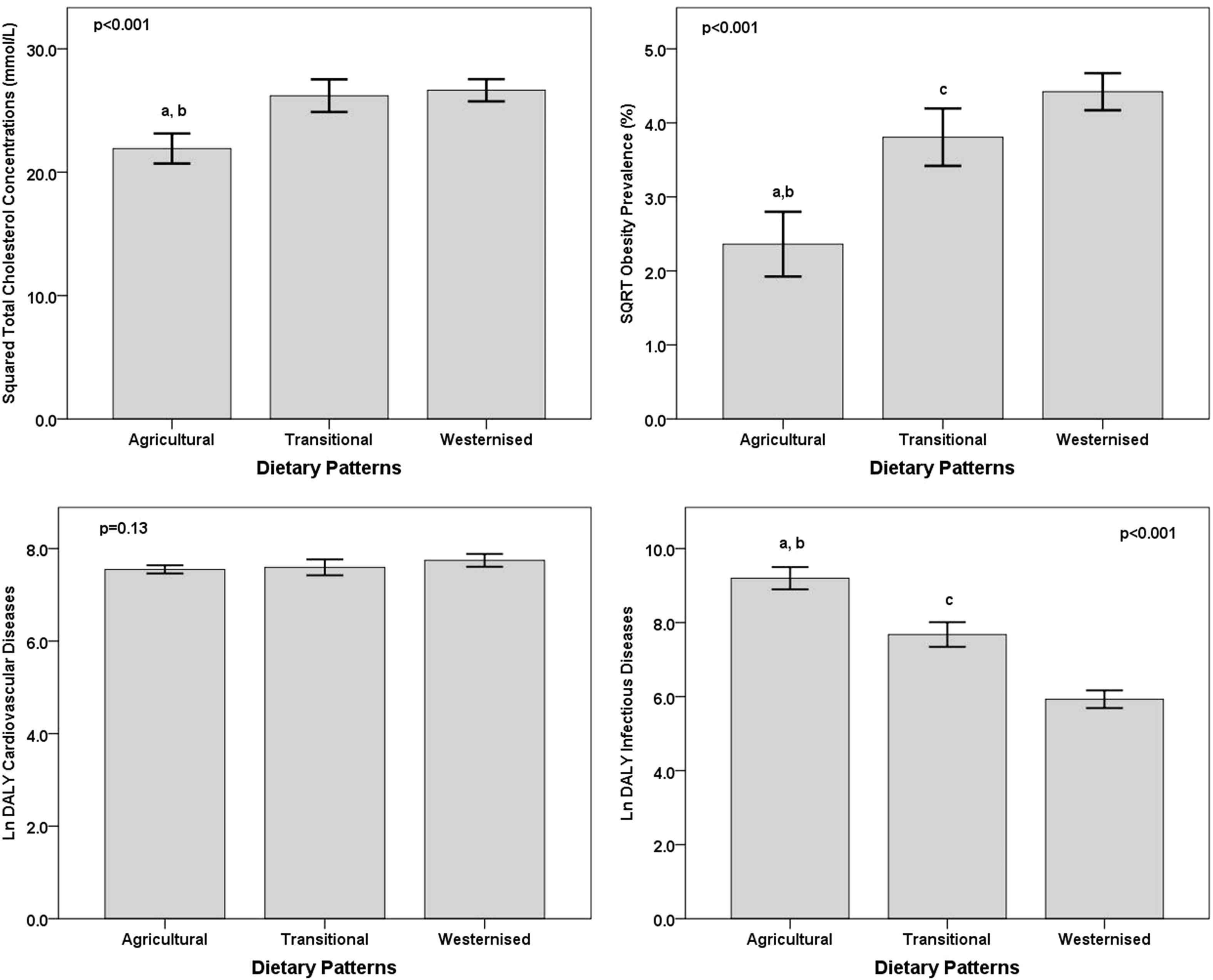
Association of dietary patterns with cholesterol concentrations, obesity prevalence and disability-adjusted life years lost (DALYs) for infectious and cardiovascular diseases. Dietary patterns were identified using k-means cluster analysis. A description of cluster analysis is provided in the methods section. Univariate analysis of variance (ANOVA) was used and post-hoc analysis (Fisher’s LSD method) was conducted to detect differences between dietary patterns. Post-hoc analysis (p < 0.05): a = agricultural vs. transitional; b = agricultural vs. Westernized; c = transitional vs. Westernized. Mean ± 95%CI.
