
Factors influencing hemodynamic and morphological indicators of carotid arteries atherosclerosis in treated hypertensive patients
- DOI
- 10.1016/j.artres.2010.08.001How to use a DOI?
- Keywords
- Intima-media thickness; Resistive index; Arterial hypertension; Carotid atherosclerosis
- Abstract
Objectives: To evaluate factors influencing resistive index (RI) and intima-media thickness of common carotid artery (IMT-CCA) as indices of arterial atherosclerosis in hypertensive patients.
Methods: 56 treated hypertensive outpatients (mean age 68.9 ± 9.7 years; 31 diabetics) were examined. Fasting blood glucose, cholesterol, and HbA1c concentration and glomerular filtration rate were measured. Systolic (SBP), diastolic blood pressure (DBP) and pulse pressure were estimated during ambulatory blood pressure monitoring. Ultrasonography of the CCA was performed with determination of IMT-CCA and RI.
Results: With diabetes IMT-CCA was significantly (1.025 ± 0.17 vs 0.928 ± 0.18 mm, p = 0.04) and RI not significantly (0.71 ± 0.06 vs 0.68 ± 0.08, p = 0.07) higher. A correlation between HbA1c and RI, IMT-CCA and the age was found. After dividing the whole group into subgroups corresponding to the tertiles of HbA1c levels, mean IMT-CCA values in I and II tertile were significantly lower than in III tertile (p = 0.008 and p = 0.002 respectively), while RI was significantly higher in III tertile than in I tertile (p = 0.03). On multiple regression analysis IMT-CCA was significantly influenced by the age (β = 0.343, p = 0.04), SBP (β = 0.430, p = 0.03) and HbA1c (β = 0.369, p = 0.01), while RI was influenced by SBP (β = 0.696, p = 0.0006), DBP (β = −0.618, p = 0.003) and HbA1c (β = 0.279, p = 0.04).
Conclusion: Patients with hypertension and diabetes mellitus had significantly increased IMT and not significantly higher RI. Concentration of HbA1c, next to the age, SBP and DBP values was independently associated with IMT-CCA and RI – parameters determining indirectly the degree of atherosclerosis of common carotid artery.
- Copyright
- © 2010 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
Arterial hypertension is one of the major atherosclerosis risk factors. Intima-media thickness of the common carotid artery (IMT-CCA) has been regarded as a best-studied marker of early stage of atherosclerosis, which precedes atherosclerotic changes and plaque formation.1–3 According to current studies arterial hypertension, especially increase in systolic blood pressure (SBP), is one of the most important independent factors influencing IMT. It is confirmed by the fact that hypertensive patients have increased IMT and higher incidence of atherosclerotic plaque in CCA in comparison with normotensive patients.4 According to current guidelines of European Society of Hypertension, European Society of Cardiology (ESH/ESC)5 an increase in IMT to a mean of 0.9 mm or greater is considered as end-organ damage in the course of hypertension. The relationship between IMT and other cardiovascular risk factors such as the age, male sex, cigarette smoking, obesity, hypercholesterolemia, elevated homocysteine, hyperuricemia and diabetes mellitus has been proved. Furthermore, IMT has been also suggested as a prognostic index for the increased incidence of myocardial infarction and stroke.4,6–13
One can make an assumption that development of morphological changes such as increase in IMT is preceded by impairment of vessel wall function, which is reflected by hemodynamic indicators.
The Resistive Index (RI) was introduced by Pourcelot14 in 1974, to detect peripheral vascular disease. It is calculated from blood flow velocities in vessels during the cardiac cycle by a pulsed-wave Doppler ultrasound. An increased value of RI is associated with a high difference in velocity between the systolic and the diastolic phase. The difference in flow velocities reflects downstream resistance, which could at least partly depend on the degree of peripheral arterial stiffness.15,16 The measurement of RI in renal arteries has been suggested as a reliable marker of downstream renal resistance,15,16 renal artery stenosis17 and kidney graft rejection.18 Furthermore, the measurement of RI of intrarenal arteries has been used to assess the severity of target organ damage in patients with hypertension, diabetes mellitus and chronic renal failure.19–21 It has been revealed not only that RI is significantly higher in hypertensive patients in comparison with normotensive ones, but that it also depend on renal flow, on renal vascular resistance and on creatinine clearance,19 and correlate significantly with albumin/creatinine index20 and IMT-CCA.20,22
Despite the fact that RI in carotid arteries has not been studied so extensively, the latest reports have shown that prognostic value of this index is similar to a prognostic value of IMT-CCA.23–25 Increase in both RI and IMT indirectly reflects decrease in vascular elasticity and distensibility.
