
Effects of transient change in carotid arterial stiffness on arterial baroreflex during mild orthostatic stimulation
- DOI
- 10.1016/j.artres.2012.05.002How to use a DOI?
- Keywords
- Arterial compliance; Carotid-vagal baroreflex; Head-up tilt
- Abstract
Stiffening of central conduit arteries –areas where the mechanoreceptors are embedded (e.g., ascending aorta and carotid artery) – is considered to be associated with the impaired baroreflex control in response to hypotensive stress. Arterial stiffness is modulated by vascular tone transiently and dynamically, however, it is unknown whether a transient change in the carotid artery stiffness influences the cardiac baroreflex response to a rapid hypotension. We measured (n = 11) carotid arterial stiffness (via concurrent applanation tonometory and ultrasound imaging) at supine rest and during 20-degree head-up tilt (HUT). To evaluate the cardiac baroreflex response, acute hypotension was evoked by releasing bilateral thigh cuffs after 3 min of suprasystolic resting ischemia at each posture; cardiac baroreflex sensitivity (e.g., change in heart rate for a given change in mean arterial pressure, ΔHR/ΔMAP) and latency (e.g., the time to peak HR response) was estimated. Carotid β-stiffness index, a measure of arterial stiffness, was reduced by 14% during HUT (P < 0.05 vs. supine position). Although cardiac baroreflex responses were unaltered, the within-group biological variability in the cardiac baroreflex sensitivity and latency from the supine to HUT was correlated with the corresponding changes in carotid arterial stiffness (r = 0.66 and r = 0.64, respectively, both P < 0.05). These findings suggest that a transient change in carotid arterial stiffness, at least in part, influences changes in the cardiac baroreflex response to a rapid hypotension.
- Copyright
- © 2012 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
In response to transient changes in arterial blood pressure (BP), the autonomic nervous system reflexively regulates heart rate (HR),1 sympathetic nervous activity,2,3 and peripheral vascular resistance4 via baroreflex mechanisms in order to maintain mean arterial pressure (MAP). Cardiac baroreflex sensitivity, evaluated by the maximal gain of carotid-HR baroreflex curve, gradually increases with incremental orthostatic stimulation.1,5 This change in sensitivity likely reflects favorable cardiovascular modulation in the face of orthostatic stress in order to help maintain MAP. In humans, reductions in cardiac filling with mild (e.g., −10 mmHg) lower body negative pressure (LBNP) unloads the cardiopulmonary baroreflex and augments the carotid baroreflex control of HR.1,6 These findings highlight the potential influence of unloading cardiopulmonary baroreceptors on carotid-cardiac baroreflex function.
Evidence indicates that alterations in vascular tone transiently and dynamically modulates arterial stiffness.7–9 Stiffening of central conduit arteries –areas where the mechanoreceptors are embedded (e.g., ascending aorta and carotid artery) – is associated with the impaired baroreflex control in response to hypotensive stress and contributes to orthostatic hypotension.10 Therefore, a transient change in carotid arterial stiffness may influence the carotid-cardiac baroreflex during orthostatic stimulation. In support of this, Steinback et al.11 reported that severe orthostatic stress [60° head-up tilt (HUT)] decreases carotid arterial distensibility (e.g., increases carotid arterial stiffness) as assessed via the relationship between carotid arterial pressure and diameter; these changes are associated with decreases in cardiac baroreflex sensitivity (as assessed using the “closed-loop” dynamic relationship between spontaneous fluctuations in BP and HR). However, the response of the cardiac baroreflex sensitivity to orthostatic stress11 occurred in the opposite direction to earlier studies using “open-loop” analysis.1,5 Recently, we have suggested the possibility that dynamic analysis under the closed-loop condition, especially during orthostatic stress, misleads the interpretation of actual characteristic of baroreflex function which could be quantified by the open-loop analysis.12 The other concern is that severe orthostatic stimulation elicits greater activation of cardiopulmonary baroreflex, decrease in pulse pressure or tachycardia, and thus may provide an additional modulation of the actual cardiac baroreflex function.13 Therefore, it remains unclear whether orthostatic stress-induced change in carotid arterial stiffness influences baroreflex function in healthy humans.
