
Rare chest pain causes by right bronchial artery
- DOI
- 10.1016/j.artres.2017.04.004How to use a DOI?
- Keywords
- Bronchial artery; Steal phenomenon; Computed tomogram
- Copyright
- © 2017 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Summary
A 42-year-old with diabetes mellitus presented with chest pain. During his initial presentation, he suddenly felt dyspnea with back pain. Physical examination was unremarkable and resting electrocardiography was normal. Serial myocardial enzyme examinations were normal. Therefore, computed tomography of chest, abdomen was performed evaluate the possibility of aortic dissection. The images showed enhancement of right bronchial artery arising from descending aorta (Fig. 1: axial view, Figs. 2 and 3: sequence images of coronal view). Patient later felt symptom relief and refuse further survey. The bronchial arteries supply the extra- and intrapulmonary airway, regional lymph nodes, bronchovascular bundles, as well as visceral pleura with nutrition and oxygenation. The angina-like symptom could result from coronary steal phenomenon through the vessel or rupture of brachial artery aneurysm.1 Moreover, some pulmonary diseases can trigger them to dilate and provoking angina or causing hemoptysis.2 In our case, the steal phenomenon could explain the brief chest pain with normal physical examinations and myocardial enzyme level. However, further coronary angiography is required to confirm the diagnosis. Advocating a lower threshold for use of computed tomography in assessment of unexplained chest pain should be a practical approach.
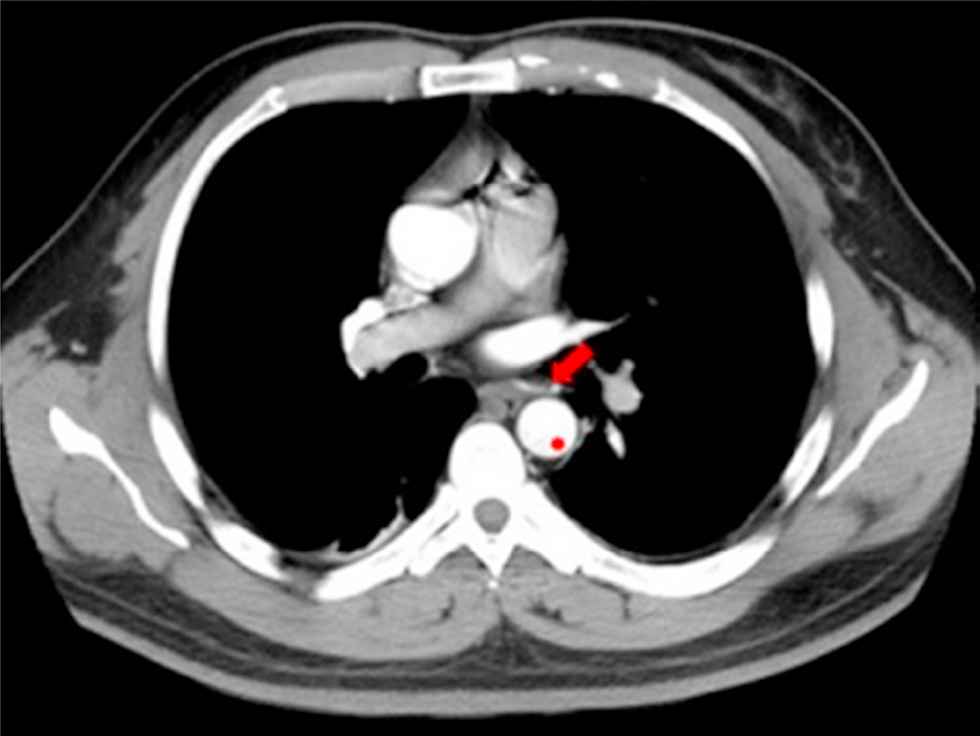
Computed tomography shows right bronchial artery (arrowhead) arising from descending aorta (asterisk).
