
Vascular function is impaired early after the initiation of chronic cigarette smoking
- DOI
- 10.1016/j.artres.2009.06.025How to use a DOI?
- Keywords
- Cigarette smoking; Endothelial function; Reactive hyperemia; Vascular function
- Abstract
Background: The aim of this study was to assess resistance artery function in short-term chronic cigarette smokers and non-smoking control subjects.
Methods: Reactive hyperemia was assessed in 19 cigarette smokers (age 23±1 years) and 19 non-smokers (age 23±1 years).
Results: Cigarette smokers demonstrated a 23% lower peak forearm blood flow response compared with non-smokers (15.81±0.66 vs. 20.58±1.26mL/min/100mL, p<0.05) and a 22% lower area under the curve of the reactive hyperemia response (607±51.57 vs. 775±53.51mL/min/100mL×3min, p<0.05).
Conclusions: These results indicate that smoking-induced impairments of vascular function occur early after the initiation of chronic cigarette smoking.
- Copyright
- © 2009 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V.All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
Chronic cigarette smoking is a well-known cardiovascular disease risk factor and has been shown to cause pro-atherosclerotic changes to the vasculature.1 For example, cigarette smoke exerts atherogenic effects through chronic activation of pro-inflammatory cytokines and increased platelet adhesion and aggregation, as well as by promoting monocyte adhesion and transendothelial migration into the sub-intimal space.2 Moreover, dysfunction of the vascular endothelium, particularly impaired vasomotor regulation, has been shown to occur following several years of chronic cigarette smoking, independent of the transient effect of acute smoking.3,4
Although previous studies have demonstrated that a long history of chronic cigarette smoking (i.e. >15 pack years) impairs endothelial function in middle-aged and older adults, there is little information available concerning the influence of short-term chronic smoking (i.e. <5 pack years) on vascular function in young adults. Knowledge regarding the early effects of chronic smoking on cardiovascular health is important considering the increasing prevalence of smoking in college-aged individuals.5,6 Indeed, a recent survey indicated that approximately one-third of college students are current cigarette smokers.5 As a result, it is necessary to gain a greater understanding of the vascular damage being caused by cigarette smoking in young adults.
Therefore, the purpose of this investigation was to determine the effects of short-term chronic smoking on resistance artery vascular function of young cigarette smokers compared with age-matched non-smokers. We hypothesized that the forearm reactive hyperemia response would be blunted in young cigarette smokers compared with age-matched non-smokers.
Materials and methods
Subjects
Thirty eight college-aged men (cigarette smokers (CS) n=19 and non-smokers (NS) n=19) between the ages of 18 and 30 years participated in the study. A cigarette smoker was defined as an individual who smoked an average of at least 20 but no more than 250 cigarettes per week and had done so for a minimum of 2 years, but for no more than 5 years. Subjects in both groups were recreationally active, defined as participation in 20–40min of moderate physical activity 2–4 days/week. Exclusion criteria included known cardiovascular, pulmonary, or metabolic diseases including diabetes, medication use, and orthopedic problems that preclude treadmill walking or running. The CS and NS groups were matched for age, weight, and physical activity status. All subjects signed an institutionally approved informed consent prior to participating in any testing procedure. The study was approved by the Institutional Review Board in compliance with the Department of Health and Human Services Regulations for the Protection of Human Research Subjects.
Baseline measurements
Body weight was determined to the nearest 0.1kg on a calibrated digital scale, with height measured using a stadiometer. Body mass index (BMI) was calculated as weight (kg) divided by height (m) squared. Resting blood pressure (BP) was determined using the oscillometric technique over the brachial artery in accordance with American Heart Association guidelines, as established by the Council for High Blood Pressure Research.7 Smoking subjects refrained from smoking cigarettes for at least 12h prior to testing to rule out the influence of acute cigarette smoking.