Accordingly, the aim of this study was to determine whether transient change in carotid arterial stiffness influences the baroreflex control of HR in response to acute hypotension. We specifically applied mild HUT (e.g., 20°) to manipulate carotid arterial stiffness because i) mild HUT does not affect carotid arterial baroreflex control of HR14 or pulse pressure; ii) large individual variability of carotid-cardiac baroreflex sensitivity change is observed during mild HUT1; and iii) our mild HUT stimulus is adequate to modulate carotid arterial stiffness via the previously reported elevations in muscle sympathetic nervous activity.2,3 We hypothesized that the smaller the increased in carotid arterial stiffness would be related to a larger the augmentation of cardiac baroreflex response (and vice versa). Because exogenous perturbation to the baroreflex system enables us to estimate the open-loop baroreflex transfer characteristics even under closed-loop conditions,20 we used the thigh cuff release-induced abrupt hypotension.15 The cardiac baroreflex function was gauged from both the sensitivity (e.g., change in heart rate for a given change in mean arterial pressure, ΔHR/ΔMAP) and latency (e.g., the time to peak HR response).
Materials and methods
Subjects
Eleven healthy men with a mean age of 22 ± 4 yr, height of 170 ± 6 cm, and weight 65 ± 9 kg voluntarily participated in this study. Each subject provided written, informed consent after all potential risks and procedures were explained. All experimental procedures and protocols conformed to the Declaration of Helsinki and were approved by the Institutional Review Boards of Faculty of Biomedical Engineering, Toyo University (IRB # 2009-R-01). None of the subjects reported using medications, recreational drugs or had significant chronic medical problems. All subjects were familiarized with the equipment and procedures before any experimental sessions.
Experimental protocols
On experimental days, subjects arrived at the laboratory a minimum of 2 h following a light meal. The subjects were placed supine on a tilt-table, and connected to the instruments described below. The experiment was composed of two protocols under two different conditions: supine and HUT of 20°. During HUT, the subjects were supported by a bicycle saddle with no footboard and were requested to abstain from leg movement to mitigate the influence of leg muscle contraction. Each protocol was composed of a 3-min baseline period, 3-min bilateral thigh cuff-occlusion, and a 3-min post-cuff release period. Supine and HUT trials were randomly conducted among the subjects and repeated in duplicate. Baseline measurement at the first trial of each condition was performed after 10 min of resting in each position. The second trial of each condition was carried out at least 3 min apart from the termination of the prior trial.
Hemodynamics
HR was continuously monitored using a lead II electrocardiogram (ECG). Beat-to-beat arterial BP was measured using a noninvasive tonometry monitoring system (BP-608; Omron Colin, Kyoto, Japan) obtained from the left wrist (the radial artery), which was supported at the level of the right atrium on an adjustable padded bedside support. These data were continuously sampled at 1 kHz with an analog-to-digital converter (PowerLab 8/30, AD Instruments, Bella Vista, Australia) interfaced with a personal computer equipped with data acquisition software (LabChart 6, AD Instruments, Bella Vista, Australia) for the beat-to-beat recording of physiological variables.
Carotid arterial properties
Using a high-resolution (10-MHz) linear transducer (SonoSite180PLUS, SonoSite Inc., Bothell) longitudinal images were continuously recorded 1–2 cm proximal to the right carotid bulb. Carotid arterial diameter was analyzed offline by a public domain, Java-based image processing program developed at the National Institutes of Health (Image J; http://rsbweb.nih.gov/ij/). Carotid arterial pressures were estimated at the left common carotid artery with applanation tonometry (Form PWV/ABI, Colin MT, Komaki, Japan). Carotid arterial pressure signals were stored at 1 kHz and were calibrated by equating the carotid mean arterial and diastolic blood pressure to the radial mean arterial and diastolic blood pressure.16 In order to account for hydrostatic pressure, radial arterial pressure was measured at the same level of carotid pressure recording point. Carotid arterial β-stiffness index was calculated by the following equation as previously reported17,18: ln (Ps/Pd)/(Ds/Dd)/Dd, where Ps and Pd are carotid systolic and diastolic BP, respectively and Ds and Dd are carotid systolic and diastolic diameters, respectively. The coefficients of variation for the two trials were 0.7 ± 0.2%, 3 ± 1%, and 4 ± 1% for carotid artery diameter, systolic BP, and diastolic BP, respectively.
