
Serum 25-Hydroxyvitamin D Deficiency and Insufficiency are Associated with Ankle-Brachial Index but not Arterial Stiffness in an Elderly Community-dwelling Chinese Population
These authors contributed equally to this study.
- DOI
- 10.2991/artres.k.191203.001How to use a DOI?
- Keywords
- 25-Hydroxy-vitamin D; arterial stiffness; brachial-ankle pulse wave velocity (baPWV); ankle-brachial index (ABI)
- Abstract
Vitamin D deficiency may increase arterial stiffness, a sub-clinical symptom of Target Organ Damage (TOD). This study aimed to investigate the associations between total serum vitamin D level and arterial stiffness assessed by brachial-ankle Pulse Wave Velocity (baPWV) and atherosclerosis assessed by Ankle-Brachial Index (ABI) in a Chinese community-dwelling elderly cohort. About 175 elderly participants (91 males and 84 females) were recruited. The levels of total serum 25-hydroxyvitamin D [25(OH)D], blood glucose, lipids and pressure were determined with clinical tests. We found 87.4% of elderly Chinese showed vitamin D deficiency (<20 ng/mL) and insufficiency (21–29 ng/mL). For these patients, the total 25(OH)D was positively correlated with right (r = 0.230, p = 0.004) and left ABI (r = 0.212, p = 0.008), whereas there was no correlation with right and left baPWV (r = −0.136 and −0.137, p = 0.092 and 0.089, respectively). In univariate linear regression, total serum 25(OH)D was positively associated with left and right ABI (p < 0.05). Multivariate regression suggested total serum 25(OH)D was independently correlated with the left and right ABI with adjustment for sex, age and Diastolic Blood Pressure (DBP). No significant association between total serum 25(OH)D level and baPWV was found. The study suggested that serum total 25(OH)D may be favorably associated with ABI in the elderly population with vitamin D deficiency and insufficiency; however, it may not correlated with arterial stiffness measured by baPWV. More prospective larger scale studies are warranted to validate these findings.
- Copyright
- © 2019 Association for Research into Arterial Structure and Physiology. Publishing services by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Vitamin D is an essential nutrient for the human body and the blood 25-hydroxyvitamin D [25(OH)D] level has been widely recognized as the biomarker of vitamin D status [1]. In Chinese, vitamin D deficiency is very common, especially in elderly individuals [2]. Recently, epidemiological studies have investigated that vitamin D deficiency may increase the risks of many chronic diseases including metabolic syndrome [1], diabetes [3] and Cardiovascular Diseases (CVD) [2–4]. In addition, several studies have reported that the serum 25(OH)D level was inversely correlated with the low density lipoprotein cholesterol (LDL-c) and triglycerides levels [5,6] and arterial stiffness [7–10]. Elderly people are at high risk of vitamin D deficiency, which may be due to decreased outdoor activities, inadequate food intake, poor intestinal absorption and decreased renal synthesis, which may underlie the increased risk of age-related chronic diseases in the population.