The aim of this study was to evaluate factors influencing resistive index and intima-media thickness of common carotid artery as hemodynamic and morphological indices of arterial atherosclerosis in a population treated for arterial hypertension.
Methods
Fifty-six outpatients treated for arterial hypertension, aged 48–90 years, were recruited to the study. All participants expressed their consent to take part in the additional examination with the understanding that part of the data might be anonymously used for scientific purposes. Data concerning coexisting risk factors, co-morbidities and treatment were obtained as a part of routine work-up.
Laboratory tests
Fasting blood samples were taken in the morning. Plasma glucose and cholesterol concentration were measured using universally applied methods. Glycated hemoglobin (HbA1c) was measured using high-performance liquid chromatography (HPLC). Glomerular filtration rate was estimated according to the Cockcroft–Gault formula (GFR = [140 − age (years) × body weight (kg)/0.814 × plasma creatinine (μmol/l) – the resulting value was multiplied by a constant of 0.85 if the patient was female).
Blood pressure measurement
In all participants the ambulatory blood pressure monitoring (ABPM) was performed by the use of the SpaceLab 90207 device (SpaceLab Inc., Redmont, WA). Mean values of systolic blood pressure (SBP) and diastolic blood pressure (DBP) from 24 h were used in further analysis.
Ultrasonography of carotid arteries
Common carotid arteries were assessed by use of B-mode ultrasonography performed with an ultrasound scanner (Vivid 3, General Electric) equipped with a 10 MHz linear probe. Common carotid arteries and their bifurcations were viewed bilaterally, in their longitudinal dimension, in anterior oblique or lateral projection, in a patient in the supine position, with his/her head turned about 45 degrees in relation to the sagittal plane of the body respectively to the right or to the left side. Frozen images were archived and analyzed offline manually by the use of Image Pro Plus 4.5 software (Media Cybernetics). The average IMT value (IMT-CCA) was calculated for the 4 IMT values measured at near and far wall of common carotid artery proximally to its bifurcation, bilaterally.