Cardiac baroreflex function
Cardiac baroreflex function was evaluated from the HR response to the cuff release-induced abrupt hypotension.15 Three minutes of suprasystolic resting ischemia (+100 mmHg) was applied to manipulate MAP by a rapid cuff inflation system (E20 Rapid Cuff Inflator and AG101 Air Source; D.E. Hokanson, Inc., Bellevue, WA, USA). Although the cuff inflation was applied manually and gradually over 10–20 s to minimize pain at thighs, the cuff deflation (e.g., suprasystolic pressure to 0 mmHg) was achieved in 0.3 s. The change in HR at a given change in MAP (ΔHR/ΔMAP)15 and the time to peak HR response19 were calculated as indices of cardiac baroreflex sensitivity and latency, respectively; where ΔHR = peak HR after the cuff release − HR just before the cuff release and ΔMAP = MAP just before the cuff release − MAP at nadir after the cuff release.
Statistics
Data are expressed as mean ± S.E.M. Repeated measures ANOVA with Tukey HSD test or paired t-test were employed to determine significant differences in hemodynamics, carotid arterial properties, and cardiac baroreflex function between supine and HUT conditions. The relation between changes in carotid arterial stiffness and cardiac baroreflex function was determined by Pearson’s correlation coefficient. P-value of 0.05 was considered to represent statistical significance.
Results
There were no significant differences in baseline HR, brachial and carotid arterial blood pressures between supine and HUT conditions (Table 1). Carotid arterial diastolic and systolic diameters tended to be smaller in HUT compared with those in supine position (P = 0.06 and P = 0.09, respectively). Carotid arterial β-stiffness index was lower in HUT than the supine position (6.4 ± 0.5 vs. 5.5 ± 0.4 a.u., P < 0.05, Fig. 1).
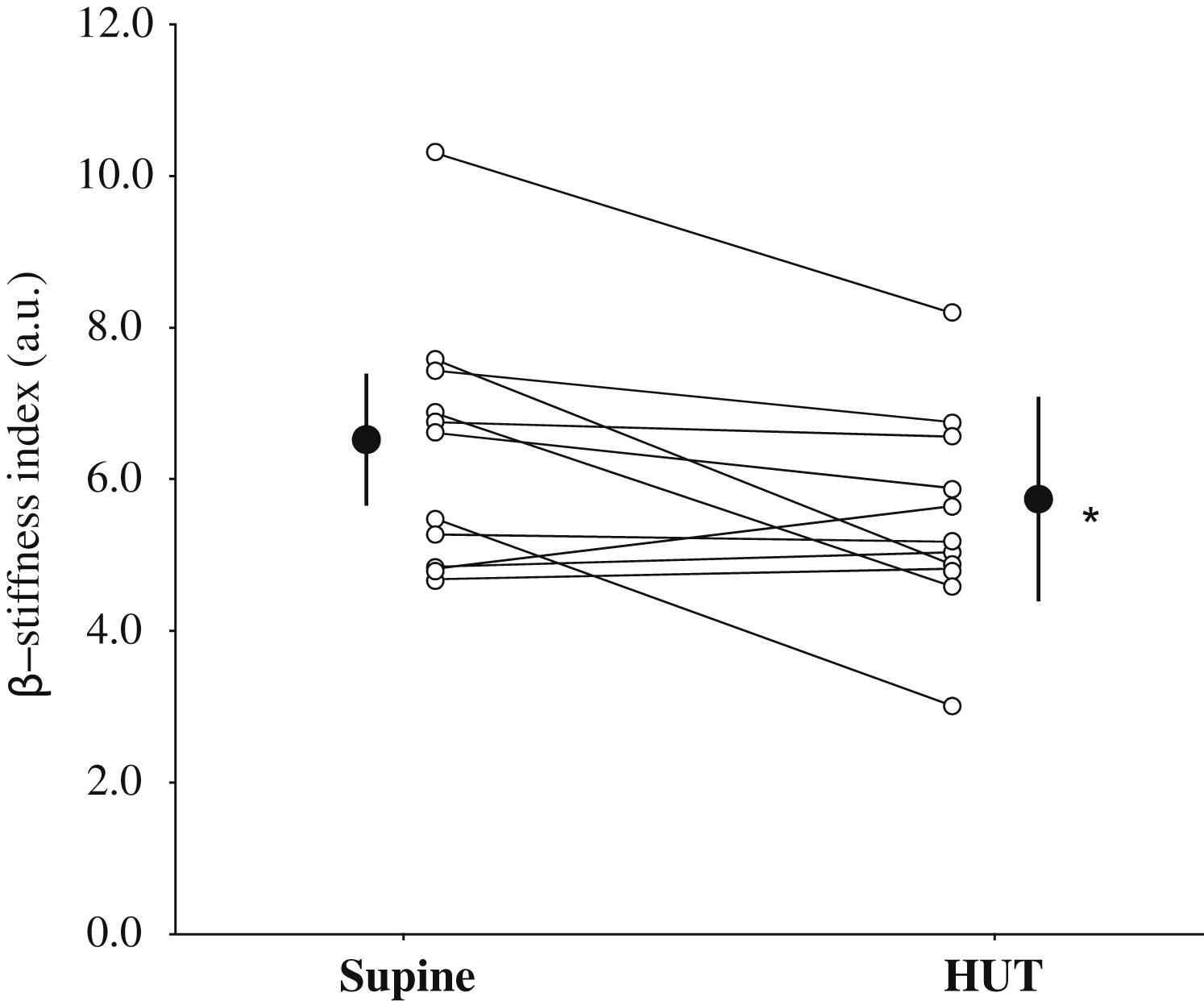
Comparison of carotid arterial β-stiffness index in supine and 20-degree head-up tilt (HUT) conditions. Open circles represent individual data. Filled circles are group mean (SD). *: P < 0.05 vs. supine position.