Age-related arterial stiffness is considered to be a degenerative disease, which is a common disorder in cardiovascular pathophysiology [11] and predisposing the elderly to increased risk of CVD. Noninvasive arterial stiffness measurement can be used to obtain additional information for early vascular aging, generally manifest by increased Systolic Blood Pressure (SBP) and pulse pressure in the population [12,13]. Carotid-femoral Pulse Wave Velocity (cfPWV) is considered as a golden standard measure of aortic stiffness and it is a cumulative measure of the damaging effects of cardiovascular risk factors on the arterial wall along with aging, especially in persons over 40 years of age [14]. We previously showed that cfPWV itself can be considered as an index of Target Organ Damage (TOD) [15]. Brachial-ankle PWV (baPWV) is robustly correlated with cfPWV, which can serve as a biomarker of arterial aging [16] in predicting CVD events and mortality [17]. Ankle-Brachial Blood Pressure Index (ABI) measurement is an accurate and noninvasive measurement in diagnosing peripheral arterial diseases including arterial stenosis and obstruction, and it is an independent predictor for cardiovascular risk [18]. Both measures were regarded as noninvasive biomarkers of subclinical TOD in the elderly by the ESH/ESC guidelines in the management of hypertension [19]. Although many investigations have examined the relationships between status of vitamin D and arterial stiffness measured by baPWV, the results are controversial [20–22]. Several cross-sectional studies and prospective studies had demonstrated that vitamin D deficiency and insufficiency was significantly associated with arterial stiffness [7–10]; however, other studies reported no significant association between vitamin D status and arterial stiffness. To date, there are relatively few studies that focus on the relationships between total vitamin D and baPWV and ABI in the elderly, with inconclusive results [8,10]. Therefore, we aimed to investigate the relationships between total serum vitamin D level and arterial stiffness assessed by baPWV and atherosclerosis assessed by ABI in a Chinese community-dwelling elderly cohort.
2. PARTICIPANTS AND METHODS
2.1. Study Population
A total of 175 elderly participants (age 60–100 years) aged 60 years and older who received a routine physical examination in the Chronic Disease Detection and Management Department of Xuhui Hospital between 2016 and 2017 were recruited. Main exclusion criteria were those participants with renal insufficiency (blood creatinine level > 180 µmol/L), presence of a malignant disease and had taken vitamin D supplements during the past 6 months. Forty subjects were excluded from the analysis because the 25(OH)D levels were not measured. The number of participants included in the present analysis was 175 (91 males and 84 females). Body height and weight were measured without shoes using a portable stadiometer (TCS-150, Shanghai Dongfang Scales Co., Ltd., China). BMI was calculated as the weight in kilograms divided by height in meters squared (kg/m2). The basic information of the patients was extracted from the participant’s medical records. All subjects provided written informed consent and the Ethics Committee of Ruijin Hospital North, Shanghai, approved the study protocol.
2.2. Laboratory Analysis
The levels of total 25(OH)D (D2 and D3) were measured with a Shimadzu series HPLC (Shimadzu Corporation, Japan) instrument connected to an API 5500 LC-MS/MS system (Applied Biosystems Inc., USA). The intraassay Coefficient of Variation (CV) was <5.0% and the interassay CV was <12.0%. Vitamin D insufficiency was defined as a serum 25(OH)D level of 21–29 ng/mL and Vitamin D deficiency was defined as a serum 25(OH)D level <20 ng/mL according to the guidelines [23]. The biochemical tests including serum total cholesterol, High Density Lipoprotein Cholesterol (HDL-c), triglycerides, blood glucose, serum creatinine and calcium were evaluated in routine laboratory tests.
2.3. Indices of Arterial Stiffness and Atherosclerosis
Noninvasive measurements of peripheral Blood Pressure (BP) and PWV were performed in the supine position using the Omron device (BP-203RPEIII VP-1000, Kyoto, Japan). After the subject had rested at least 10 min in the supine position, the pressure cuffs were wrapped on both upper arms and ankles. The device simultaneously and automatically measured blood in both ankles and upper arms. ABI was shown by the device as the ratio of the systolic blood pressures at the ankle to the systolic blood pressures in the upper arm (brachial). ABI value of 0.9–1.2 was considered normal with ABI ≤ 0.9 indicating arterial disease [24,25].
2.4. Statistical Analysis
The characteristics of the study participants were presented as the median and the Interquartile Range (IQR) or the number of participants and the corresponding proportion. The correlation between the variants was determined with Pearson’s coefficient of correlation. The relationships between the total 25(OH)D levels and arterial stiffness values of the participants were evaluated using univariate linear models. The multiple linear regression model was applied to determine whether the serum 25(OH)D was independently associated with arterial stiffness in the participants. All analyses were performed using R software (version 3.3.1, The R Foundation, Vienna, Austria) and related packages (www.r-project.org). A two-sided p < 0.05 was considered statistically significant.