Reactive hyperemia
Following 15min of supine rest, resting forearm blood flow (FBF) measurements were taken on the non-dominant arm using venous occlusion strain-gauge plethysmography (EC-6, D.E. Hokanson, Inc., Bellevue, WA) as described previously.8,9 Briefly, an inflatable cuff was placed around the upper arm, while another inflatable cuff was placed around the wrist to occlude hand circulation. A mercury-in-silastic strain-gauge was placed around the widest part of the forearm to measure changes in forearm volume resulting from changes in blood flow. One minute prior to FBF determination, the wrist cuff was inflated to 50mmHg above the systolic blood pressure (SBP) to exclude the hand circulation. FBF was determined by inflating the upper arm cuff to 40mmHg for 7s, followed by an 8-s deflation. The plethysmographic signal was transmitted to a Biopac digital recorder for determination of FBF (Biopac Systems, Inc., Santa Barbara, CA) and all testing and analyses were performed by the same technician. Resting forearm vascular conductance (FVC) was calculated as FBF/mean arterial pressure and expressed in the units mL/min/100mL tissue/100mmHg. Flow per 100mmHg was used so that FVC was quantitatively similar to the units for FBF.10
Reactive hyperemia was induced by inflating the upper arm cuff to 100mmHg above the resting SBP to occlude FBF for 5min. One minute prior to the release of the upper arm cuff, the wrist cuff was inflated to 50mmHg above the resting SBP. After release of the inflated upper arm cuff, forearm volume changes were recorded by the strain-gauge, using the above mentioned technique for 3min.9
Statistical analysis
Independent t tests were used to determine differences in baseline characteristics, resting FBF, peak reactive hyperemia (RH), and area under the curve (AUC) of RH above baseline FBF between CS and NS. Area under the curve of RH was calculated using the trapezoidal rule.11 The time-course of the RH response was analyzed using repeated measures analysis of variance, with post hoc independent t tests to determine differences in FBF at individual time points between groups. Statistical significance was set at p<0.05. SPSS (v. 13, Chicago, IL) was used for the analysis. All data are presented as mean±SEM.
Results
Subject characteristics
Descriptive statistics for the CS and NS groups are presented in Table 1. No differences in age, body height, body weight, BMI, or BP were found between the two groups. Cigarette smoking history is presented in terms of pack years (1 pack year was equivalent to 20 cigarettes smoked per day for 1 year). Smoking subjects reported an average smoking history of 1.6 pack years.
| Characteristic | Non-smokers (n=19) | Cigarette smokers (n=19) |
|---|---|---|
| Age (years) | 23±1 | 23±1 |
| Body height (cm) | 181.8±1.3 | 177.7±2.1 |
| Body weight (kg) | 79.7±2.5 | 78.4±3.7 |
| BMI (kg/m2) | 24.1±0.7 | 24.7±0.9 |
| SBP (mmHg) | 108±2 | 106±2 |
| DBP (mmHg) | 68±1 | 68±2 |
| MAP (mmHg) | 81.9±1.2 | 80.4±1.6 |
| Smoking history (pack years) | – | 1.6±0.3 |
| Resting FBF (mL/min/100mL tissue) | 2.86±0.2 | 2.85±0.2 |
| Resting FVC (mL/min/100mL tissue/100mmHg) | 3.47±0.26 | 3.58±0.26 |
BMI – body mass index, SBP – systolic blood pressure, DBP – diastolic blood pressure, MAP – mean arterial pressure, FBF – forearm blood flow, FVC – forearm vascular conductance. Values presented as mean±SEM.
Subject characteristics.
Reactive hyperemia
There were no differences in resting FBF or FVC between the groups (Table 1). The CS group demonstrated a 23% lower peak RH (15.81±0.66mL/min/100mL of tissue) compared with the NS group (20.58±1.26mL/min/100mL of tissue) (p<0.05) (Fig. 1). Similarly, the CS group demonstrated a 22% lower AUC of RH (607±52mL/min/100mL of tissue×3min) compared with the NS group (775±54mL/min/100mL of tissue×3min) (p<0.05) (Fig. 2). Additionally, FBF remained higher in NS compared to CS (p<0.05) until the 45s time point following cuff release (Fig. 3).