| Variables | Supine | HUT |
|---|---|---|
| Heart rate, bpm | 56 ± 4 | 60 ± 3 |
| Brachial MAP, mmHg | 79 ± 3 | 81 ± 3 |
| Brachial systolic BP, mmHg | 119 ± 3 | 118 ± 3 |
| Brachial diastolic BP, mmHg | 60 ± 2 | 64 ± 2 |
| Brachial PP, mmHg | 59 ± 2 | 55 ± 2 |
| Carotid systolic BP, mmHg | 106 ± 2 | 107 ± 3 |
| Carotid diastolic BP, mmHg | 60 ± 2 | 64 ± 2 |
| Carotid PP, mmHg | 46 ± 2 | 43 ± 1 |
| Carotid diastolic diameter, mm | 6.24 ± 0.07 | 6.08 ± 0.08 |
| Carotid systolic diameter, mm | 6.83 ± 0.07 | 6.68 ± 0.08 |
| Pulsatile diameter change, mm, | 0.58 ± 0.04 | 0.60 ± 0.04 |
Data are mean and SEM. MAP = mean arterial pressure, BP = blood pressure, PP = pulse pressure.
Baseline hemodynamics and carotid arterial properties during supine and head-up tilt (HUT).
Fig. 2 depicts example recordings of ECG, radial and carotid arterial blood pressure waveforms, and HR throughout the cuff release from one subject at supine rest and during 20-degree HUT. Bilateral thigh cuff release evoked a significant reduction in MAP followed by an increase in HR. The hypotensive response was significantly larger in HUT (from 94 ± 5 to 67 ± 4 mmHg, −26 ± 2 mmHg) than the supine position (from 96 ± 3 to 75 ± 3 mmHg, −21 ± 1 mmHg). There was no significant difference in HR response between supine (from 60 ± 3 to 73 ± 3 bpm, +13 ± 1 bpm) and HUT positions (from 61 ± 3 to 75 ± 4 bpm, +14 ± 1 bpm). The ΔHR/ΔMAP was not significantly different between supine and HUT positions (−0.68 ± 0.07 in supine vs. −0.62 ± 0.10 bpm/mmHg in HUT, P = 0.45, Fig. 3). The time (sec) to peak HR response was not significantly different between supine and HUT positions (3.34 ± 0.32 in supine vs. 3.64 ± 0.45 s in HUT, P = 0.66, Fig. 3). However, the individual changes in ΔHR/ΔMAP and time to peak HR response from the supine to HUT position correlated with the corresponding changes in β-stiffness index (r = 0.66 and r = 0.64, both P < 0.05; Fig. 4).