3. RESULTS
3.1. Characteristics of Participants
The 175 participants included 91 (52%) males and 84 (48%) females. The age of participants ranged from 60 to 100 years old with a median value of 87 years. The BMI of the participants ranged from 15.6 to 37.2 kg/m2 with the mean value of 24.5 kg/m2 (Table 1). Of all participants, 20 (11.4%) had sufficiency serum 25(OH)D level, while 155 (88.6%) had insufficiency (20–29 ng/mL) and deficiency (<20 ng/mL) serum 25(OH)D level. Females had higher serum 25(OH)D, total triglycerides, HDL-c and LDL-c levels compared with males, but males had higher creatinine levels than females. Similar results were found in those participants with insufficiency and deficiency serum 25(OH)D level (Table S1). Compared with participants with sufficiency serum 25(OH)D, the age was older and the serum calcium level was higher in participants with vitamin D deficiency and insufficiency (Table S2).
| Characteristics | Median (IQR) (n = 175) | Male (n = 91) | Female (n = 84) | p-value |
|---|---|---|---|---|
| Age (years) | 87 (73–91) | 85.8 ± 8.7 | 78.1 ± 11.7 | <0.001 |
| BMI (kg/m2) | 24.52 (22.28–26.88) | 24.5 ± 3.1 | 24.6 ± 3.7 | 0.856 |
| Fasting glucose (mmol/L) | 8.6 (6.4–10.8) | 9.1 ± 3.7 | 9.9 ± 4.4 | 0.300 |
| Total cholesterol (mmol/L) | 4.39 (3.55–5.14) | 4.0 ± 1.0 | 4.8 ± 1.1 | <0.001 |
| HDL-c (mmol/L) | 1.1 (1.0–1.4) | 1.0 ± 0.3 | 1.2 ± 0.3 | <0.001 |
| LDL-c (mmol/L) | 2.32 (1.77–2.93) | 2.2 ± 0.7 | 2.6 ± 0.8 | 0.001 |
| Total triglyceride (mmol/L) | 1.24 (0.95–1.69) | 1.3 ± 0.5 | 1.6 ± 1.0 | 0.006 |
| Calcium (mmol/L) | 2.3 (2.2–2.4) | 2.3 ± 0.1 | 2.3 ± 0.1 | 0.59 |
| 25(OH)D (ng/mL) | 19.0 ± 9.2 | 17.5 ± 8.0 | 20.7 ± 10.0 | 0.019 |
| Creatinine (µmol/L) | 68 (54–86) | 88.0 ± 29.2 | 60.3 ± 15.8 | <0.001 |
| Left SBP (mmHg) | 137 (122–150) | 136.9 ± 21.3 | 138.3 ± 18.8 | 0.642 |
| Left DBP (mmHg) | 75 (67–84) | 75.7 ± 11.0 | 75.9 ± 11.4 | 0.902 |
| Right SBP (mmHg) | 138 (124–151) | 138.6 ± 20.5 | 140.0 ± 18.3 | 0.642 |
| Right DBP (mmHg) | 77 (68–85) | 77.2 ± 11.6 | 76.5 ± 11.6 | 0.643 |
| Left baPWV (cm/s) | 1868 (1681–2104) | 1924.9 ± 398.4 | 1922.4 ± 450.6 | 0.969 |
| Right baPWV (cm/s) | 1839 (1649–2077) | 1891.7 ± 380.8 | 1887.1 ± 426.1 | 0.940 |
| Left ABI | 1.11 (1.03–1.17) | 1.0 ± 0.1 | 1.0 ± 0.2 | 0.806 |
| Right ABI | 1.11 (1.03–1.16) | 1.1 ± 0.2 | 1.1 ± 0.2 | 0.052 |
| Season (Spring/Summer/Autumn/Winter) | 26/112/23/14 | 16/55/12/8 | 10/57/11/6 | 0.689 |
BMI, body mass index; HDL-c, high density lipoprotein cholesterol; LDL-c, low density lipoprotein cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure; baPWV, brachial-ankle pulse wave velocity; ABI, ankle brachial index.