During Doppler ultrasonography examination peak systolic and minimum diastolic velocity were recorded. Resistive index in common carotid artery was calculated by the built-in computer software as follows: RI = (peak systolic velocity − end-diastolic velocity)/peak systolic velocity (Fig. 1).
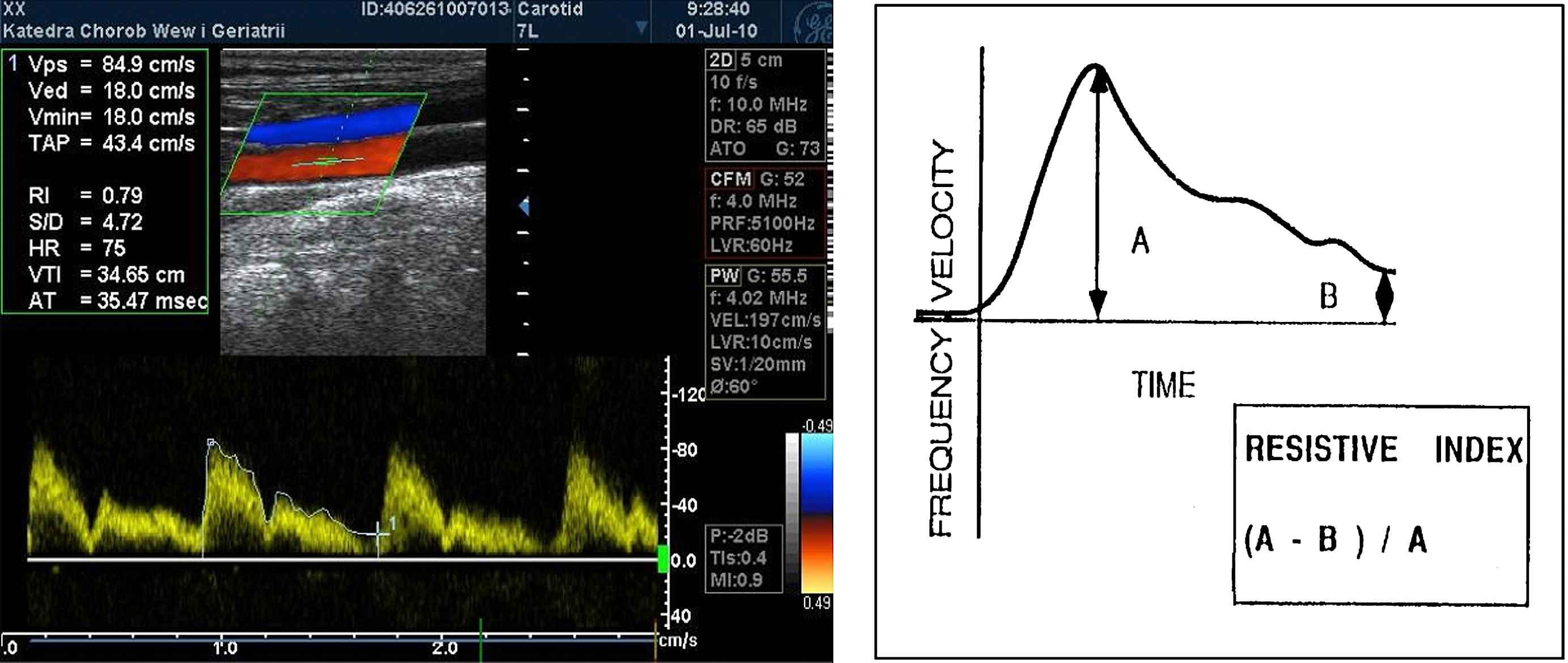
Measurement of resistive index in common carotid artery (A – peak systolic velocity, B – end diastolic velocity).
Statistical analysis
The statistical analysis was performed using Statistica version 8.0. The values were expressed as means ± standard deviations (SD). Shapiro–Wilks’ test was used to assess the distribution of the variables. Because of non-normal distribution of variables the differences between the mean values were analyzed with the use of Mann–Whitney U-test. The correlation between HbA1c and variables under study was assessed with Spearman’s correlation test.
Additionally one-way ANOVA was used to compare mean IMT-CCA and RI values between the three subgroups corresponding to tertiles of HbA1c level, independently of the presence of diabetes. Multiple regression analysis was performed to identify factors which independently influenced RI and IMT. As a dependent variable RI was included to the first regression model and IMT-CCA to the second one. As operands age, sex, body mass index (BMI), cigarette smoking, presence of diabetes, duration of arterial hypertension, heart rate, HbA1c, plasma cholesterol concentration, treatment with ACEI, calcium channel blockers, beta blockers, SBP, and DBP (or pulse pressure, PP) were used.
Results
The average age of 56 examined patients (39 females and 17 males) was 68.9 ± 9.7 years. Thirty-one persons of 56 subjects (55.35%; 12 males) were treated for diabetes mellitus. Sixteen persons (28.6%; 7 males) were active smokers. Baseline characteristics of study population are presented in Table 1.
