
Measurement of Instantaneous Wave-free Ratio through a Diagnostic Catheter: Comparison of the Results between 4Fr and 5Fr
 , Ryota Uemura1, 4, Yoshiyuki Saiki1, 5, Tatsuo Haraki1, Takeshi Lee2
, Ryota Uemura1, 4, Yoshiyuki Saiki1, 5, Tatsuo Haraki1, Takeshi Lee2- DOI
- 10.2991/artres.k.200620.001How to use a DOI?
- Keywords
- Instantaneous wave-free ratio; pressure study; reliability; diagnostic catheter
- Abstract
Background: Clinical evidence of coronary pressure assessment through a diagnostic catheter is limited. The aim of this study was to assess the difference, safety, and rate of successful measurement of Instantaneous Wave-free Ratio (iFR) through 4Fr and 5Fr diagnostic catheters.
Methods: This single-centre prospective study included 32 lesions among 24 patients exhibiting intermediate coronary stenosis on coronary angiography. iFR measurements were performed through 4Fr and 5Fr diagnostic catheters for each lesion. The primary outcome was the reliability, as assessed by a Bland–Altman plot, for comparison of the mean differences [mean ± 2 Standard Deviations (SDs)], and the agreement on the Kappa coefficient, using a threshold iFR value of 0.89. The secondary outcome was the rate of successful iFR measurement. Safety was assessed by procedural complications and in-hospital Major Adverse Cardiac Events (MACE).
Results: The mean difference was −0.0003 ± 0.058, according to the Bland–Altman plot. One lesion was out of the range of 2 SDs. There was good agreement (Kappa coefficient = 0.85), and the correlation coefficient between the 4Fr and 5Fr catheters was 0.948 (p < 0.001). The success rate was not significantly different between the 4Fr and 5Fr catheters (90.6% vs. 96.9%, p = 0.09), although the 4Fr catheter had a lower success rate. No procedural complications or in-hospital MACE occurred.
Conclusion: Our findings suggest that iFR measurements could be safely performed, with similar reliability and success rate, through either the 4Fr or 5Fr diagnostic catheter.
- HIGHLIGHTS
- •
Instantaneous Wave-free Ratio (iFR) measurements through 4Fr and 5Fr diagnostic catheters.
- •
Correlation and agreement of iFR between 4Fr and 5Fr.
- •
To compare the successful measurement of iFR values.
- •
- Copyright
- © 2020 Association for Research into Arterial Structure and Physiology. Publishing services by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Coronary pressure measurement, using a 0.014-inch pressure wire, has been widely used for the measurement of Instantaneous Wave-free Ratio (iFR), which is a new physiological index of coronary artery severity calculated during a wave-free period and without hyperaemic stimulation, with good repeatability [1–4]. Recently, an iFR value of 0.89 was used as a threshold cut-off value in two multi-centre, randomised, clinical trials that investigated whether the iFR was non-inferior to Fractional Flow Reserve (FFR). These studies revealed that the iFR-guided revascularization strategy was non-inferior to the FFR-guided revascularization strategy, in terms of Major Adverse Cardiac Events (MACE) at 12 months [5,6]. The use of a guiding catheter has been recommended for assessing coronary pressure measurement [7]. In Japan, following coronary angiography, a 4Fr or 5Fr diagnostic catheter has been often used for pressure assessment in cases presenting with intermediate coronary stenosis; however, the variation in iFR values between the 4Fr and 5Fr diagnostic catheter has not been elucidated. The present study aimed to evaluate the differences in iFR values, safety, and the rate of successful iFR measurement between the 4Fr and 5Fr diagnostic catheters.