Baseline characteristics of the participants (N = 175)
3.2. Correlation between Serum 25(OH)D Level and Arterial Stiffness in the Elderly Population
Correlation between the variables and the ABI and baPWV is shown in Table S3. The serum 25(OH)D level was significantly correlated with the right ABI level (p = 0.025) but not the left ABI (p = 0.076) of the participants. No correlation with baPWV was found (Table S3). In the stratification study by serum 25(OH)D level, we found that the total serum 25(OH)D level showed a significant positive correlation with the right ABI (r = 0.230, p = 0.004) and the left ABI (r = 0.212, p = 0.008) in participants with insufficiency and deficiency serum 25(OH)D level; however, there was no significant correlation between serum 25(OH)D and baPWV (Figure 1). In addition, the total serum 25(OH)D level was negatively correlated with age (r = −0.364, p < 0.001) and total cholesterol (r = 0.161, p = 0.048) and positively correlated with serum calcium level (r = 0.181, p = 0.0039).

Correlation matrix between the variables in participants with vitamin D insufficiency and deficiency level. The numbers in the squares and colored circles represent the Spearman’s r values between the variants.
3.3. Univariate Regression Analysis of ABI and baPWV
In participants with deficiency and insufficiency vitamin D level, the univariate linear regression suggested that the total serum 25(OH)D level was positively associated with right ABI (standardized β = 0.230, p = 0.004; Figure 2a) and left ABI (standardized β = 0.212, p = 0.008; Figure 2b), whereas the total 25(OH)D level was not significantly associated with the left or right baPWV in individuals with vitamin D deficiency and insufficiency (Table 2 and Figure 2c and d). Age, SBP and DBP were positively related to right and left baPWV (Table 2). For participants with sufficiency, the serum 25(OH)D level was not significantly associated with the ABI or baPWV (Table S4).
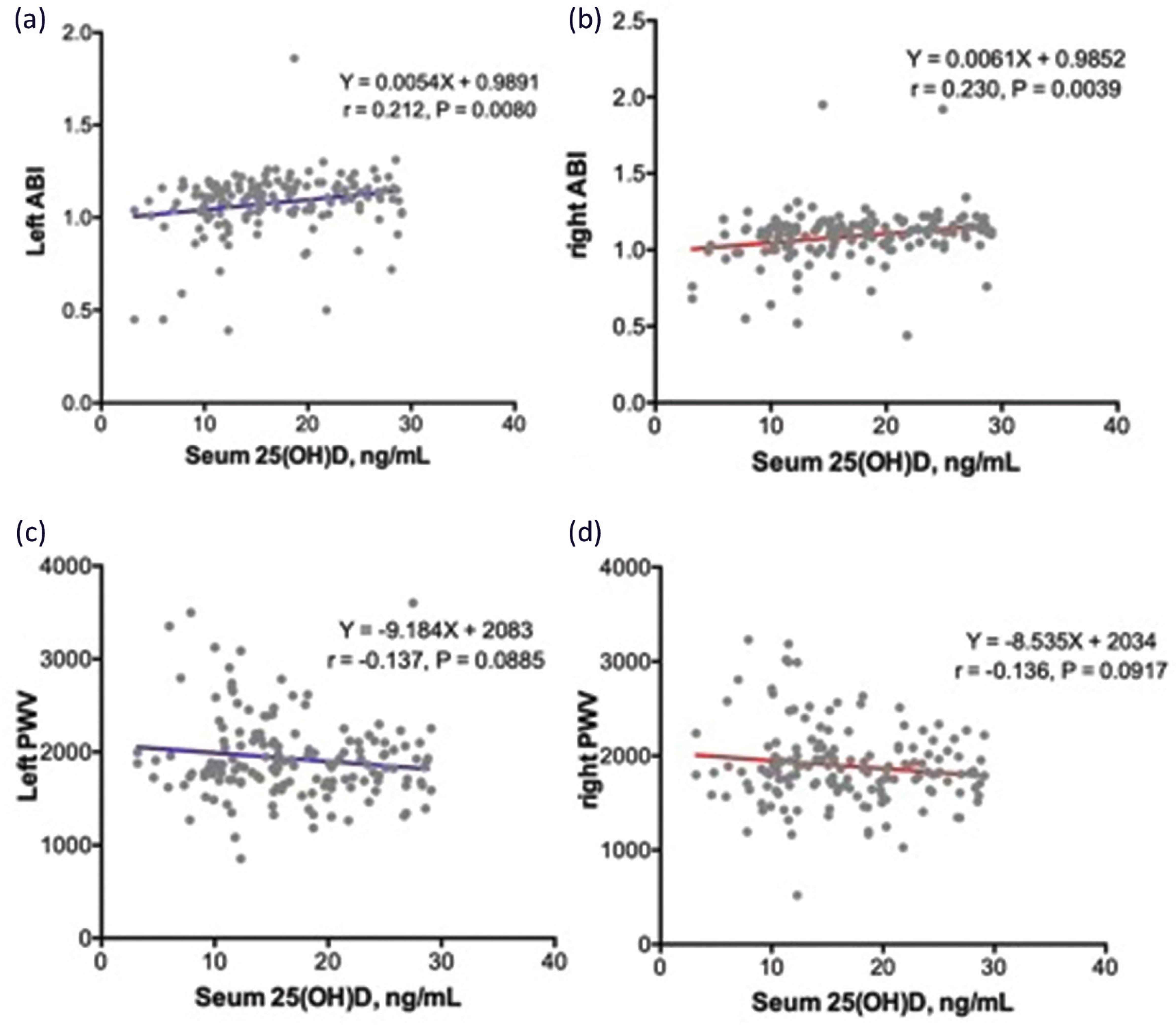