| Total population n = 56 | Females n = 39 | Males n = 17 | p | |
|---|---|---|---|---|
| Age (years) | 68.9 ± 9.7 (48–90) | 69.7 ± 9.6 | 67.2 ± 10.0 | 0.4 |
| BMI (kg/m2) | 28.43 ± 4.8 (20.68–42.7) | 28.3 ± 4.9 | 28.8 ± 4.4 | 0.72 |
| Glucose (mmol/L) | 6.3 ± 2.1 (4.11–14.8) | 5.91 ± 1.9 | 7.20 ± 2.4 | 0.03 |
| Cholesterol (mmol/L) | 5.27 ± 1.0 (3.6–8.57) | 5.36 ± 1.1 | 5.06 ± 0.8 | 0.29 |
| HbA1c (%) | 7.26 ± 1.9 (4.3–13.6) | 7.32 ± 2.1 | 7.13 ± 1.4 | 0.72 |
| RI | 0.69 ± 0.07 (0.52–0.84) | 0.697 ± 0.07 | 0.682 ± 0.08 | 0.45 |
| IMT-CCA (mm) | 0.978 ± 0.18 (0.586–1.543) | 0.973 ± 0.17 | 0.991 ± 0.19 | 0.73 |
| SBP (mmHg) | 129.44 ± 17.94 (98–188) | 128.97 ± 18.8 | 130.44 ± 16.3 | 0.77 |
| DBP (mmHg) | 72.19 ± 11.18 (52–114) | 71.4 ± 10.8 | 74.0 ± 11.9 | 0.41 |
| PP (mmHg) | 57.2 ± 12.3 (32–100) | 57.6 ± 12.4 | 56.4 ± 12.5 | 0.74 |
| eGFR (ml/min) | 74.6 ± 25.9 (25.8–134.8) | 70.77 ± 25.9 | 82.87 ± 24.7 | 0.10 |
BMI – body mass index, HbA1c – glycated hemoglobin, RI – resistive index, IMT-CCA – common carotid artery intima-media thickness, SBP – systolic blood pressure, DBP – diastolic blood pressure, PP – pulse pressure, eGFR – estimated glomerular filtration rate.
Baseline characteristics of study population.
Men and women did not differ between themselves in examined values, except for glucose level. While diabetics were characterized by significantly higher IMT (1.025 ± 0.17 vs 0.928 ± 0.18 mm, p = 0.04), and higher, although not significantly, RI (0.71 ± 0.06 vs 0.68 ± 0.08, p = 0.07), they did not differ in values of blood pressure and pulse pressure.