2. MATERIALS AND METHODS
2.1. Patient Selection
This study was a single-centre, prospective study including 32 lesions in 24 patients who underwent elective coronary angiography due to stable angina pectoris between August 2015 and March 2016. Inclusion criteria were as follows: (1) showing intermediate coronary stenosis on coronary angiography, which was diagnosed at the operator’s discretion, (2) age ≥ 20 years, and (3) informed consent of the patients. Exclusion criteria were as follows: (1) presence of acute coronary syndrome, (2) presence of chronic kidney disease on hemodialysis, (3) measurement for bypass graft or previous history of coronary artery bypass grafting, and (4) prevalence of a target lesion with distal occlusion. The medical ethics committee of Saitama Eastern Cardiovascular Hospital approved this study, and written informed consent was obtained from every patient. The measurements and the whole study were conducted in accordance with the Declaration of Helsinki (1964).
2.2. Study Protocol
Study protocol is depicted in Figure 1. A 5Fr sheath was inserted in all patients. After sheath insertion, 3000 IU dose of heparin was administered intravenously, and intracoronary 0.2 mg of nitroglycerin was injected before coronary angiography. An additional intravenous injection of 2000 IU of heparin was administrated before FFR measurement. Coronary angiography was performed according to standard procedures. Pressure assessments were performed through the 4Fr and 5Fr diagnostic catheters (Technowood INF cath®, Technowood, Tokyo, Japan) with 1.10 and 1.20 mm luminal diameters, respectively. At first, FFR measurement was performed through a 5Fr diagnostic catheter following coronary angiography. Second, iFR measurements were performed twice for each lesion through both 4Fr and 5Fr diagnostic catheters, at least 5 min after the initial FFR measurement. Immediately after the procedure, the arterial sheath was removed.
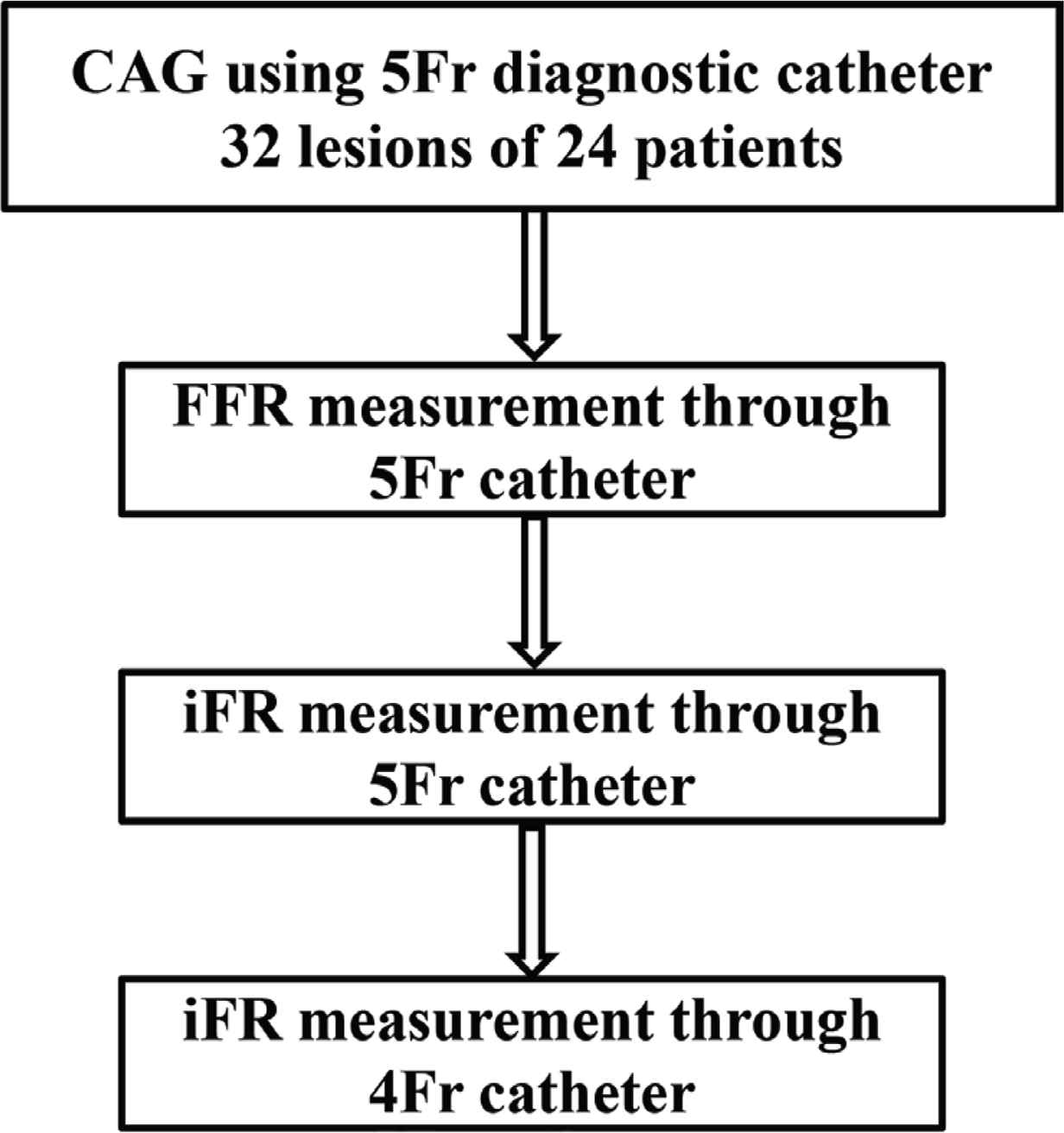
Study flow chart. CAG, coronary angiography.
2.3. Pressure Study
The pressure study was performed according to standard procedures. FFR and iFR measurements were performed using a 0.014-inch pressure guide wire (Verrata® pressure guide wire, Phillips Volcano Corporation, San Diego, CA, USA). After the wire was calibrated, the pressure wire was carefully advanced so that the pressure sensor was positioned and attached at the tip of the catheter. Normalization was performed at this location after the catheter was flushed with heparinized saline. After advancing the pressure wire to