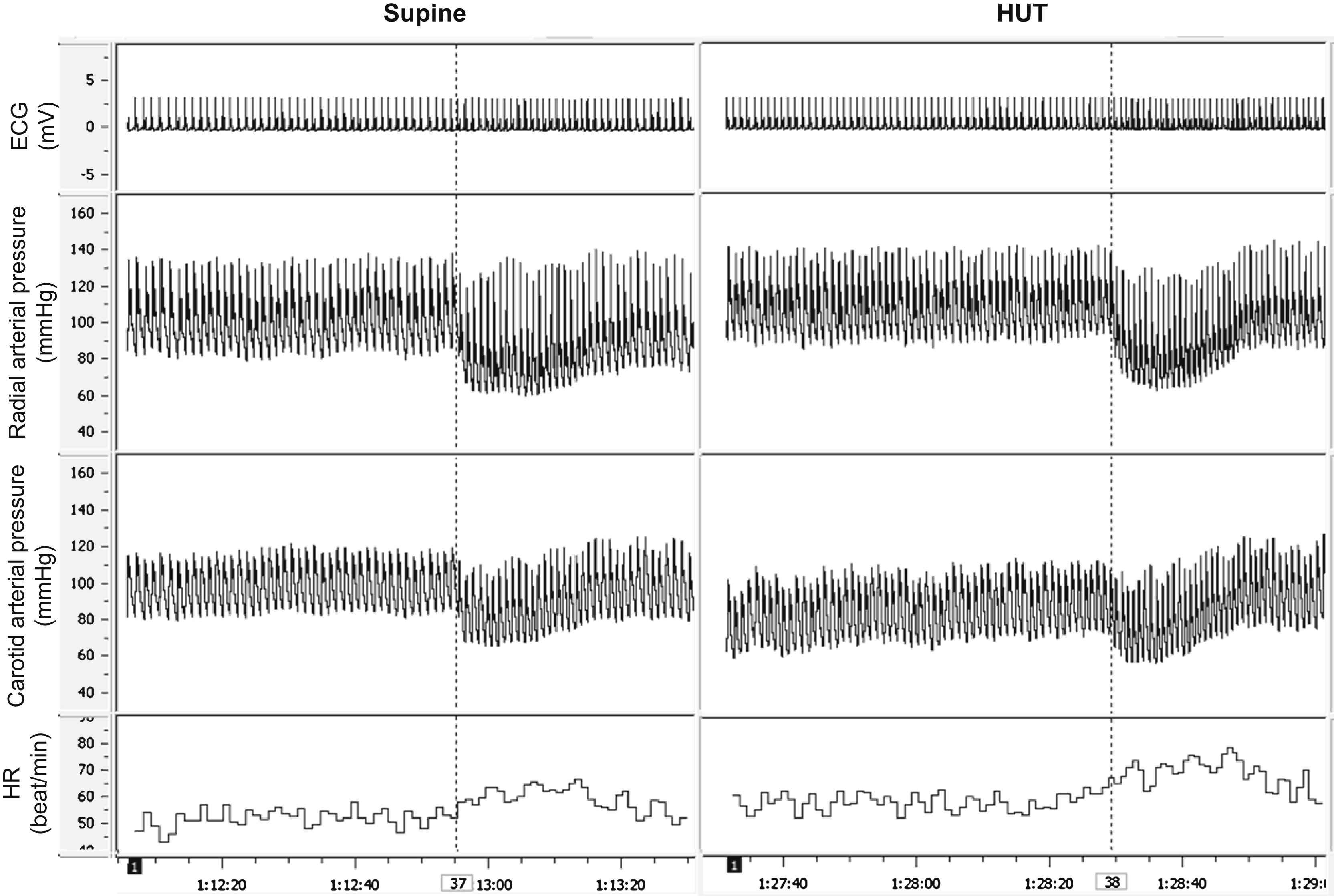
Example recordings of electrocardiogram (ECG), radial and carotid arterial blood pressure waveforms, and heart rate (HR) from one subject at supine rest (left panels) and during 20-degree head-up tile (HUT; right panels). Dotted lines represent the onset of cuff release.