By the use of the Spearman’s rank correlation, an association between HbA1c and RI (Fig. 2), IMT-CCA (Fig. 3) and the age was found (Table 2).
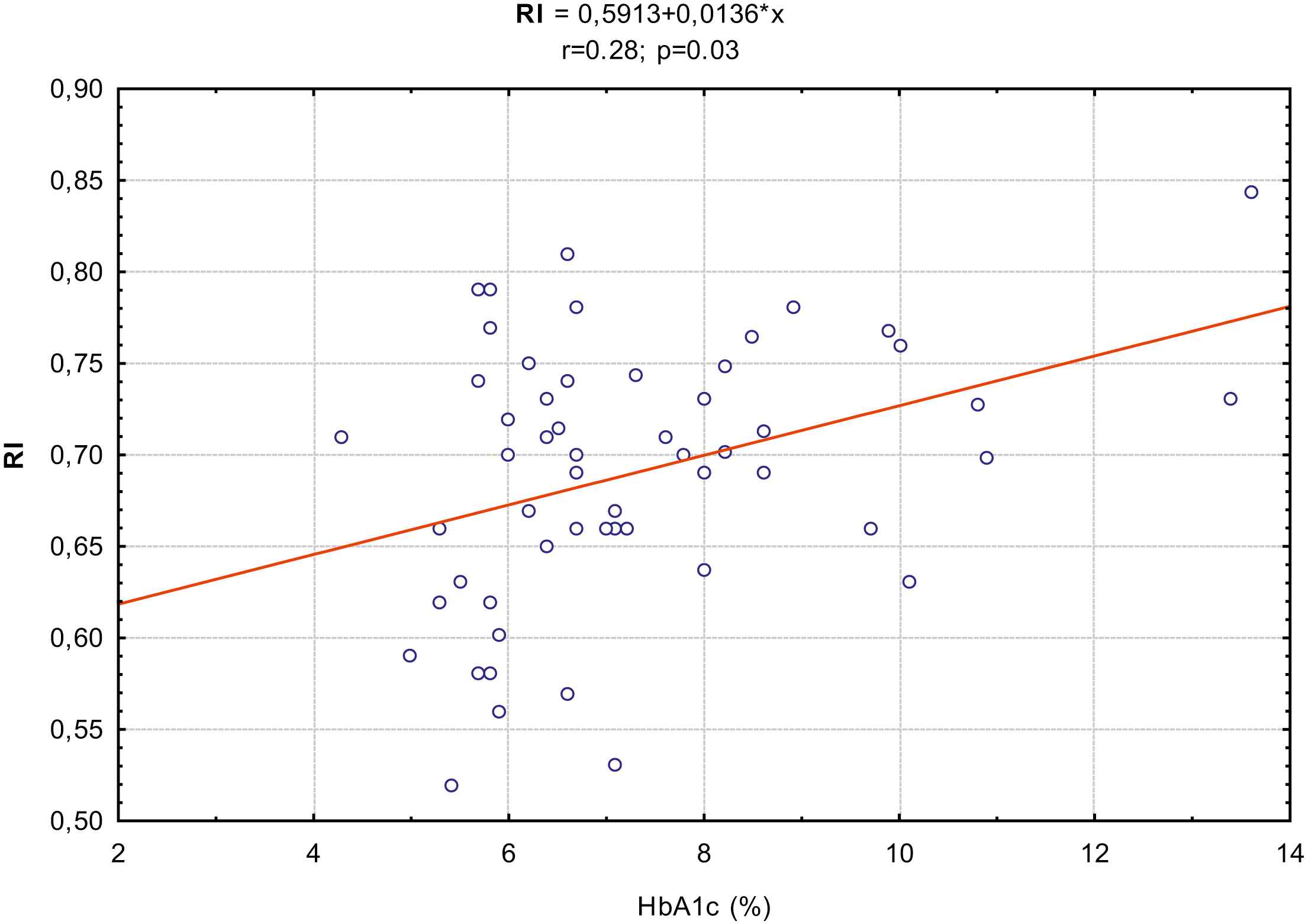
Relationship between HbA1c concentration and RI in common carotid artery.
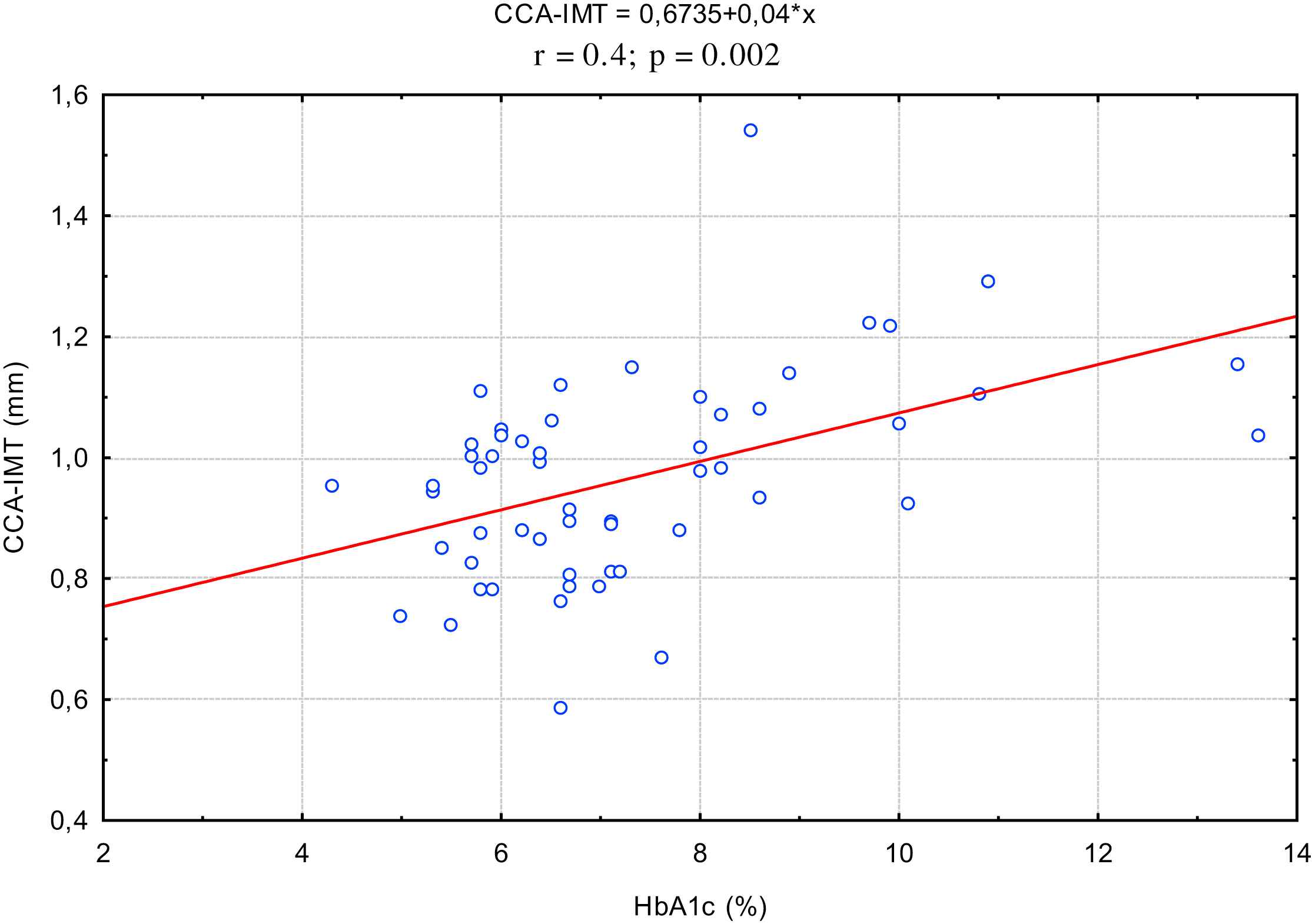
Relationship between HbA1c concentration and intima-media thickness of common carotid artery.
| Correlation coefficient (r; p) | |
|---|---|
| HbA1c – RI | 0.28; p = 0.03 |
| HbA1c – IMT-CCA | 0.4; p = 0.002 |
| HbA1c – age | 0.38; p = 0.002 |
HbA1c – glycated hemoglobin, RI – resistive index, IMT-CCA – common carotid artery intima-media thickness.
Correlation between HbA1c and RI, IMT-CCA and the age.
The whole study group was divided, independently of the presence of diabetes, into three subgroups corresponding to the tertiles of HbA1c levels: tertile I included 19 persons with HbA1c < 6.21%, tertile II included 18 persons with HbA1c between 6.2 and 7.59% and tertile III consisted of 19 persons with HbA1c ≥ 7.6%. One-way ANOVA test revealed that subjects with higher HbA1c were significantly older (p for trend 0.039) and had significantly higher IMT-CCA (p for trend 0.009) and higher RI (p for trend 0.045).
An increase in RI was observed along with an increase in HbA1c (Table 3) and in persons in I tertile amounted to 0.663 ± 0.08, in II tertile – 0.687 ± 0.07, and in III tertile – 0.720 ± 0.05. In post-hoc analysis RI was significantly higher in persons with HbA1c ≥ 7.6% than in persons with HbA1c < 6.2% (p = 0.03).