the distal segment of the target vessel, FFR measurement was performed through a 5Fr diagnostic catheter under intracoronary papaverine injection, which was administered over a span of 15 s. Injection dose was 8.0 mg for the right coronary artery and 12.0 mg for the left coronary artery. The diagnostic catheter was flushed with enough heparinized saline after intracoronary papaverine injection. FFR was measured 45–60 s after the intracoronary administration of papaverine. Following the FFR measurement, iFR measurements were performed twice through both 4Fr and 5Fr diagnostic catheters; the 5Fr catheter was used first, followed by the 4Fr catheter. Each iFR value was measured after stabilization of the pressure curve. At the end of each pressure measurement, the pressure wire was slowly pulled back to the location where the sensor and the tip of the catheter coincided – this was done to check the pressure drift. When the sensor of the pressure wire reached the tip of the diagnostic catheter, we confirmed the drift. If the FFR or iFR values were <0.98 or >1.02, repeat assessments were required until the FFR and iFR were within the range of 0.98–1.02.
2.4. Outcome Definitions
The primary outcome was the reliability of iFR values obtained with both 4Fr and 5Fr diagnostic catheters. The secondary outcome was the success rate, which was defined as crossing the tip of guide wire to the distal segment of the target lesion with a successful iFR measurement. The safety endpoint was assessed by any procedural-related complications, and in-hospital MACE. Procedure-related complications were defined as pressure wire or catheter-oriented complications such as coronary dissection, myocardial infarction, and ostial coronary artery injury due to a catheter. In-hospital MACE was defined as a composite of all-cause mortality, myocardial infarction, and stroke.
2.5. Statistical Analyses
Categorical variables are expressed as number and percentage, and continuous variables are expressed as mean ± Standard Deviation (SD). Reliability was assessed by (1) Bland–Altman plot, which was used to assess the mean difference of iFR values obtained by both 4Fr and 5Fr diagnostic catheters and (2) the Kappa coefficient, using a threshold value 0.89 for agreement. Pearson’s correlation coefficient was calculated to determine the relationship between iFR values. Success rates were compared using the student t-test. A p-value <0.05 was considered statistically significant. Statistical analyses were performed using SPSS statistical software 19 (IBM Corp., Armonk, NY, USA).