The correlation between serum 25(OH)D concentrations and the left (a) or (b) right ABI in participants with vitamin D deficiency and insufficiency, and its association with left (c) or right (d) baPWV level.
| Characteristics | Left ABI | Right ABI | Left baPWV | Right baPWV | ||||
|---|---|---|---|---|---|---|---|---|
| Standardized β (se) | p-value | Standardized β (se) | p-value | Standardized β (se) | p-value | Standardized β (se) | p-value | |
| Age (years) | −0.111 (0.080) | 0.170 | −0.158 (0.080) | 0.049 | 0.281 (0.078) | <0.001 | 0.291 (0.077) | <0.001 |
| BMI (kg/m2) | −0.001 (0.083) | 0.991 | 0.044 (0.083) | 0.599 | −0.002 (0.083) | 0.978 | −0.032 (0.083) | 0.697 |
| Sex | −0.025 (0.162) | 0.876 | −0.315 (0.160) | 0.051 | 0.051 (0.162) | 0.755 | 0.039 (0.162) | 0.812 |
| Fasting glucose (mmol/L) | −0.027 (0.093) | 0.769 | 0.082 (0.091) | 0.373 | −0.282 (0.082) | 0.001 | −0.254 (0.088) | 0.004 |
| Vitamin D (ng/mL) | 0.212 (0.079) | 0.008 | 0.230 (0.079) | 0.004 | −0.137 (0.080) | 0.089 | −0.136 (0.080) | 0.092 |
| Total cholesterol (mmol/L) | −0.067 (0.082) | 0.415 | −0.023 (0.082) | 0.780 | −0.110 (0.082) | 0.180 | −0.154 (0.081) | 0.059 |
| HDL-c (mmol/L) | 0.108 (0.082) | 0.191 | −0.032 (0.083) | 0.696 | 0.009 (0.083) | 0.911 | 0.009 (0.083) | 0.909 |
| LDL-c (mmol/L) | −0.060 (0.083) | 0.471 | 0.000 (0.083) | 0.997 | −0.113 (0.082) | 0.170 | −0.174 (0.081) | 0.034 |
| Triglycerides (mmol/L) | −0.088 (0.082) | 0.285 | 0.040 (0.082) | 0.625 | −0.123 (0.082) | 0.133 | −0.110 (0.082) | 0.178 |
| Calcium (mmol/L) | −0.060 (0.093) | 0.519 | 0.206 (0.084) | 0.016 | 0.125 (0.091) | 0.173 | 0.138 (0.090) | 0.130 |
| Creatinine (µmol/L) | −0.093 (0.081) | 0.253 | 0.032 (0.081) | 0.699 | 0.006 (0.081) | 0.940 | −0.009 (0.081) | 0.913 |
| SBP (mmHg) | −0.097 (0.081) | 0.232 | 0.078 (0.081) | 0.334 | 0.617 (0.064) | <0.001 | 0.585 (0.066) | <0.001 |
| DBP (mmHg) | 0.012 (0.081) | 0.881 | 0.103 (0.080) | 0.203 | 0.445 (0.073) | <0.001 | 0.391 (0.074) | <0.001 |
| PP (mmHg) | −0.161 (0.080) | 0.047 | 0.025 (0.081) | 0.754 | 0.571 (0.067) | <0.001 | 0.537 (0.068) | <0.001 |