| HbA1c tertiles | CCA-IMT (mm) (mean ± SD) | p | RI (mean ± SD) | p | ||
|---|---|---|---|---|---|---|
| For trend | 0.009 | For trend | 0.04 | |||
| <6.21% | 0.923 ± 0.11 | I vs II | ns | 0.663 ± 0.08 | I vs II | ns |
| 6.2–7.59% | 0.891 ± 0.14 | II vs III | 0.002 | 0.687 ± 0.07 | II vs III | ns |
| ≥7.6% | 1.075 ± 0.18 | I vs III | 0.008 | 0.720 ± 0.05 | I vs III | 0.03 |
Mean values of carotid intima-media thickness and resistive index in HbA1c tertiles and results of post-hoc analysis.
In contrast, IMT-CCA in persons with HbA1c < 6.21% and in persons with HbA1c between 6.2 and 7.59% was similar and amounted to 0.923 ± 0.11 mm and 0.891 ± 0.14 mm respectively, and in persons with HbA1c ≥ 7.6% – 1.075 ± 0.18 mm (Table 3). In the Tukey’s test mean values of IMT-CCA in I and II tertile were significantly lower in comparison with values in III tertile (I vs III p = 0.008 and II vs III p = 0.002).
On multiple regression analysis, to which RI as a dependent variable, and the age, sex, BMI, cigarette smoking, presence of diabetes, duration of arterial hypertension, blood cholesterol concentration, treatment with ACEI, calcium channel blockers, beta blockers, SBP, DBP, heart rate and HbA1c as operands were included, the significant relationship between RI and SBP (β = 0.696, p = 0.0006) and DBP (β = −0.618, p = 0.003), as well as between RI and HbA1c was found (β = 0.279, p = 0.04). If in the model SBP and DBP were replaced with PP, then relationship between RI and PP (β = 0.450, p = 0.0009) was statistically significant and between RI and HbA1c (β = 0.292, p = 0.03) was observed.