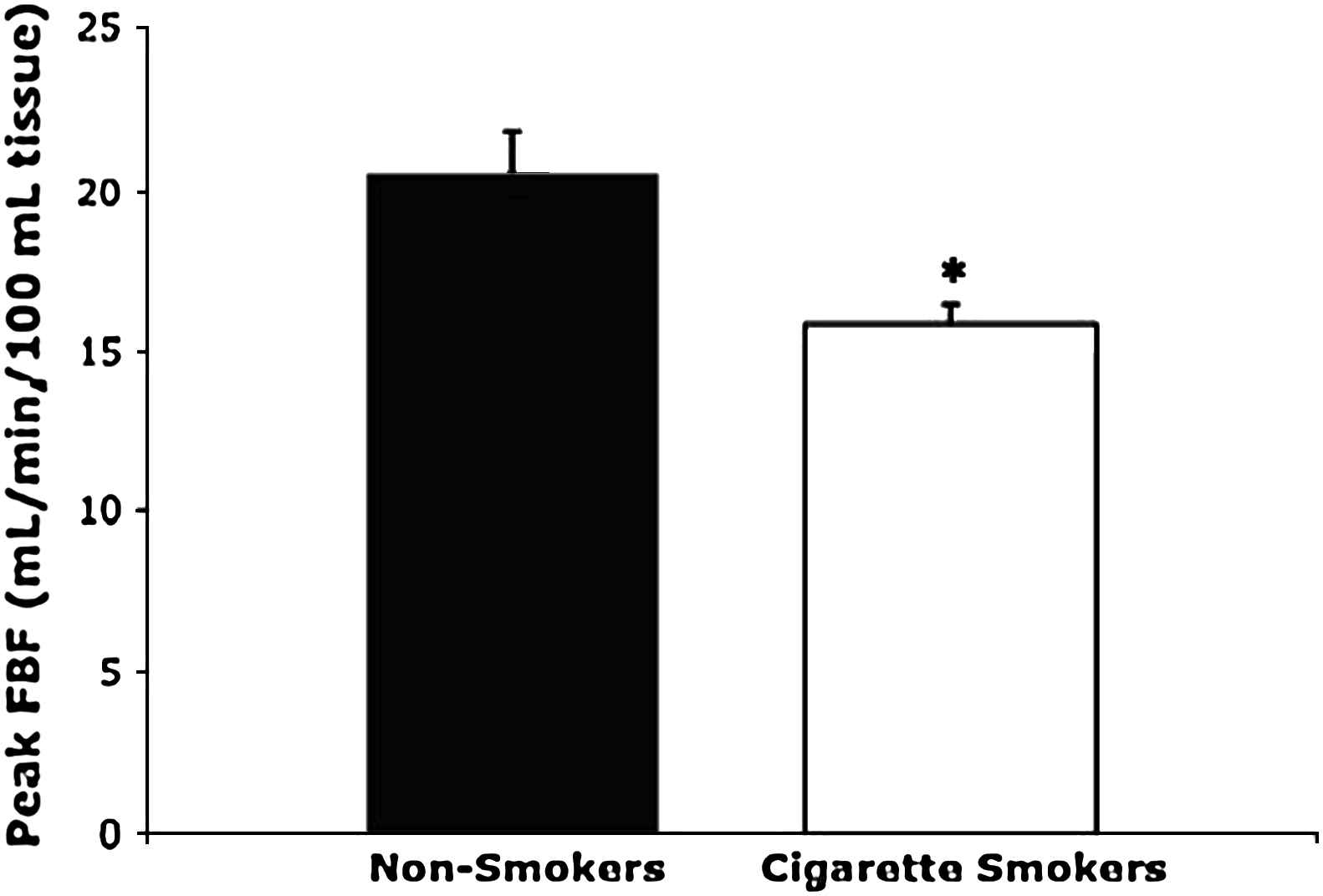
Peak reactive hyperemia. Peak FBF following cuff release in cigarette smokers and non-smokers. Values are mean±SEM. The cigarette smoking group had a significantly lower peak FBF during RH compared to the non-smoking group (p<0.05). *p<0.05 compared with non-smokers.