3. RESULTS
3.1. Study Population and Angiographic Findings
Clinical characteristics of the patients are shown in Table 1. Of these patients, 15 (62.5%) were male and the mean age was 70.1 ± 10.3 years. Fourteen patients (58.4%) had a history of percutaneous coronary intervention. Angiographic and procedural characteristics are shown in Table 2. Lesions located at the left anterior descending artery were observed the most (56.2%). Regarding the lesion type, type B2/C lesions were observed in 19 lesions of 32 lesions (59.3%), while 29 lesions (90.6%) were de novo lesions. The average total contrast volume was 87.0 ± 27.0 ml, while the average total procedure time was 76.0 ± 20.0 min.
| Variable (patients = 24) | N (%) |
|---|---|
| Age (years) | 70.1 ± 10.3 |
| Male | 15 (62.5) |
| Current smoker | 8 (33.3) |
| HTN | 21 (87.5) |
| DM | 11 (45.8) |
| DL | 21 (87.5) |
| Previous MI | 7 (29.2) |
| Previous PCI | 14 (58.4) |
| LVEF < 40% | 1 (4.2) |
| eGFR < 60 ml/min/1.73 m2 | 10 (41.7) |
| Approach site | |
| Radial artery | 23 (95.8) |
| Femoral artery | 1 (4.2) |
Values represent the mean ± SD or n (%). HTN, hypertension; DM, diabetes mellitus; DL, dyslipidemia; MI, myocardial infarction; PCI, percutaneous coronary intervention; LVEF, left ventricular ejection fraction; eGFR, estimate glomerular filtration rate.
Patients’ baseline clinical characteristics
| Variable (lesion = 32) | N(%) |
|---|---|
| Target vessel (LMT/LAD/LCX/RCA) | 2 (6.3)/18 (56.3)/3 (9.3)/9 (28.1) |
| ACC/AHA type B2, C | 19 (59.3) |
| De novo lesion | 29 (90.7) |
| In-stent lesion | 3 (9.3) |
| QCA analysis | |
| RD (mm) | 2.6 ± 0.5 |
| MLD (mm) | 1.4 ± 0.3 |
| %DS | 45 ± 9 |
| LL (mm) | 16 ± 8 |
| Pressure measurement | |
| FFR | 0.82 ± 0.08 |
| iFR5Fr | 0.89 ± 0.08 |
| iFR4Fr | 0.89 ± 0.09 |
| Type of catheter | |
| RCA (JR/BR) | 30 (92.7)/2 (6.3) |
| LCA (JL/BR) | 30 (92.7)/2 (6.3) |
| Contrast volume (ml) | 87 ± 27 |
| Procedure time (min) | 76 ± 20 |
LMT, left main trunk; RCA, right coronary artery; ACC, American College of Cardiology; AHA, American Heart Association; QCA, quantitative coronary angiography; RD, reference diameter; MLD, minimal lumen diameter; DS, diameter stenosis; LL, lesion length; JR, Judkins right; JL, Judkins left; LCA, left coronary artery.
Patients’ lesions and procedural characteristics. BR type diagnostic catheter is used for angiogram of the left and right coronary artery
3.2. Reliability
Figure 2 shows an example of a pressure curve during the iFR measurement. Pressure curves were clearly obtained with either 4Fr or 5Fr diagnostic catheters. In the 29 lesions that could be assessed for iFR using both 4Fr and 5Fr diagnostic catheters, Pearson’s correlation coefficient identified the linear relationship between the two catheters (R = 0.948, p < 0.001) (Figure 3A). Bland–Altman analysis showed that only one case was out of the range of the mean ± 2 SD. The mean difference was −0.0003, while the 95% confidence interval was −0.059 to 0.058 (Figure 3B). The Kappa coefficient was 0.85, showing good agreement between 4Fr and 5Fr diagnostic catheters.