BMI, body mass index; HDL-c, high density lipoprotein cholesterol; LDL-c, low density lipoprotein cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure; PP, pulse pressure; baPWV, brachial-ankle pulse wave velocity; ABI, ankle brachial index.
Univariate regression analysis of clinical characteristics and blood vessel properties in vitamin D deficiency and insufficiency (N = 155)
3.4. Multivariate Regression Analysis in the Elderly Population with Vitamin D Deficiency and Insufficiency
In multivariate linear regression analysis of individuals with vitamin D deficiency and insufficiency, we found the total 25(OH)D level was positively associated with left ABI (standardized β = 0.195, p = 0.025) and right ABI (standardized β = 0.194, p = 0.022) in participants with serum 25(OH)D level <30 ng/mL with the adjustments of confounding factors including age, sex and DBP. No correlation was noticed in participants with sufficiency serum 25(OH)D level (Table 3). For baPWV, serum 25(OH)D was not associated with baPWV when adjusted for age, sex and DBP (Table 4). Age and DBP were independently associated with left baPWV (standardized β = 0.473, p < 0.001, standardized β = 0.552, p < 0.001, respectively) and right baPWV (standardized β = 0.502, p < 0.001, standardized β = 0.527, p < 0.001, respectively).
| Left ABI | Right ABI | |||
|---|---|---|---|---|
| Standardized β (se) | p-value | Standardized β (se) | p-value | |
| Vitamin D ≥ 30 ng/mL (N = 20) | ||||
| Sex | −0.675 (0.540) | 0.234 | −0.415 (0.353) | 0.259 |
| Age (years) | −0.885 (0.244) | 0.003 | −0.500 (0.168) | 0.010 |
| Vitamin D (ng/mL) | 0.204 (0.323) | 0.540 | 0.280 (0.244) | 0.232 |
| DBP (mmHg) | 0.203 (0.249) | 0.429 | 0.043 (0.198) | 0.833 |
| Vitamin D < 30 ng/mL (N = 155) | ||||
| Sex | −0.067 (0.171) | 0.697 | −0.422 (0.165) | 0.011 |
| Age (years) | −0.043 (0.094) | 0.646 | −0.138 (0.092) | 0.134 |
| Vitamin D (ng/mL) | 0.195 (0.086) | 0.025 | 0.194 (0.084) | 0.022 |
| DBP (mmHg) | 0.002 (0.083) | 0.983 | 0.063 (0.081) | 0.442 |
DBP, diastolic blood pressure; ABI, ankle-brachial index.