4. Discussion
4.1. Summary of main findings
The cluster analysis on worldwide consumption of food commodities identified characteristic dietary patterns (agricultural, transitional and Westernized) associated with circulating cholesterol concentrations [11,14,15]. Life expectancy at birth and meat and egg energy availability for consumption were significantly associated with circulating total cholesterol concentrations in a fully-adjusted model for socio-demographic, dietary and lifestyle factors. The role of cholesterol in determining the worldwide disease burden for infectious and CVDs was not significant. Conversely, DALYs for infectious diseases were explained by factors typically associated with an epidemiological transition such as per capita GDP, life expectancy and smoking. Smoking was the only variable significantly associated with global DALYs for CVDs. The dichotomous effect of nutritional and epidemiological transitional patterns of DALYs for infectious and CVDs was evident in the contrasting association with the three dietary patterns identified in this manuscript. Not surprisingly, the prosperity of the countries and consequent adoption of more Westernized dietary habits reduced both mortality and disability associated with infectious diseases. A slightly unexpected result was instead seen for DALYs of CVDs as no association was observed with the three dietary patterns, as the burden of disease remained essentially unchanged across the three dietary patterns.
4.2. Determinants of global cholesterol concentrations
The link between egg consumption and cholesterol levels is not unexpected as the cholesterol content of eggs is generally elevated and previous studies have shown a direct relationship between egg consumption and cholesterol levels in humans [16]. However, the association between egg consumption and cholesterol in this study may simply reflect the utilization of eggs for the preparation of other food products such as biscuits, cakes and pastries, as well as oils and animal products rich in saturated fat used for cooking the eggs. Egg consumption could therefore represent at the ecological level a surrogate dietary measure for food consumption of products rich in saturated fat and associated with the stages of nutrition transition. In addition, recent findings from prospective cohort studies do not support a role of egg consumption as a risk factor for CVDs [17]. The epidemiological literature, as well as the clinical trial evidence, does not support the idea that dietary cholesterol, and in particular egg consumption, is a risk factor for CHD or stroke in healthy adults [18], contrary to what has been observed in subjects with chronic degenerative diseases like type 2 diabetes, especially if elderly [19]. The contrasting results may be linked to the multi-factorial association between dietary cholesterol and pathogenesis of CHD, as this is influenced by genetic, lifestyle and dietary factors [20,21]. More specifically, the weak relationship of CHD and dietary cholesterol from egg consumption might be modulated by the intake of other nutrients present in eggs such as antioxidants, mainly beta-carotenoids and Vitamin E, with potential, beneficial effects of atherosclerotic plaque formation and progression [20]. The same can be said for the association between the consumption of meat products and cholesterol levels. Consumption of processed meats is associated with a higher incidence of CHD, stroke and diabetes mellitus [22,23], and studies both in developed and developing countries have shown a significant association between meat intake and total cholesterol concentrations [24,25]. However, the analyses that were performed in this study have not distinguished between the consumption of lean, white or processed meat, or the trends in consumption of meat that vary widely around the world, or between populations in different world regions and in sub-population groups within each country. In addition, a moderate intake of lean red meat within the context of a balanced diet is generally seen as having beneficial effects on cardio-metabolic health [26,27]. It is therefore suggested that researchers cautiously interpret these results and take into account the ecological study design and the limited specificity in the assessment of meat intake from the utilization of food balance sheets.
Life expectancy at age zero was the second strong predictor for circulating cholesterol concentrations. This observation may be derived from the direct association between ageing and cholesterol levels, as well as from the greater life expectancy of individuals living in Westernized societies with dietary patterns higher in saturated fat and cholesterol intake. This association was observed in the present analyses as total cholesterol concentrations were greater in the transitional and Westernized dietary patterns. In addition, a non-linear association of total cholesterol concentrations was observed as a steeper association with both obesity and physical inactivity prevalence in low-income countries (Fig. S4). This means that a greater rise in cholesterol concentrations may be expected in developing countries as a result of the escalating worldwide trends of obesity and physical inactivity. The plateau reached in wealthier countries might suggest a greater investment in prevention policies for the prevention of non-communicable diseases [28–30]. In the specific case of hypercholesterolemia, these actions may include the wider use of hypo-lipidemic drugs for the primary and secondary prevention of CVDs [31,32]. The plateau may also be explained by putative physiological mechanisms controlling cholesterol metabolism in individuals with excess adiposity to the extent that the increased “transmigration of fatty acids” and their deposition in other organs may curb the increase in plasma cholesterol.
4.3. DALYs for infectious diseases
The health impact of infectious diseases has decreased in the last two decades passing from approximately 30% in 1990 to 20% of the total of the estimated DALYs in 2010 [33]. However, infectious diseases have continued to have a significant impact on global public health burden, particularly in deprived and underdeveloped areas of the world. In addition, epidemiological and nutritional trends have rapidly shifted the public health significance of infectious diseases as these countries are facing the double burden of disease as non-communicable diseases and injuries have become the major causes of disability and death [34]. The present analyses have clearly demonstrated the significant association between dietary and socio-demographic indicators of wealth and Westernized dietary and lifestyle habits with DALYs of infectious diseases. The results highlight once again how developing countries are facing the double-burden of both communicable and non-communicable diseases which, if not addressed immediately and effectively through concerted local and global public health actions, will have a profound impact on the economic and social development of the populations affected.