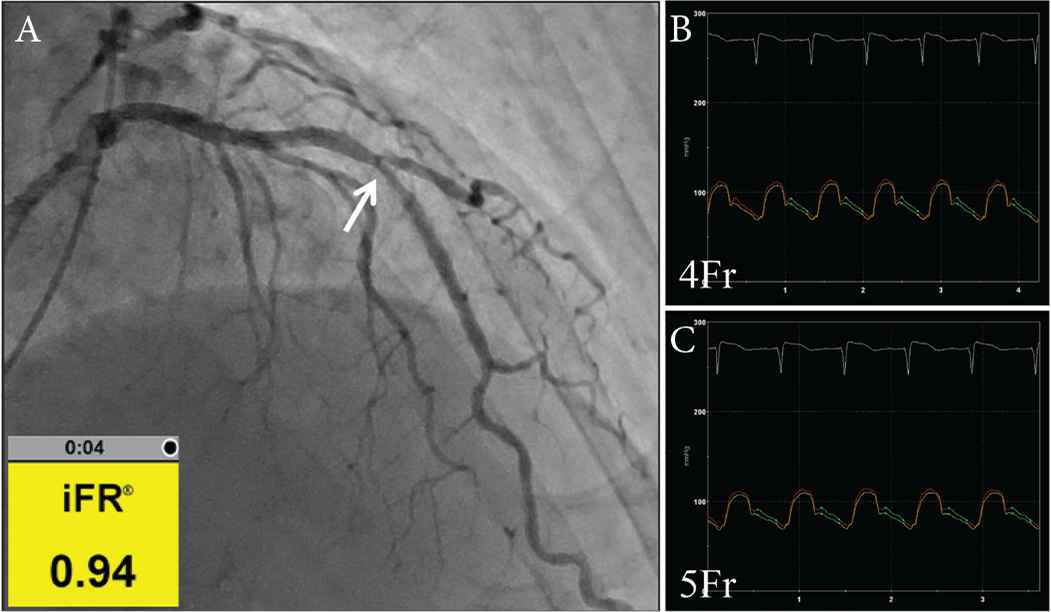
Representative case of an assessment of Instantaneous Wave-free Ratio (iFR) through 4Fr and 5Fr diagnostic catheters. (A) White arrow indicates intermediate stenosis in the middle-segment of the Left Anterior Descending artery (LAD). iFR value at the distal LAD was 0.94, calculated through both 4Fr and 5Fr diagnostic catheters. (B) Pressure curve obtained through a 4Fr diagnostic catheter. (C) Pressure curve obtained through a 5Fr diagnostic catheter.
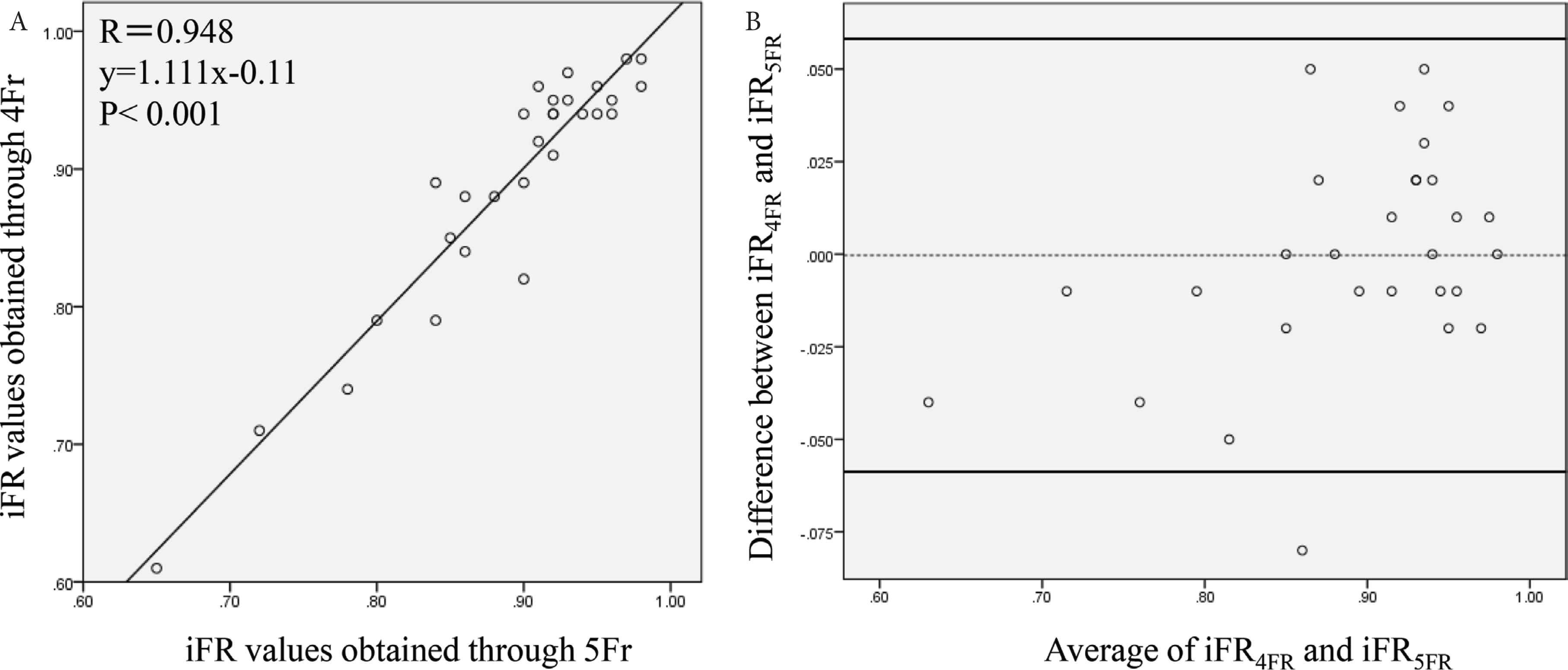
(A) Linear regression plot comparing Instantaneous Wave-free Ratio (iFR) values obtained through the 4Fr (y-axis) and 5Fr (x-axis) diagnostic catheters. There is a strong, linear correlation between iFR values obtained through the 4Fr and 5Fr catheters (R = 0.948, p < 0.001). (B) Bland-Altman plot for agreement between iFR values obtained using the 4Fr and 5Fr diagnostic catheters. Mean difference was −0.0003, and the 95% confidence interval was −0.059 to 0.058. iFR, instantaneous wave free ratio.
3.3. Success Rate and Safety
Instantaneous wave-free ratio was successfully measured in 29 of 32 lesions through the 4Fr diagnostic catheter, and in 31 of 32 lesions through the 5Fr catheter. The success rates were not significantly different between 4Fr and 5Fr catheters (90.6% vs. 96.9%, p = 0.09), although the 4Fr diagnostic catheters were less likely to be successful. Of 32 lesions, we could not assess the iFR value through either the 4Fr or 5Fr diagnostic catheter in one lesion, showing diffuse stenosis and calcification with moderate tortuosity at the Left Circumflex Artery (LCX) (Figure 4). Regarding the safety, there were no procedure-related complications during the procedure, or in-hospital MACE.