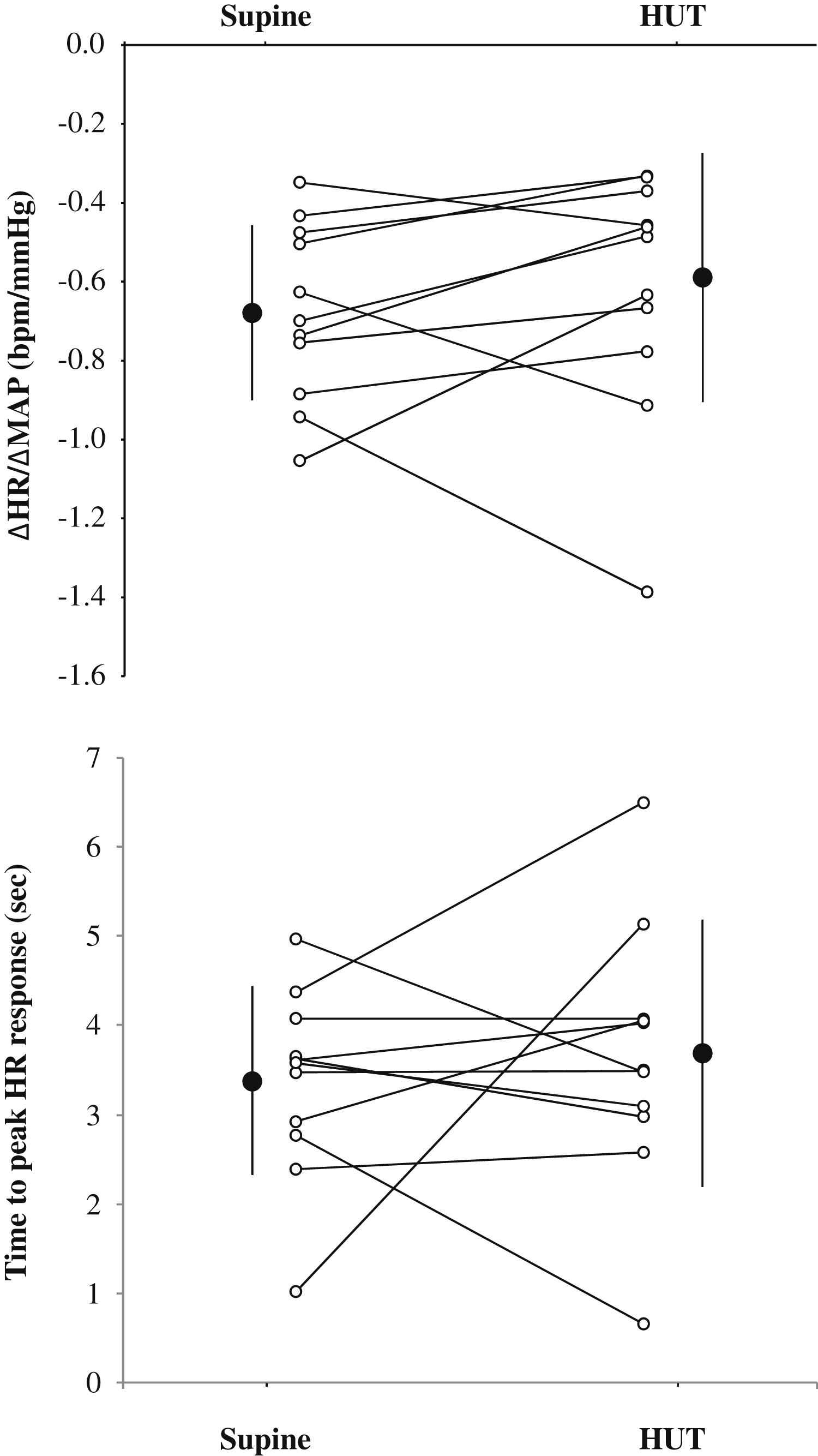
Comparison of arterial baroreflex sensitivity and latency in supine and 20-degree head-up tilt (HUT) conditions. The change in heart rate at a given change in mean arterial pressure (ΔHR/ΔMAP) and the time to peak HR response were calculated as indices of cardiac baroreflex sensitivity and latency, respectively. Open circles represent individual data. Filled circles are group mean (SD).