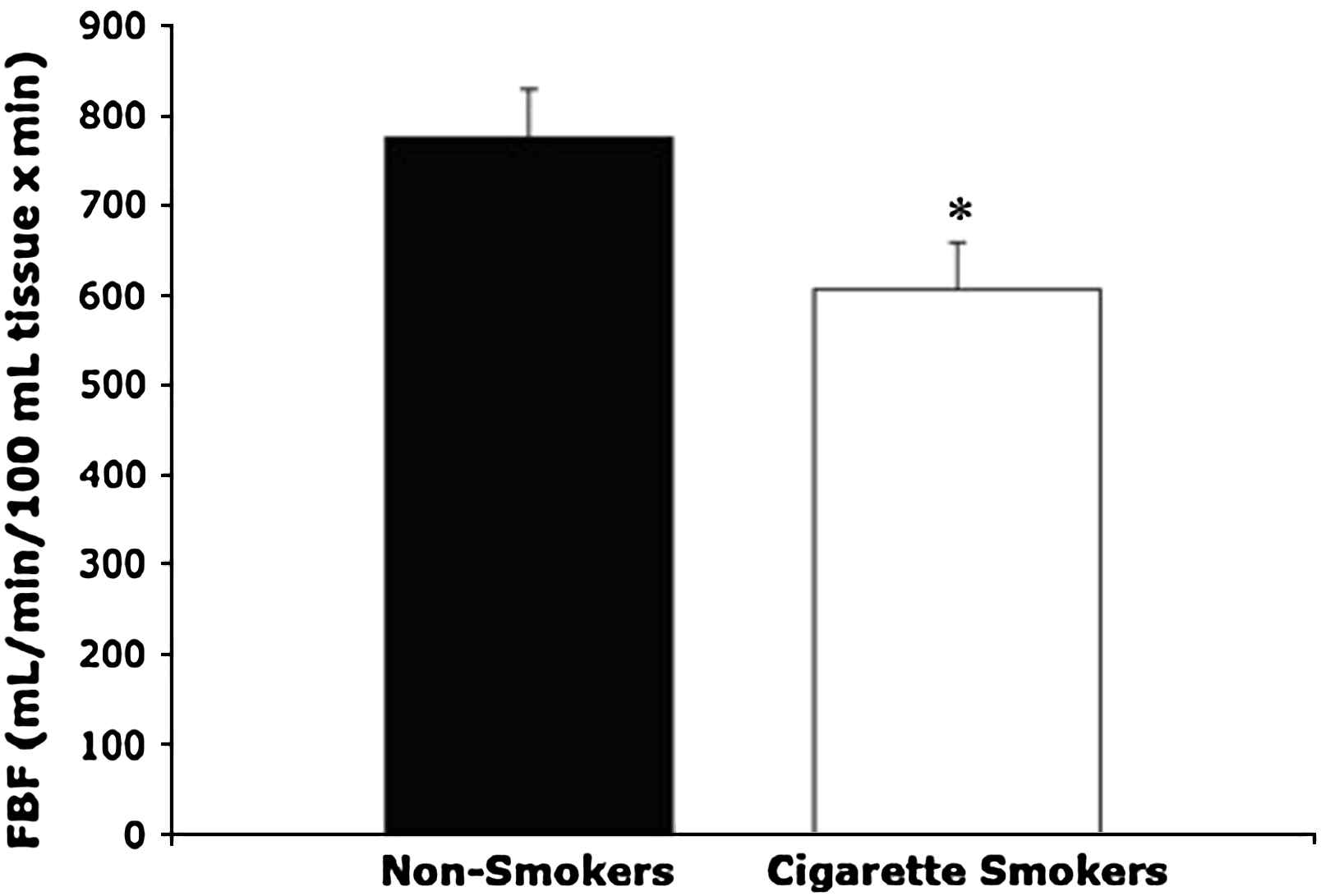
Incremental area under the curve of the reactive hyperemia response. Area under the curve (AUC) of FBF following cuff release in cigarette smokers and non-smokers. Values are mean±SEM. Compared with non-smokers, cigarette smokers had a lower AUC of the RH response (p<0.05). *p<0.05 compared with non-smokers.