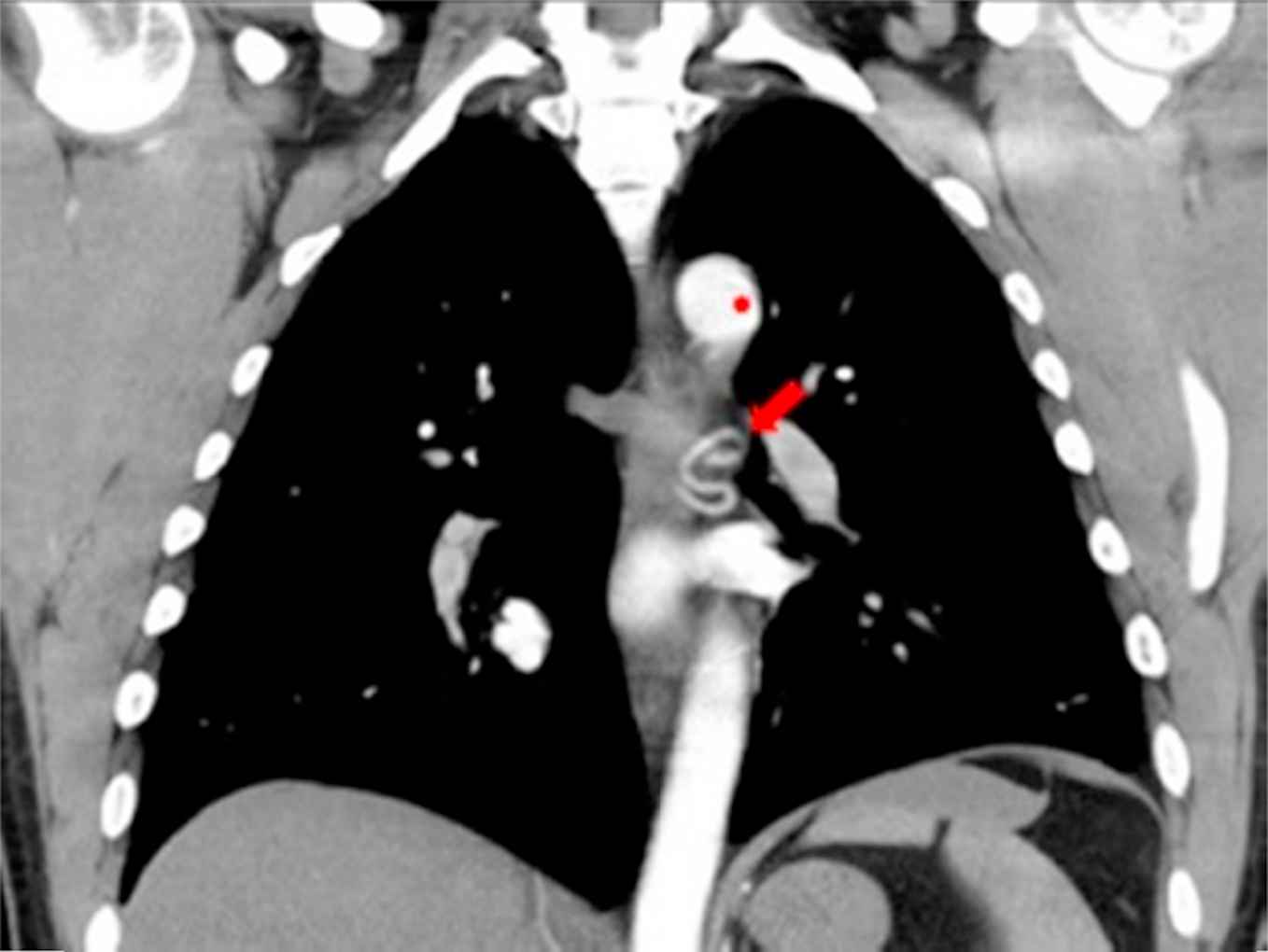
Sequence images of coronal view from computed tomography shows right bronchial artery (arrowhead) arising from descending aorta (asterisk).
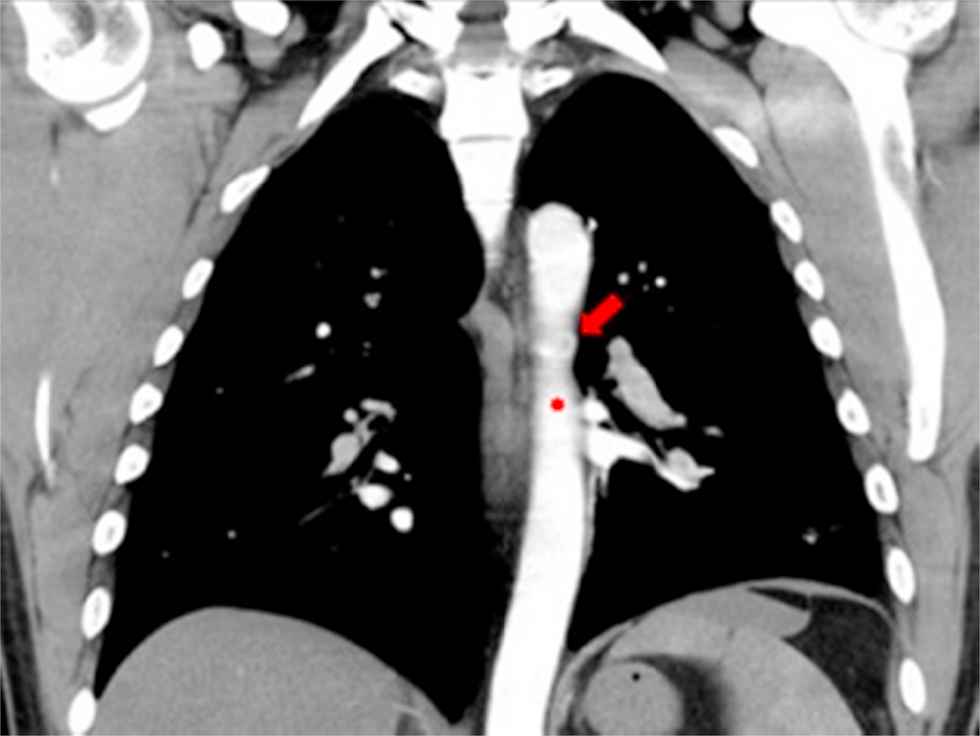
Sequence images of coronal view from computed tomography shows right bronchial artery (arrowhead) arising from descending aorta (asterisk).
Conflict of interest statement
All the authors declare that they have no competing interests.
Author’s contributions: Dr. Liu and Hsu made the substantive contributions to the design and drafting of the manuscript.
Cite this article
TY - JOUR AU - Ching Chih Liu AU - Yuan Pin Hsu PY - 2017 DA - 2017/04/21 TI - Rare chest pain causes by right bronchial artery JO - Artery Research SP - 64 EP - 65 VL - 18 IS - C SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2017.04.004 DO - 10.1016/j.artres.2017.04.004 ID - Liu2017 ER -