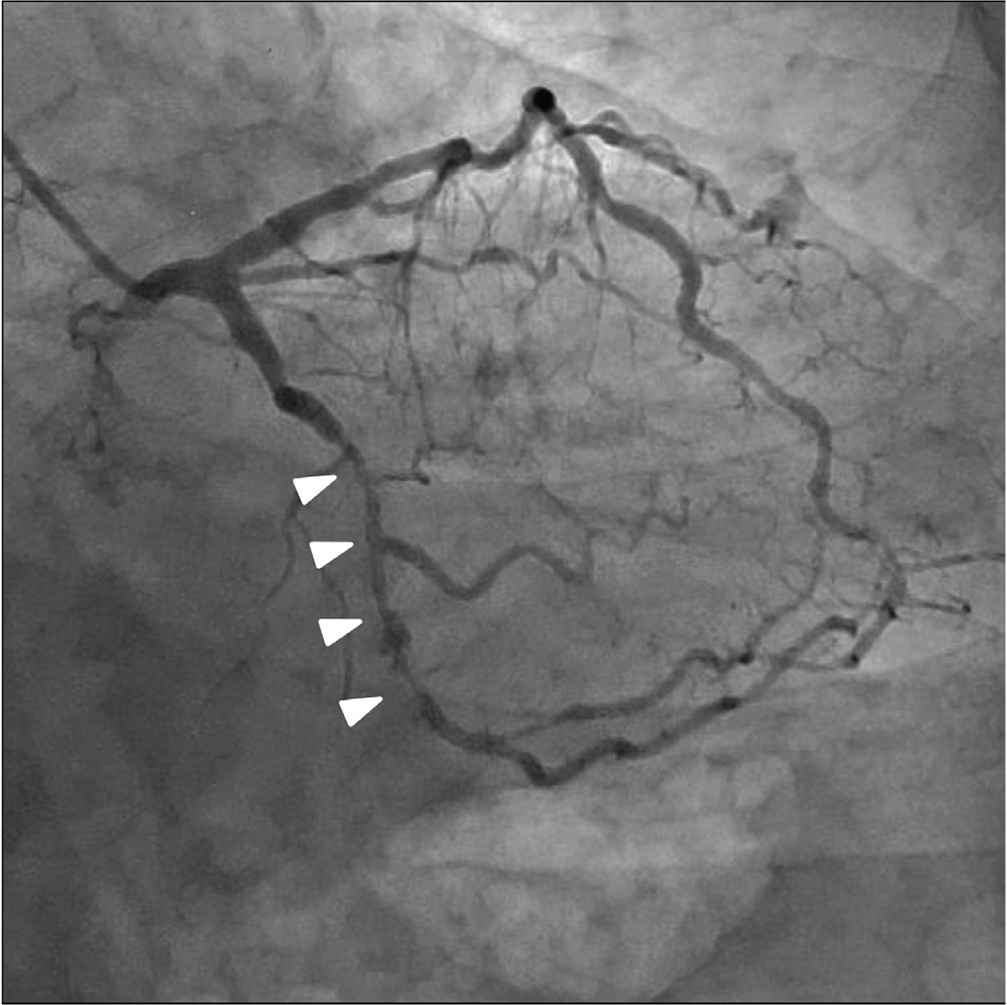
Coronary angiography of the case that was not assessed using either the 4Fr or 5Fr diagnostic catheter, showing diffuse stenosis and severe calcification with moderate tortuosity in left circumflex artery (white arrowheads).
4. DISCUSSION
The major findings of the present study were as follows: (1) the iFR values obtained through 4Fr and 5Fr diagnostic catheters showed a good correlation, with an acceptable agreement; (2) the success rates of iFR measurements were not significantly different. To the best of our knowledge, this is the first study to compare the differences in iFR values between the 4Fr and 5Fr diagnostic catheters.
The use of a diagnostic catheter has not been recommended for coronary artery pressure assessment because of the lack of back-up force and blunted pressure signal; therefore, reliable aortic waveform cannot be routinely obtained [7,8]. Despite this, diagnostic catheters have often been used for coronary pressure assessment in Japan. According to expert consensus, the 5Fr diagnostic catheter is widely accepted because of the clinical environment [9]. In several clinical studies, diagnostic catheter was used for iFR assessment [10,11]. Although, there were no clinical data regarding iFR assessment through a 4Fr diagnostic catheter, a previous clinical study reported that pressure waveform could be obtained through a 4Fr diagnostic catheter, and FFR measurement had a good repeatability, comparable to that with a 7Fr guiding catheter [12].