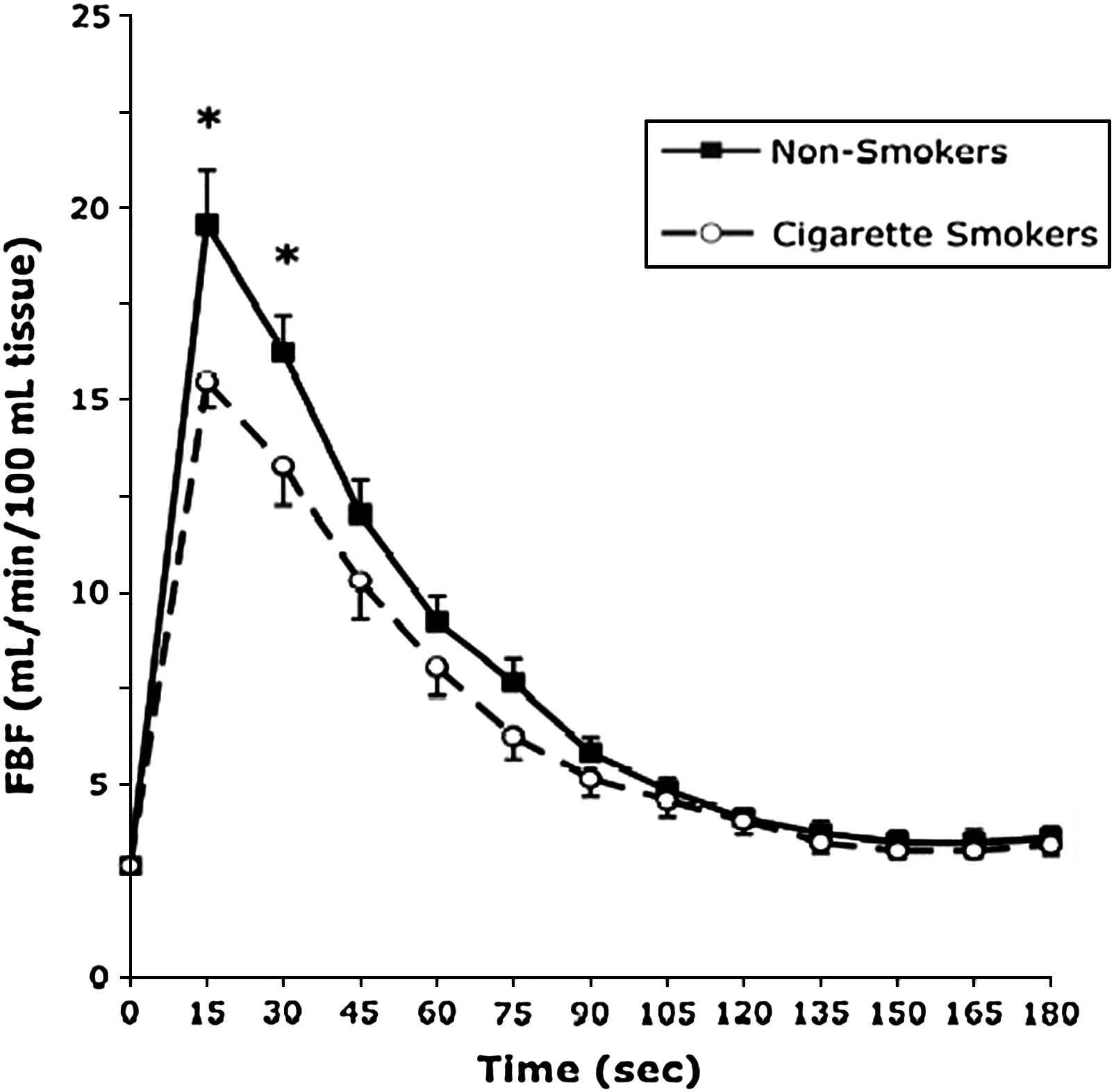
Reactive hyperemia response of cigarette smokers vs. non-smokers. FBF following cuff release in non-smokers compared to smokers. Values are mean±SEM. Cigarette smokers had significantly lower FBF compared with non-smokers at the 15s and 30s time points following RH (p<0.05). *p<0.05 compared with cigarette smokers.