On the second model of multiple regression analysis, to which IMT-CCA as a dependent variable and the age, sex, body mass index (BMI), cigarette smoking, presence of diabetes, blood cholesterol concentration, treatment with ACEI, calcium channel blockers, beta blockers, SBP, DBP and HbA1c as operands were included, the statistically significant relationship between IMT-CCA and the age (β = 0.343, p = 0.04), SBP (β = 0.430, p = 0.03) and HbA1c (β = 0.369, p = 0.01) was observed. If in the model SBP and DBP were replaced with PP, then relationship between IMT-CCA and PP (β = 0.341, p = 0.01) and between IMT-CCA and HbA1c (β = 0.354, p = 0.01) was also statistically significant.
Discussion
Both, RI as a hemodynamic parameter, and IMT as a morphological one, are associated with decreased arterial wall elasticity and distensibility and with development of atherosclerosis. Intima-media thickness of carotid artery has been suggested as a prognostic index for the increased incidence of myocardial infarction and stroke.4,6–13 On the contrary there are only few studies taking RI as a prognostic index into consideration. Nakatou et al. evaluating RI in carotid arteries in type 2 diabetic patients, proved usefulness of RI, as well as IMT in estimating the risk of previous cerebral infarction.11 Lee et al. in a Taiwanese population with essential hypertension revealed a correlation between RI of a carotid artery and the risk of coronary heart disease, which was comparable to the well-known correlation between carotid IMT and the cardiovascular risk.23 Frauchiger et al. recognized RI of common and internal carotid arteries (CCA and ICA) as markers of atherosclerosis comparable to IMT, although a correlation between RI ICA and IMT was greater than that between RI CCA and IMT.24 Resistive index of ICA was also revealed as a reliable marker of cardiovascular morbidity and mortality comparable to IMT in research of Staub et al.25
The relationship between many cardiovascular risk factors and increased IMT has been proved.26 We showed in our study that factors influencing independently IMT-CCA in patients treated for arterial hypertension are the age, HbA1c concentration, value of systolic blood pressure and pulse pressure. An independent relationship between IMT and HbA1c in middle aged patients suffering from diagnosed or undiagnosed diabetes mellitus was also confirmed by Selvin et al.27 There has been proved the relationship between carotid IMT and the span of diabetes mellitus. In this study IMT was greater in patients with a history of diabetes mellitus more than two years than in the newly diagnosed diabetic patients. Subjects with a higher HbA1c, compared to those with the lower HbA1c had slightly but non-significantly increased carotid IMT.28 In the ARIC study (Atherosclerosis Risk in Communities) population increase in HbA1c concentration in non-diabetic subjects was associated with significant increase in risk of coronary heart disease.29 Strong relationship between dysglycaemia and atherosclerosis, independent of the presence or absence of diabetes was revealed by Gertstein et al.30 These findings are important from clinical point of view.
Resistive index, similarly as IMT, correlates with the age and cardiovascular risk factors.3,24 Positive correlation between RI and HbA1c, SBP and pulse pressure and negative one between RI and diastolic blood pressure was revealed in examined population in our study on regression analysis, the same like in Ohta’s et al. research.31
A knowledge of factors influencing the development of atherosclerosis enable us to control the progression of this disease. The age is a non-modifiable parameter, but through the blood pressure and HbA1c control we can protect against the development of atherosclerosis and decrease a risk of cardiovascular events such as myocardial infarction and stroke.