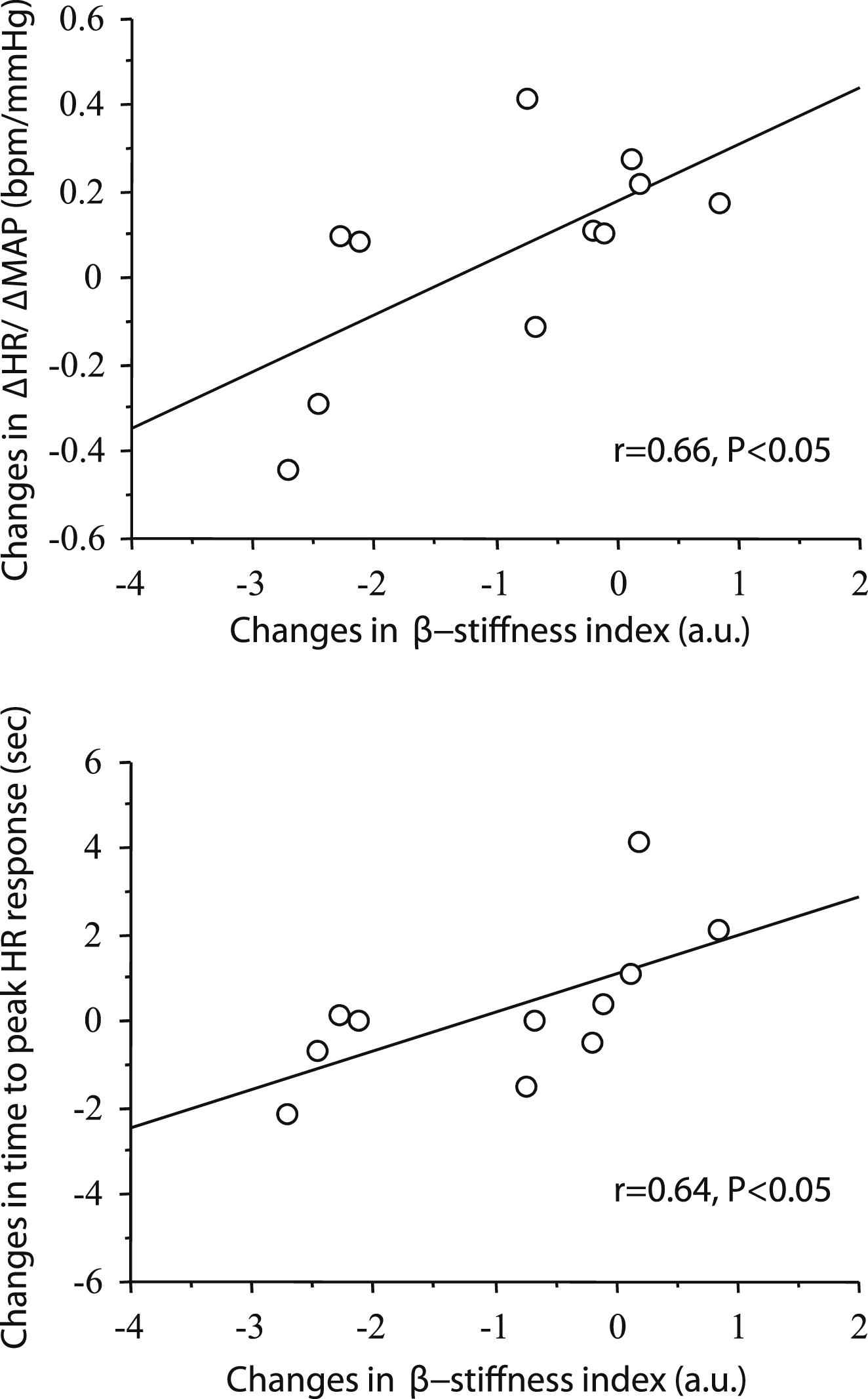
Correlations between transient changes in carotid arterial β-stiffness index from the supine to 20-degree head-up tilt (HUT) with the corresponding changes in ΔHR/ΔMAP and the time to peak HR response.
Discussion
We tested the hypothesis that the smaller the increased in carotid arterial stiffness would be related to a larger the augmentation of cardiac baroreflex response (and vice versa). Carotid arterial β-stiffness index were significantly lower during mild HUT compared with the supine position, whereas there were no differences in either ΔHR/ΔMAP or time to peak HR response between two positions presumably due to large individual variability. However, as hypothesized, within individuals, the changes in β-stiffness index from the supine to HUT position correlated with the corresponding changes in cardiac baroreflex response (magnitude and latency) variability. These results suggest that a transient change in carotid arterial stiffness, at least in part, influences changes in the cardiac baroreflex adjustments to rapid hypotension.
Unexpectedly, we identified a significant reduction in carotid arterial stiffness (assessed using β-stiffness index) during mild orthostatic stimulation. The mechanism(s) underlining this response was not identifiable with our study design. Whilst speculative, because arterial distension (e.g., pulsatile change in diameter) did not change, it may be that the reduced arterial diameter during HUT was due to diminished transmural pressure across the carotid artery rather than vessel contraction per se.