Linear regression analysis of associations between serum vitamin D level and ABI stratified by vitamin D level
| Left baPWV (cm/s) | Right baPWV (cm/s) | |||
|---|---|---|---|---|
| Standardized β (se) | p-value | Standardized β (se) | p-value | |
| Vitamin D ≥ 30 ng/mL (N = 20) | ||||
| Sex | −0.318 (0.369) | 0.405 | −0.112 (0.394) | 0.780 |
| Age (years) | 0.140 (0.167) | 0.418 | 0.411 (0.188) | 0.046 |
| Vitamin D (ng/mL) | −0.324 (0.221) | 0.167 | −0.355 (0.250) | 0.200 |
| DBP (mmHg) | 0.316 (0.170) | 0.086 | 0.210 (0.220) | 0.356 |
| Vitamin D < 30 ng/mL (N = 155) | ||||
| Sex | 0.341 (0.138) | 0.015 | 0.389 (0.141) | 0.006 |
| Age (years) | 0.473 (0.076) | <0.001 | 0.502 (0.078) | <0.001 |
| Vitamin D (ng/mL) | 0.020 (0.070) | 0.778 | 0.042 (0.071) | 0.554 |
| DBP (mmHg) | 0.552 (0.067) | <0.001 | 0.527 (0.069) | <0.001 |
DBP, diastolic blood pressure; baPWV, brachial-ankle pulse wave velocity.
Linear regression analysis of associations between serum vitamin D level and baPWV stratified by vitamin D level
4. DISCUSSION
In the current study, we demonstrated that prevalence of vitamin D deficiency and insufficiency (<30 mg/ml) accounted for 88.6% in elderly Chinese subjects. The total serum 25(OH)D level was positively correlated with ABI in elderly people with vitamin D deficiency, whereas it was negatively associated with age. In addition, our results showed that the serum 25(OH)D level was not associated with the baPWV level in elderly Chinese. These results suggest that vitamin D may have preventive roles in peripheral vascular diseases.
Ankle-Brachial Blood Pressure Index is a widely-used index in the noninvasive assessment of peripheral vascular disease. Lower ABI value was correlated with arterial disease; however, as the stiff arteries produce elevated ankle blood pressure, higher ABI was usually found in patients with diabetes mellitus and it was associated with arterial calcification. Lower ABI reflects the burden of atherosclerosis on the vascular wall, which may lead to the increased cardiovascular disease morbidity and lower quality of life [25]. There is also a significant inverse correlation with intima-media thickness, a marker of sub-clinical TOD and preclinical atherosclerosis in elderly subjects [26]. In the present study, we found a significant positive relationship of serum 25(OH)D with ABI. Vitamin D deficiency has been recognized as a risk factor for CVD [27], and it had been widely recognized as an independent risk factor for atherosclerosis, peripheral artery disease [28] and arteriosclerosis. Previous studies have reported that vitamin D had a preventative role in patients with CVD [4], which may be due to vitamin D inhibiting the Renin-Angiotensin-Aldosterone System (RAAS) [20], modulating macrophage activity and cytokine production [29]. Low ABI has been reported to be associated with cardiovascular morbidity and mortality [30]. The total serum 25(OH)D decreased along with lower ABI in vitamin D deficient individuals, suggesting that vitamin D was associated with arterial atherosclerosis, which may underlie the increased risk of CVD in patients with lower serum 25(OH)D [20]. Moreover, we found that higher serum 25(OH)D level was correlated with increased serum calcium in the elderly population, and the higher calcium levels could contribute to vascular calcification which results in less distensible arteries. Interestingly, a cross-sectional study reported a strong inverse and independent association between dietary calcium intake and arterial stiffness in those with higher dietary vitamin D intake [31], which might be caused by the increased calcium absorption in population with higher vitamin D intake. Therefore, our findings suggest a potential mechanism that underlie the association of serum 25(OH)D deficiency and the increased vascular calcification in the elderly population.