HbA1c is a product of early glycation – the non-enzymatic reaction between glucose and proteins, known as Maillard, or browning reaction.32,33 Early glycation and oxidation processes result in formation of Schiff bases and Amadori products (HbA1c). Further glycation of proteins causes molecular rearrangements that lead to form advanced glycosylation endproducts (AGEs), which are nearly irreversible.33 The degree of non-enzymatic glycation is determined mainly by the glucose concentration and time of exposure. Therefore, AGEs accumulate continuously on long-lived vessel wall proteins with aging, and at an accelerated rate in diabetes.32 AGEs can alter properties of the large matrix proteins and cause cross-linking of collagen molecules, which may lead to loss of collagen elasticity and a subsequent reduction in arterial elasticity and flexibility during normal aging and in diabetes.32,33
In our study, both parameters, hemodynamic (RI) and morphological (IMT-CCA), grow along with increased HbA1c, which reflect a decrease in arterial wall elasticity and progression of atherosclerosis in uncontrolled diabetes. However after dividing subjects into thirds, RI, in comparison with IMT-CCA, increases along with the growth of HbA1c (Table 3). Furthermore, the increase in RI, although not significant between I and II as well as II and III tertile, can be easily seen already at low value of HbA1c, i.e. <6.21%. The lack of statistical significance between mean values of RI in subgroups (the significance for trend and between I and III tertile exists) may be a result of little size of subgroups as well as received treatment, which can limit the progression of adverse vessel changes. On the contrary a marked increase in intima-media thickness of common carotid artery can be noticed at higher values of HbA1c i.e. ≥7.4%. A conclusion arises that increase in RI as a marker of decreased extensibility and increased arterial resistance, appears earlier at given HbA1c concentrations, and this measurement is able to detect functional disorders associated with progression of atherosclerosis before evident increase in IMT can be observed. Manabe et al. came to similar conclusions while evaluating relationship between IMT and RI in common carotid artery and markers of inflammation such as IL-6 (interleukin – 6) and hs-CRP (high sensitivity C-reactive protein) in hypertensive patients.34 In their study RI was positively correlated with pulse pressure, IL-6 and hs-CRP, and IMT was positively correlated with age and pulse pressure, but not with IL-6 and hs-CRP.34 That difference may be time related. RI might refer to the present status of atherosclerotic change, as do inflammatory markers such as IL-6 and hs-CRP, being a marker of early atherosclerotic changes resulting in both, endothelium disorders and a decrease in arterial wall elasticity, and RI increase precedes morphological changes expressed by increased IMT. Intima-media thickening is a result of a prolonged influence of atherogenic factors on vessel wall, for example in the course of essential hypertension or diabetes. Normal or low RI may be a marker of healthy vessel wall contrary to normal IMT which may coexist with ultrastructural and functional changes in vessel wall, not detectable during ultrasound examination.
Resistive index is a parameter, which can be easily measured during ultrasound Doppler examination. When RI and IMT measurements are compared, the essential advantages of the former are the easier data acquisition by the use of a lower frequency probe, while the measurement of IMT requires the use of higher frequency probe. The RI evaluation is characterized by the tendency of lower interobserver and intraobserver variability, and the smaller side difference. The disadvantages comprise a dependency of RI measurement on heart rate and rhythm (in our study standardized according to heart rate on a regression model) and on a presence of stenosis before and behind the place of measurements. Then, a measurement of IMT can be made difficult by the segmental character of atherosclerosis, which provokes different localization of atherosclerotic plaques in patients. Taking into account advantages and simplicity of an evaluation, RI could be a useful marker of early atherosclerotic changes. However, the limitation of our study is its cross-sectional character and small number of examined patients, so our results should be confirmed in a larger prospective investigation.
In conclusion
Patients with hypertension and diabetes mellitus had significantly increased intima-media thickness and higher, but not significantly, RI. Concentration of HbA1c, next to the age and values of systolic and diastolic blood pressure, was independently associated with RI and IMT – parameters determining indirectly the degree of atherosclerosis of common carotid artery. Resistive index of CCA seems to be earlier marker of atherosclerotic changes than IMT. Proper control of blood pressure and glucose metabolism may prevent from the progression of atherosclerosis.
References
Cite this article
TY - JOUR AU - Anna Skalska AU - Ewa Klimek AU - Tomasz Grodzicki PY - 2010 DA - 2010/09/20 TI - Factors influencing hemodynamic and morphological indicators of carotid arteries atherosclerosis in treated hypertensive patients JO - Artery Research SP - 1 EP - 7 VL - 5 IS - 1 SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2010.08.001 DO - 10.1016/j.artres.2010.08.001 ID - Skalska2010 ER -