In this study, we applied mild orthostatic stress to manipulate carotid arterial geometry and stiffness because of following reasons: i) severe orthostatic stimulation activates cardiopulmonary baroreflexes, and thus may provide an additional modulation of the actual cardiac baroreflex sensitivity13; ii) the increase in pulse frequency (i.e., elevation of HR) lowers carotid arterial baroreflex afferent discharge21 and causes less baroreflex inhibition of sympathetic nervous activity.22 The orthostatic stimulation we employed did not evoke significant changes in HR during HUT, suggesting that activation of arterial baroreceptors and the interaction between carotid and cardiopulmonary baroreflexes should be minimal.
Baroreflex control of HR in response to hypotensive stress (i.e., postural change, hemorrhage) is an important protective mechanism against orthostatic hypotension and syncope.23 Therefore, we measured the cardiac baroreflex response using the HR response to the abrupt hypotension by bilateral thigh cuff release. Even under a closed-loop condition, exogenous perturbation to the baroreflex system enables us to estimate the open-loop baroreflex transfer characteristics from MAP to HR.12,20 Because the operating point of baroreflex function remains at the center of its function curve during orthostatic stress, baroreflex sensitivity to hypertensive is similar with that to hypotension.29 The bilateral thigh cuffs occlusion-release does not affect central venous pressure, and hence cardiopulmonary baroreflexes are not stimulated.15
Our findings indicate that approximately 44% of the variance in changes in the cardiac baroreflex sensitivity and latency are explained by the changes in β-stiffness index with mild orthostatic stress (Fig. 4). Broadly consistent with this finding, Monahan et al.24 suggested that age-related decrease and exercise training-induced increase in carotid artery compliance explain approximately 50% of the variance between the concomitant changes in cardiovagal baroreflex sensitivity with aging and exercise training, respectively. This finding supports and extends the notion that stiffness of central conduit arteries (in which the mechanoreceptors are located) is partly responsible for determining cardiac baroreflex sensitivity.10,24 The physiological mechanism that may account for the other factors are unclear but may involve neural component of vagal baroreflex.25–27
Our data in young healthy men may provide an additional mechanism for cardiovascular regulation during circulatory collapse (e.g., syncope). From a pathophysiology perspective, the association between transient changes in carotid arterial stiffness and cardiac baroreflex response may also be relevant in elderly adults because such populations have blunted cardiac baroreflex gain24 and latency,19 which might be associated with highly prevalence of orthostatic intolerance.28
Several methodological considerations are acknowledged. First, this study has a small sample size. Second, carotid arterial baroreflex regulates MAP not only by HR via cardiovagal nervous system but also vascular resistance via sympathetic nervous system. Because the latter arm was not evaluated in this study, interpretation is limited to the cardiac baroreflex response. Third, the bilateral thigh cuffs occlusion-release may activate both aortic and carotid arterial baroreceptors and we could not quantify aortic-cardiac and carotid arterial-cardiac baroreflex function separately. Additionally, the cuff release induces production of metabolite with potential vasoactive properties, and which may influence vasomotor response.
In conclusion, we identified that the individual changes in β-stiffness index from the supine to HUT position positively correlated with the corresponding changes in cardiac baroreflex response (magnitude and latency) variability. In other words, individuals who showed larger reduction in carotid arterial stiffness exhibited larger improvement of baroreflex control of HR during mild orthostatic stimulation. These findings suggest that transient changes in carotid arterial stiffness are, at least in part, associated with changes in the cardiac baroreflex response during mild orthostatic stress.
Conflict of interest
None.
Acknowledgment
This study was supported by the Uehara Memorial Foundation (JS) and Center for Academic Researches Promotion (Toyo University Research Institution of Industrial Technology, Grant #7) (SO).
References
Cite this article
TY - JOUR AU - Jun Sugawara AU - Christopher K. Willie AU - Taiki Miyazawa AU - Hidehiko Komine AU - Philip N. Ainsle AU - Shigehiko Ogoh PY - 2012 DA - 2012/06/07 TI - Effects of transient change in carotid arterial stiffness on arterial baroreflex during mild orthostatic stimulation JO - Artery Research SP - 130 EP - 135 VL - 6 IS - 3 SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2012.05.002 DO - 10.1016/j.artres.2012.05.002 ID - Sugawara2012 ER -