Discussion
The primary novel finding of the present study is that the forearm reactive hyperemic response was significantly blunted in young cigarette smokers compared to age-matched non-smokers. Moreover, the total blood flow response (AUC) was markedly lower in young smokers. These data suggest that even a relatively short-term history of cigarette smoking is detrimental to vascular health in young men.
These results significantly extend previous findings that have shown that vascular dysfunction is associated with long-term chronic cigarette smoking.3,4,12 In middle-aged (54±7 years) long-term cigarette smokers, Zeiher et al.4 reported that smoking was associated with impaired endothelium-dependent coronary vasodilation regardless of the presence or absence of coronary atherosclerotic lesions. Similarly, studies of healthy, long-term heavy cigarette smokers found cigarette smoking to be associated with impairment of endothelium-dependent arterial vasodilation and an impaired flow-mediated dilation (FMD) response.3,12 It is important to note that the subjects in these studies reported a history of heavier smoking (smoking average of 16 pack years3 and 25 cigarettes/day,12 respectively). In the present study, the subjects were younger and reported an average smoking history of 1.06±0.3 pack years. Therefore, the current study provides evidence that smoking-induced impairments of vascular function occur early after the onset of regular cigarette smoking, suggesting that even short-term chronic cigarette smoking has deleterious effects on cardiovascular health.
Furthermore, we have shown that cigarette smokers have a reduced magnitude of RH, indicating impaired function of the forearm resistance vessels. Our observations build on existing data showing impairment in large conduit arteries3,4,12 as well as the cutaneous13 and coronary14 microcirculation in older smokers. Importantly, this demonstrates that cigarette smoking results in a generalized impairment of vascular function and does not appear to be specific to any particular vascular bed.
While the current investigation was not designed to provide mechanistic insight, it has been postulated that the adverse effects of acute cigarette smoking on vascular health may result from oxidative damage to endothelial cells, since cigarette smoke contains superoxide and other reactive oxygen species.15 Oxidative damage to endothelial cells reduces the bioavailability of nitric oxide (NO), resulting in impaired endothelial function.15 Thus, it is biologically plausible that a reduction in NO bioavailability contributed to the reduced RH observed in short-term chronic cigarette smokers in the current study. Indeed, previous research has shown that NO contributes to post-ischemic vasodilation in the human forearm.16
Although the reactive hyperemic vasodilatory response is partially mediated by endothelium-derived NO,16,17 several other factors have been implicated as well. These include structural changes, prostaglandins, adenosine, membrane-bound ion channels, and direct smooth muscle function.18 Therefore, the measurement of RH is not solely endothelium-dependent, and results of the current study must be viewed within the context of the RH protocol employed. Furthermore, because the FBF response to an endothelium-independent vasodilator such as glyceryl trinitrate was not measured, we cannot rule out a difference in vascular smooth muscle function between groups. However, previous studies have shown that the vasodilator response to NO donors such as glyceryl trinitrate is preserved in cigarette smokers.3
In conclusion, the current study demonstrates that smoking-induced impairments of vascular function are apparent after a short history of regular cigarette smoking, underscoring the rapid onset of the negative effects of smoking on cardiovascular health. Furthermore, these results reinforce the importance of programs aimed to prevent or offset the negative effects of smoking on the cardiovascular health of young adults.
References
Cite this article
TY - JOUR AU - Brian R. Weil AU - Shannon A. Byrne AU - Tracy Baynard AU - Jill A. Kanaley PY - 2009 DA - 2009/07/14 TI - Vascular function is impaired early after the initiation of chronic cigarette smoking JO - Artery Research SP - 111 EP - 114 VL - 3 IS - 3 SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2009.06.025 DO - 10.1016/j.artres.2009.06.025 ID - Weil2009 ER -