As we expected, our results showed that coronary waveform could be clearly obtained through either a 4Fr or 5Fr catheter; this was in agreement with a previously reported clinical study [12]. Furthermore, the difference in iFR values between 4Fr and 5Fr catheters was acceptable. These findings may serve for several aspects. First, iFR measurement through the 4Fr diagnostic catheter may reduce radial artery occlusion, compared to the 5Fr catheter. In our country, the trans-radial approach has been a popular approach for coronary angiography. In the trans-radial approach, the use of a bigger sheath can lead to vascular damage, which leads to radial artery occlusion. Previous clinical studies that assessed vascular complication via the trans-radial approach between the 5Fr and 6Fr sheaths demonstrated that the use of a 5Fr sheath was associated with a lower rate of access site radial artery occlusion, compared with that of a 6Fr sheath [13,14]. Similar to this finding, iFR measurement through a 5Fr diagnostic catheter may be associated with a higher rate of vascular complications than on through a 4Fr diagnostic catheter. Moreover, if we perform iFR measurement through only 4Fr diagnostic catheter without change of the sheath to 5Fr, we can avoid repeat sheath insertion, which may also reduce vascular complications. The second advantage to use a 4Fr catheter is the economic benefit. In cases of coronary angiography using a 4Fr diagnostic catheter, a 5Fr diagnostic catheter is additionally needed when coronary pressure assessment required following diagnostic coronary angiography. We expect additional cost savings in this situation.
However, there are some points to be aware of regarding iFR measurement through diagnostic catheters. In our study, not all lesions could be assessed using the diagnostic catheters. Our results showed the successful measurement was achieved in 90.9% and 96.6% lesions with the 4Fr and 5Fr catheter, respectively. A previous clinical study assessing FFR through a 4Fr diagnostic catheter reported that in 6% of patients, a crossover to a 7Fr guiding catheter was needed [9]. Unlike a guiding catheter, a diagnostic catheter is not made for crossing a 0.014-inch pressure wire and is not covered with hydrophilic-coating; therefore, it is assumed that friction may occur easily, which likely contributes to deterioration that might lead to failure of accuracy of iFR measurement. In this study, the pressure wire could not be advanced through either the 4Fr or 5Fr catheter in one lesion, which presented diffuse stenosis and calcification with moderate tortuosity in the LCX due to the lack of back-up force. Collectively, in pressure measurement through a diagnostic catheter in cases of complex lesions, it was suggested that the use of a back-up type catheter, or guiding catheter was preferable.
This study has a few limitations. First, this was a single-centre study based only on a small number of cases. Further study with a larger sample size is needed to support this result. Second, the deterioration of the pressure wire might have affected the result because the same wire was used among all the pressure assessments. Investigation using a new pressure guide wire at each pressure assessment is needed to confirm the repeatability. Third, lumen diameters of currently available diagnostic catheters are different. In this study, we used a 4Fr diagnostic catheter with a 1.10-mm lumen diameter, which has enough lumen area to reflect the pressure waveform. Therefore, our result has been established under the results of iFR measurement using a diagnostic catheter with a luminal diameter larger than 1.10 mm. Fourth, pressure measurements firstly performed through a 5Fr diagnostic catheter. Procedure was not randomized with 4Fr and 5Fr; therefore, we could not completely exclude any potential systematic bias.
5. CONCLUSION
Our findings suggest that iFR measurements could be safely performed, with similar reliability and success rate, through either the 4Fr or 5Fr diagnostic catheter.
CONFLICTS OF INTEREST
The authors declare that there is no conflicts of interest regarding the publication of this article.
AUTHORS’ CONTRIBUTION
SM and RU study conceptualization and writing (review & editing) the manuscript. SM, RU, YS and TH Data curation, formal analysis and writing (original draft). SM project administration. RU and TL supervised the project. SM and YS formal analysis and writing (original draft) the manuscript.
FUNDING
No financial support was provided.
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Shinichiro Masuda AU - Ryota Uemura AU - Yoshiyuki Saiki AU - Tatsuo Haraki AU - Takeshi Lee PY - 2020 DA - 2020/06/26 TI - Measurement of Instantaneous Wave-free Ratio through a Diagnostic Catheter: Comparison of the Results between 4Fr and 5Fr JO - Artery Research SP - 143 EP - 147 VL - 26 IS - 3 SN - 1876-4401 UR - https://doi.org/10.2991/artres.k.200620.001 DO - 10.2991/artres.k.200620.001 ID - Masuda2020 ER -