Previous clinical studies and meta-analysis have reported that serum 25(OH)D level is inversely associated with arterial stiffness measured by baPWV, even in the elderly [8,10]. However, the value of left and right baPWV are expressed as average of bilateral baPWV measurement in assessing arterial stiffness in these studies [8,10], which may not accurately reflect the status of the baPWV of the participants. In our study, the value of right and left baPWV were calculated and applied in the analysis, which may underlie the inconsistent results with previous observational studies. Furthermore, there are several longitudinal studies on vitamin D that failed to show improvements in arterial stiffness with vitamin D supplementation [32,33], suggesting that vitamin D may have no significant influence on arterial stiffness. Other randomized controlled trails performed to date, show vitamin D had an effect on arterial stiffness, with a potential protective role interpreted by suppressing RAAS [34,35] and improving endothelial function [36]. Arterial stiffness measured by PWV is a powerful predictor in increasing cardiovascular mortality and morbidity mainly influenced by age and blood pressure [37]. Our population-based study has shown now an association between serum vitamin D and blood pressure and arterial stiffness measured by baPWV (mean value > 1880 cm/s), which is consistent with other cross-sectional studies [21,22].
There are several limitations to be acknowledged in the current study. First, the study was performed by cross-sectional design, and so provides the association of relationships instead of predictive values of vitamin D on the progression of arterial stiffness. Second, there is lack of data on history of medication and other previous disease status as factors that may confound the results of the current study. Third, the sample size of our study is relatively small and the age of the participants over 70 years old, which limits the findings applicable only to the elderly population. In particular, the small sample of the vitamin D sufficient individuals has the effect of reducing the power for comparison.
In conclusion, the present cross-sectional study suggested that serum 25(OH)D may be favorably related to ABI; however, serum 25(OH)D level is not related to arterial stiffness measured by baPWV, which is likely to be mainly mediated by age. Large-scale prospective studies are warranted to confirm these findings in future.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHOR’S CONTRIBUTION
JZ, PC and AA contributed in conception of the work. KQ and YH contributed in data curation. JZ and KQ contributed in drafting the work. KQ, YH, IT, MB and JZ contributed in formal analysis.
FUNDING
Project Supported by the
ACKNOWLEDGMENTS
We gratefully acknowledge the invaluable assistance of the physicians of the Department of Geriatric Medicine and Healthy Assessment Center, Ruijin Hospital North, Shanghai Jiaotong University School of Medicine, the study would not have been possible without their support.
SUPPLEMENTARY MATERIALS
Supplementary data related to this article can be found at
Footnotes
Peer review under responsibility of the Association for Research into Arterial Structure and Physiology
Data availability statement: The Numeric data used to support the findings of this study are restricted by the Ethics Committee of Ruijin Hospital North in order to protect PATIENT PRIVACY. Data are available from Junli Zuo ( zuo-junli@163.com ) for researchers who meet the criteria for access to confidential data.
REFERENCES
Cite this article
TY - JOUR AU - Junli Zuo AU - Kun Qian AU - Yan He AU - Isabella Tan AU - Mark Butlin AU - Alberto Avolio AU - Peizhan Chen PY - 2019 DA - 2019/12/17 TI - Serum 25-Hydroxyvitamin D Deficiency and Insufficiency are Associated with Ankle-Brachial Index but not Arterial Stiffness in an Elderly Community-dwelling Chinese Population JO - Artery Research SP - 113 EP - 119 VL - 25 IS - 3-4 SN - 1876-4401 UR - https://doi.org/10.2991/artres.k.191203.001 DO - 10.2991/artres.k.191203.001 ID - Zuo2019 ER -