4.4. DALYs for cardiovascular diseases
CVDs contribute to approximately 30% of global total mortality and approximately 80% of these deaths occur in developing countries [35]. However, survivors of major cardiovascular events, such as myocardial infarction or stroke, are frequently characterized by severe disability, which contributes to the impact of both mortality and disability on the global significance of DALYs for CVDs [35]. A primary finding of the present analysis is the relative stability of DALYs for CVDs across the three dietary patterns which seems to suggest that DALYs estimates of developing nations are mostly affected by years lost of a healthy life as a consequence of premature death, whereas years lost in developed countries are mostly derived from survival of CVDs events and occurrence of severe disability alongside a greater longevity of individuals.
A primary finding of the present analysis is the identification of smoking as the single predictor of DALYs for CVDs. Anti-smoking campaigns have been effective in reducing tobacco consumption in developed countries, but this has been globally counterbalanced by more persuasive, targeted promotion advertisement of tobacco in developing countries such as it has been predicted that developing countries contribute to approximately 70% of the world’s tobacco consumption [36]. Smoking, together with physical inactivity and dietary factors, is a modifiable behavioural risk factor strongly linked to the development of CVDs. Smoking-related total mortality is projected to double over the next 2 decades in developing nations which calls for urgent, concerted anti-smoking campaigns at the global and local public health levels to minimize the impact on CVDs as well as on other chronic diseases such as cancer and respiratory disorders [13]. A recent authoritative report of the causes of CVD mortality has identified smoking cessation as a cornerstone for CVD prevention, together with increased physical activity and dietary changes [37]. Mortality models have shown that more than half of the decline in CVD mortality may be explained by reductions in modifiable risk factors such as primarily smoking, cholesterol and blood pressure [37].
4.5. Study limitations
A number of limitations are linked to the ecological design of this study. Data collection was from a large scale; therefore, individual energy and food intake may not be fully representative along with actual food consumption. Food consumption and socio-demographic and lifestyle trends are described at the national level and, therefore, differences may exist within subgroups of the population in each country. The way in which food availability for consumption is calculated does not account for waste, food loss or food fed to animals. Obesity cut-off points were also the same for each country; however, this may not be accurate for certain regions, such as Asia, due to ethnic differences reported in body mass index (BMI). Data size may also vary from one country to another which could have potentially affected the results. Life expectancy at birth was used as an indirect measure of ageing. However, this measure may be affected by infant mortality and therefore the results should be interpreted with caution. Ecological studies are generally used as the initial step of epidemiology, assessing disease prevalence amongst many populations [38]. Therefore, ecological associations concerning risk factors require confirmation using longitudinal studies and interventions. Total cholesterol concentrations may not be sensitive in determining CVD risk and more detailed information on lipid profiles (high and low lipoprotein concentrations) may represent more sensitive biomarkers for the prediction of CVD risk.
5. Conclusions
This paper has identified dietary and lifestyle factors contributing to mean blood cholesterol concentrations with the scope to ascertain potential factors that may explain the global rise in CVDs, particularly in developing countries. The role of cholesterol as a primary determinant of global trends in DALYs for CVDs has not been confirmed in these results which is aligned to more recent evidence on the lack of predictive value of dietary cholesterol and saturated fats for CVD risk. However, these results need to be interpreted with caution in trying not to dismiss the relevance of dietary and lifestyle factors as contributors to the global epidemic of non-communicable diseases, but analyses have pointed strongly at smoking as a critical determinant of CVD disability and mortality. These results should serve as a promoter to support stronger and more effective anti-smoking campaigns incorporated within local and global public health policies to prevent the projected rise in non-communicable diseases.
Conflict of interest
None to declare.
Statement of authorship
CO, MS and JCW wrote the manuscript. MS analysed the data. All authors contributed to the critical revision of the manuscript.
Funding sources
None.
Acknowledgements
None.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, in the online version, at http://dx.doi.org/10.1016/j.jegh.2015.02.002.
References
Cite this article
TY - JOUR AU - C. Oggioni AU - H. Cena AU - J.C.K. Wells AU - J. Lara AU - C. Celis-Morales AU - M. Siervo PY - 2015 DA - 2015/03/05 TI - Association between worldwide dietary and lifestyle patterns with total cholesterol concentrations and DALYs for infectious and cardiovascular diseases: An ecological analysis JO - Journal of Epidemiology and Global Health SP - 315 EP - 325 VL - 5 IS - 4 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2015.02.002 DO - 10.1016/j.jegh.2015.02.002 ID - Oggioni2015 ER -